
Abstract
The purpose of this study was to determine the efficacy of inhaled epoprostenol for treatment of acute pulmonary hypertension (PH) in pediatric patients and to formulate a plan for a prospective, randomized study of pulmonary vasodilator therapy in this population. Inhaled epoprostenol is an effective treatment for pediatric PH. A retrospective chart review was conducted of all pediatric patients who received inhaled epoprostenol at a tertiary care hospital between October 2005 and August 2007. The study population was restricted to all patients under 18 years of age who received inhaled epoprostenol for greater than 1 hour and had available data for oxygenation index (OI) calculation. Arterial blood gas values and ventilator settings were collected immediately prior to epoprostenol initiation, and during epoprostenol therapy (as close to 12 hours after initiation as possible). Echocardiograms were reviewed during two time frames: Within 48 hours prior to therapy initiation and within 96 hours after initiation. Of the 20 patients in the study population, 13 were neonates, and the mean OI for these patients improved during epoprostenol administration (mean OI before and during therapy was 25.6±16.3 and 14.5±13.6, respectively, P=0.02). Mean OI for the seven patients greater than 30 days of age was not significantly different during treatment (mean OI before and during therapy was 29.6±15.0 and 25.6±17.8, P=0.56). Improvement in echocardiographic findings (evidence of decreased right-sided pressures or improved right ventricular function) was demonstrated in 20% of all patients. Inhaled epoprostenol is an effective therapy for the treatment of selected pediatric patients with acute PH. Neonates may benefit more consistently from this therapy than older infants and children. A randomized controlled trial is needed to discern the optimal role for inhaled prostanoids in the treatment of acute PH in childhood.
INTRODUCTION
Pulmonary hypertension (PH) is a complex disease with a heterogeneous group of etiologies in the neonatal and pediatric populations. The most common cause of acute pulmonary vascular crisis in children is persistent PH of the newborn (PPHN)—postpartum persistence of the high pulmonary vascular resistance of fetal life.[1] PPHN may be isolated but also occurs in association with meconium aspiration syndrome (MAS, 50%), pneumonia and/or sepsis (20%), as well as other disease states.[1–3] Congenital diaphragmatic hernia (CDH) is often associated with newborn PH, and these cases are complicated by pulmonary vascular hypoplasia.[4] Etiologies of PH after the first month of life include acute respiratory distress syndrome (ARDS), restrictive lung disease, obstructive sleep apnea-hypopnea, acute and chronic thromboembolic disease and pulmonary venous obstruction. Nonpulmonary causes include left-to-right intracardiac shunts, left heart disease, idiopathic PH (both sporadic and familial) and portal hypertension. Early treatment of PH regardless of etiology is crucial because advanced disease may be less responsive to therapy.[5]
Prostacyclin (PGI2) is an arachidonic acid metabolite formed by prostacyclin synthase in the vascular endothelium. PGI2 acts as a potent systemic and pulmonary vasodilator through induction of adenyl cyclase and increased formation of cAMP.[6] Intravenous PGI2 (epoprostenol sodium) is administered as a continuous infusion, both decreasing pulmonary artery pressures (PAP) and improving oxygenation in PPHN.[7] In addition, it has been used in pediatric patients with primary pulmonary arterial hypertension (PAH)[8] and PH acquired as a result of congenital heart disease.[9] Aerosolized or inhalational administration of epoprostenol offers the potential for more selective pulmonary vasodilatation with minimal impact on systemic systolic blood pressure (SBP).[10] In addition, ventilation/perfusion (V/Q) matching could be improved since lung units with the best ventilation will have more medication exposure. Use of inhaled epoprostenol for PPHN has been reported to improve oxygenation and decrease PAP by Doppler echocardiography without effects on SBP.[11,12] Improvements in oxygenation have also been demonstrated in a randomized trial of inhaled epoprostenol in children with acute lung injury (ALI).[13]
In our study, we retrospectively reviewed the effects of inhaled epoprostenol on oxygenation index (OI) in neonates and children who received inhaled epoprostenol for PH due to various etiologies in the pediatric and neonatal intensive care units of a tertiary care hospital.
