
Abstract
Hairy cell leukemia (HCL) is a low grade B-cell lymphoproliferative disorder that typically presents with splenomegaly, cytopenias, and diffuse bone marrow infiltration. There have been few cases in the literature of HCL presenting as lymphomas in extra-nodal locations, such as soft tissues and bones without circulating leukemic cells, splenomegaly, or iliac crest bone marrow involvement. We present an additional case presenting as a thoracic mass, and discuss potential diagnostic pitfalls and management of these rare cases.
Keywords
Introduction
Hairy cell leukemia (HCL) is an indolent, mature B-cell lymphoproliferative disorder (B-CLPD) recognized by its near universal presentation of splenomegaly with splenic red pulp involvement, cytopenias with the frequent finding of monocytopenia, bone marrow infiltration with reticulin deposition, and identification of lymphocytes with non-polar, hair-like cytoplasmic projections in the peripheral blood. 1 There have been few previous reports of a lymphomatous variant of HCL, most frequently presenting as a marginal zone-like lymphoma without any other classic features, particularly a leukemic component. We report the fifth case in medical literature and discuss the potential diagnostic pitfalls of this rare entity.
Case Report
A 53-year-old white man developed left chest wall pain and a persistent cough. He had no associated B symptoms or shortness of breath. He had smoked one pack of cigarettes per day for 35 years. There was no family history of cancer. He had age appropriate recommended cancer screening and did not take any medications. A chest X-ray showed a left anterior chest wall mass, so he was referred to an oncologist.
His physical exam was unremarkable, without any lymphadenopathy or organomegaly. Laboratory testing that included a complete blood count, full chemistry, and a hepatic panel were unremarkable. A computed tomography (CT) scan of the chest revealed two anterior mediastinal soft tissue masses involving the pleura with extension to the chest wall; the larger mass measured 8.7 cm x 4.7 cm. A core needle biopsy of one of the chest wall lesions showed sheets of small to medium sized plasmacytoid lymphoid cells that stained positive for CD20, CD45, cyclin D1, and BCL2 by immunohistochemistry (IHC). There was weak cytoplasmic staining for kappa light chain. IHC staining was negative for keratin AE1/AE3, TTF-1, chromogranin, synaptophysin, CD3, CD5, CD10, and CD23, and CD138.
Fluorescence in situ hybridization (FISH) for BCL2, BCL6, c-Myc, CCND1/IGH [(t(11;14)], and MALT1 showed no rearrangement. Traditional cytogenetics of 20 metaphases revealed a normal 46 XY karyotype without clonal aberrations. Subsequent positron emission tomography (PET) imaging demonstrated uptake only in the chest wall masses, with a maximum standardized uptake value (SUV max) of 11.7 and 14.1. Bone marrow biopsy was unremarkable with normal trilineage hematopoiesis. Serology for hepatitis and HTLV1/2, protein electrophoresis, and lactate dehydrogenase were normal.
He was initially diagnosed as having low-grade marginal zone lymphoma based on the morphologic appearance and nonspecific staining pattern. He was treated with rituximab, cyclophosphamide, vincristine, and prednisone (R-CVP), but he had no response after 3 cycles; adriamycin was added (R-CHOP) for an additional 3 cycles. Subsequent PET-CT imaging showed no change in size or SUV of the lesions. This led to a repeat biopsy. The malignant cells were consistent with prior IHC staining, but they were also found to be diffusely positive for CD123 and CD200 (Figure 1 and Table 