MATERIALS AND METHODS
Study population
Following approval by the institutional review board, a retrospective chart review was conducted for all pediatric patients who received inhaled epoprostenol between October 2005 and August 2007. Potential study patients were identified as those having an order for epoprostenol in a computer-generated report from the pharmacy management system, GE Centricity. The study population was restricted to those patients under 18 years of age who received inhaled epoprostenol for at least 1 hour, and had data available for analysis of the OI before and during treatment. Patient information was deidentified and subjects were assigned arbitrary sequential study-related numbers.
Delivery of inhaled epoprostenol
All patients received inhaled epoprostenol via a MiniHeart Lo-Flo nebulizer (model number 100611, Westmed, Tucson, Ariz.). The nebulizer was connected to either the inspiratory limb of the ventilator circuit or to the BiPAP circuit for noninvasive ventilation, at a point as close as possible to the endotracheal tube or mask. The intravenous formulation of epoprostenol (Flolan) was reconstituted with sterile diluent supplied by the manufacturer, GlaxoSmithKline, and nebulized. The reconstituted solution of epoprostenol has a pH of 10.2–10.8 as the diluent contains glycine, sodium chloride, sodium hydroxide and water for injection. The epoprostenol was diluted for continuous nebulization at a rate of 8 ml/hr, and a dose of 50 ng/kg/min, or intermittently as 50 ng/kg diluted in 3 ml of diluent.
Outcome measures
There were two primary outcome measures: (1) proportion of patients with improved OI (defined as a 10-point or 20% decrease from baseline); and (2) proportion of patients whose echocardiographic data depicted improved PAP and/or right heart mechanics. There were six secondary outcome variables: (1) need for extracorporeal membrane oxygenation (ECMO); (2) deterioration of renal function; (3) deterioration of liver function; (4) sustained and significant drop in SBP; (5) worsening respiratory failure; and (6) death. For subgroup analyses of outcome measures, patients were subdivided a priori by age group (≤30 days vs. >30 days) and primary diagnosis.
Data collection
For each patient identified, the following data were collected manually from the electronic medical records (Eclipsys Sunrise Critical Care and the institutional Electronic Patient Record): Age and weight; admitting diagnosis; dose and duration of epoprostenol; and concurrent administration of other therapies for PH. Arterial blood gas values and ventilator settings were collected at two time points: The time prior and closest to epoprostenol initiation; and the latest available time point during the continued administration of epoprostenol up to 12 hours after initiation. Laboratory data including blood urea nitrogen, creatinine, AST, ALT, and bilirubin were collected during these time windows and following epoprostenol discontinuation.
Echocardiograms were reviewed during two separate time frames for each patient. The first window was within 48 hours prior to therapy initiation; the second window was within 96 hours after initiation. All echocardiograms were deidentified and reviewed by three blinded pediatric cardiologists. Echocardiographic data collected included the presence or absence of structural abnormalities and estimation of PAP and right ventricular (RV) function. Ten percent of echocardiograms were randomly selected for independent review by all three blinded cardiologists. Inter-rater reliability was analyzed for categorization of the parameters of RV function, RV dilation, and septal position.
Statistical analysis
Proportions were calculated for all outcome measures. Student's t-test for paired, parametric data (or Wilcoxon's nonparametric test) was used to compare pre- and post-OI continuous data. Chi-square or Fisher's exact was used to evaluate categorical variables. The null hypothesis was rejected with α=0.05, and P<0.05 was considered significant. Inter-rater reliability data were calculated for echocardiogram analysis. Data were presented as mean±SD for normally distributed data and median±interquartile range for non-normally distributed data.
RESULTS
Patient population
Twenty patients under the age of 18 years were identified that had received inhaled epoprostenol for greater than 1 hour and had OI data available for analysis, between October 2005 to August 2007.
Patient demographics, diagnoses, and outcomes are shown in (Table 1). The majority of patients (65%) were 30 days of age or less, and the most common admission diagnosis for this age group was MAS and/or PPHN (85%). The median age for all patients was 12 days (range 0 days to 15 years). All patients were treated with other pulmonary vasodilators concomitantly with the inhaled epoprostenol. All 20 patients received inhaled nitric oxide and intravenous milrinone, and 16 of the 20 patients received enteral sildenafil.
Baseline patient characteristics
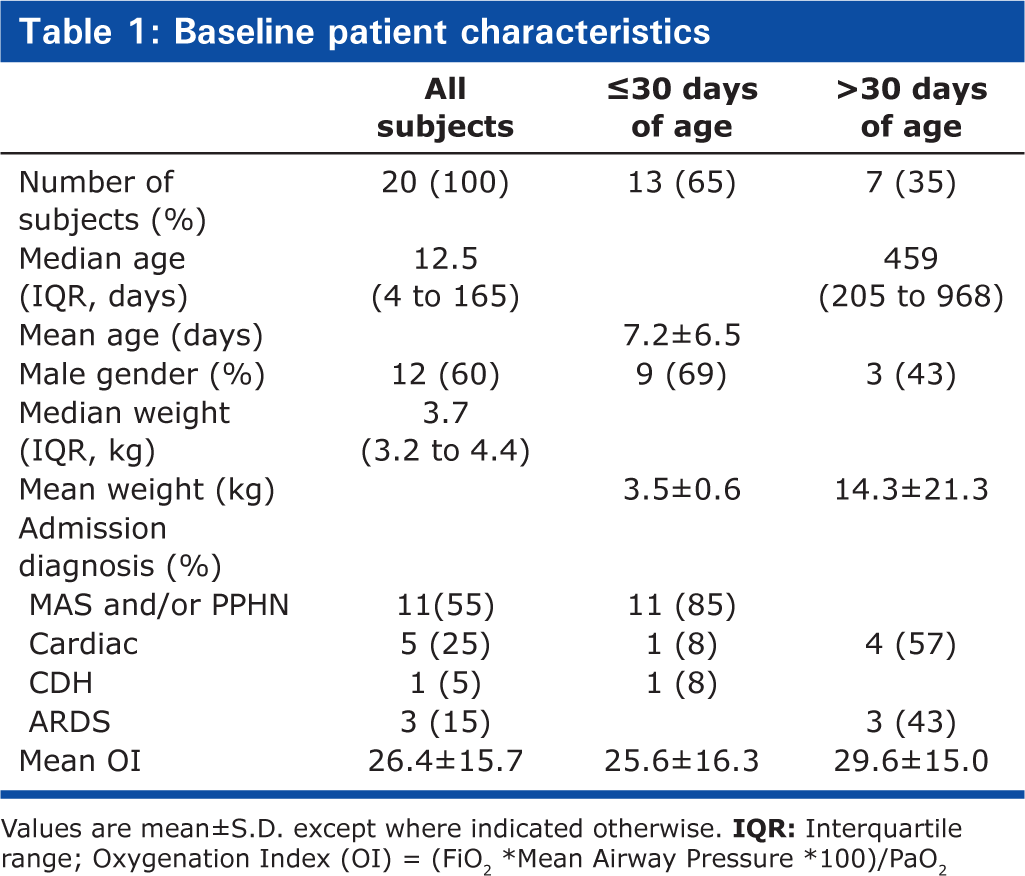
Values are mean±S.D. except where indicated otherwise.
The first patient to receive inhaled epoprostenol received intermittent nebulizations every 2 hours of 50 ng/kg. All subsequent patients in this series received continuous nebulization at a dose of 50 ng/kg/min. Patients received inhaled epoprostenol for an average of 7 hours and 14 minutes (range 3 hours to 630 hours.).
Oxygenation index
The mean OI prior to treatment for all 20 patients was 26.4±15.8 and the mean OI during treatment was significantly decreased to 18.6±16.1 (P=0.04). Of the patients, 13 were neonates and 7 were not. The mean OI prior to initiation of epoprostenol for patients less than 30 days of age was 25.6±16.3 and the mean OI during epoprostenol was 14.5±13.6, which represents a statistically significant decrease (P=0.02). The mean OI prior to treatment for patients greater than 30 days of age was not significantly different during and before epoprostenol administration (29.6±15.0 vs. 25.6±17.8, P=0.56; Fig. 1).
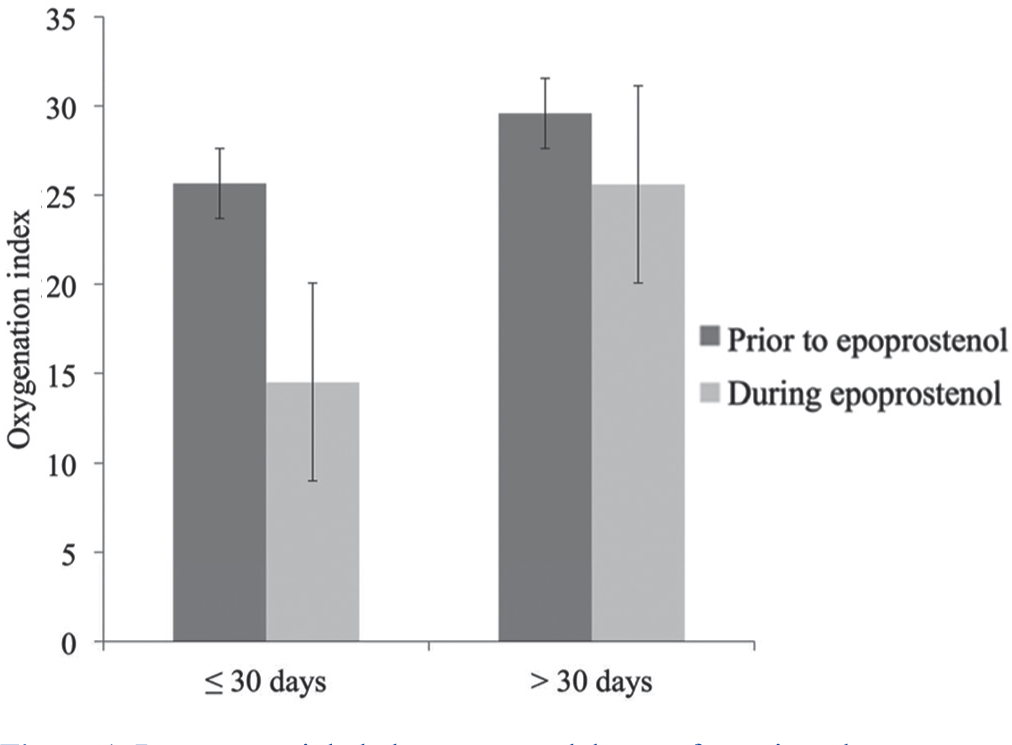
Response to inhaled epoprostenol therapy for patients by age group (less than 30 days of age vs. greater than 30 days of age). Mean oxygenation indices with standard error prior to therapy and during therapy are shown.
Echocardiographic data
Twelve patients had interpretable echocardiography data before and during therapy with epoprostenol. Four had improvement in either estimations of RV function or PAP on echocardiogram while on epoprostenol. Two had insufficient data for analysis, and 7 had no change. One patient had worsening RV function on echocardiography after epoprostenol initiation. Six patients were excluded from echocardiographic data review as they were on ECMO during echocardiography and outcome measures specific to epoprostenol could not be accurately evaluated. Twenty percent (4 of 20) had echocardiographic signs of improvement in RV function or decreases in PAP. Inter-rater reliability for individual indices was as follows: RV function, 97% agreement (90% CI: 0.890–0.995); RV dilation, 90% agreement (90% CI: 0.627–0.984); and septal position, 94% agreement (90% CI: 0.764–0.990). There was 95% agreement (90% CI: 0.905, 0.980) for analysis of echocardiographic data for all examined indices.
Subgroup analysis by diagnosis
There were five patients with congenital and/or acquired cardiac lesions. Three demonstrated improvement in OI with epoprostenol, two had no significant change in OI, and one had insufficient data with which to calculate the OI. For the five patients with data, the mean pretreatment OI was 23.8±20.3 compared to mean post-treatment OI of 18.2±15.3, which was not a significant change (P=0.18). Only one patient in the cardiac subgroup showed demonstrable improvement in RV function or PAP on echocardiography. Two patients had insufficient data for analysis.
There was no difference in mean pretreatment OI (31.3±6.6) and mean post-treatment OI (31.7 ± 21.5) for the three patients with ARDS (P=0.98). Echocardiographic data were available for analysis for two of the patients with ARDS: One showed no change and one showed worsening RV function.
The largest subgroup by diagnosis was the MAS/PPHN group. Mean OI during treatment (14.8 ± 14.6) was significantly improved when compared with mean OI prior to treatment (27.5 ± 16.5) for the 11 patients in this group (P=0.03). Two of the patients with MAS/PPHN had echocardiographic improvement, 4 had no change, and 5 were on ECMO and had echocardiograms that were not interpretable. (Fig. 2) shows the OI data by diagnostic subgroup.
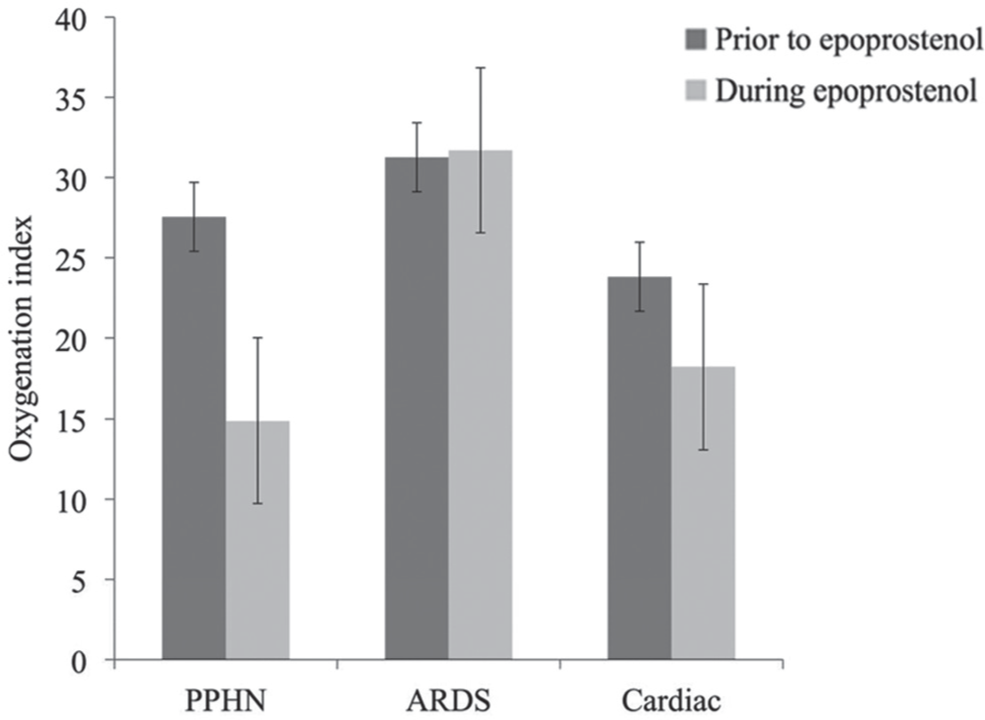
Response to inhaled epoprostenol therapy for patients by diagnosis. Mean oxygenation indices with standard error prior to therapy and during therapy are shown for each diagnosis.
ECMO data
Six patients (30%) in the study group were placed on veno-arterial ECMO during therapy with epoprostenol. Four of these patients received epoprostenol therapy prior to ECMO initiation. Three patients had improvement in OI, but were placed on ECMO based on other criteria. One patient had worsening of OI during administration of epoprostenol and was placed on ECMO. Two patients were started on inhaled epoprostenol while on ECMO. Both were subsequently weaned from ECMO and decannulated. As the patients were on ECMO, OI data could not be accurately determined.
Echocardiographic data for these two patients showed no change in RV function or PAP. However, medical records for both patients indicate that subjective improvement in RV function was noted during clamp trials following epopostenol initiation.
Potential side effects of therapy and mortality data
Six of 20 patients experienced at least one studied side effect during inhaled epoprostenol therapy. Five patients who experienced side effects were neonates. The most common side effect both during and after treatment with inhaled epoprostenol was a drop in SBP requiring fluid boluses or circulotropic drugs. The most common respiratory problem requiring brief interruption of therapy was transient difficulty with the nebulizer-ventilator interface—most commonly causing inconsistent mean airway pressure during high-frequency oscillatory ventilation. No patients experienced continued respiratory compromise after treatment cessation. No changes in renal function were documented. A neonate with undiagnosed total anomalous pulmonary venous return (TAPVR) experienced a decrease in SBP, worsening respiratory failure, and elevation of liver enzymes, but all of these resolved with surgical repair (and cessation of therapy). There were four patient deaths, none of which were directly attributable to epoprostenol.
DISCUSSION
In this retrospective analysis of 20 patients who received inhaled epoprostenol, we found a significant decrease in OI from 26.4±15.8 to 18.6±16.1 (P=0.04). Echocardiographic improvement in PA pressures or RV function was seen in 29% of patients who were not on ECMO. The majority of our patients were neonates with PPHN, and in subgroup analysis by age and diagnosis, significant improvement in OI was only noted in the neonatal group, and those with MAS/PPHN. ECMO was used for five neonates with MAS/PPHN in our series (45% of patients with this diagnosis)—a higher than expected rate of ECMO therapy for these diagnoses. This may be due to the fact that the majority of neonates in this study were referred to the PICU for consideration for ECMO therapy, so that our neonatal population may be more severely ill than average neonates with MAS/PPHN. We did not observe significant change in OI in patients greater than 30 days of age, infants and children with congenital or acquired heart disease or in children with ALI/ARDS (although we recognize that OI is not the best indicator of response to therapy in all of these patients).
Developmental and clinical factors could explain enhanced responsiveness to inhaled epoprostenol in the neonatal group with MAS/PPHN. A late gestation nadir in the expression and function of vasoactive compounds derived from the pulmonary endothelium may lead to discrete dysfunction of the pulmonary microcirculation.[14–17] Additionally, neonates with acute pulmonary endothelial injury may not mount the normal perinatal increase in endothelial nitric oxide synthase (eNOS) expression.[16] Further, diminished cGMP activity may occur due to both decreased expression of the paracrine eNOS-inducing agent VEGF, and by prenatally increased levels of phosphodiesterases 3 and 5.[14] A hypoxemic or acidemic perinatal event can then trigger a cascade of events and PPHN.[18] The principal dysfunction in this syndrome involves vasoactive pathways in the pulmonary circulation, and this may make these neonates ideal targets for direct pulmonary delivery of vasodilator therapy.
This study provides further evidence that inhaled prostanoids have a good safety profile in neonates, infants, and children, and adds momentum toward what is now needed most: A multi-institutional, randomized, controlled trial of inhaled prostanoids in children with acute PH in the ICU setting.[19,20] Three lessons gleaned from the experience of this study and the current literature will improve the design and impact of this future study. The first is early initiation of therapy. The initiation of therapy before all other options were exhausted led to the engagement of both cAMP and cGMP pathways to enhance pulmonary arteriolar smooth muscle relaxation, and both timing and strategic pharmacology may explain the efficacy of inhaled epoprostenol for those neonates that responded in the experience reported here. Inhaled epoprostenol needs to be started soon after the inadequacy of nitric oxide therapy for PH is suspected in order to decrease the need for ECMO and the risk of death. This underlines a second priority—early diagnosis. Careful protocols for echocardiography and more persistence in pursuit of adequate windows by trans-thoracic or trans-esophageal study may be needed. Consistent focus on right ventricular systolic and diastolic performance using the Tei index, tricuspid valve tissue annular excursion or volumetric three-dimensional analysis may also help to build consensus on a consistent diagnostic approach for PH in these patients.[21–23] Finally, the availability and efficacy of prostanoids specifically formulated for inhalation therapy may improve the consistency, reliability and safety of drug delivery, and further supports the need and feasibility of studying these agents in critically ill patients.[18,20,24,25] We hope that the present study and others like it will prompt a collaborative effort in pediatric critical care medicine and neonatology that will answer important questions about therapy for acute PH, providing a response to the urgent need for effective therapies for neonates, infants and children with this severe critical illness.[18]
In conclusion, inhaled epoprostenol may be an effective therapy for the treatment of PH and RV failure in selected subsets of the pediatric population. Our data indicate that neonates with PPHN with or without MAS showed significant improvement in oxygenation with this therapy, and this population therefore warrants priority consideration for further trials. Further study is needed that incorporates prospective, randomized and multi-institutional design, as well as consideration of whether this therapy best serves the target population as an early intervention option or as a rescue therapy.
Footnotes
ACKNOWLEDGMENTS
The authors thank the Department of Anesthesiology and Critical Care Medicine for support for this study, Elizabeth White for her invaluable assistance during the IRB approval process, Dave Ani for deidentification of the echocardiographic data to facilitate evaluation by the cardiologists, and Tzvi Ursuy for his work on the database.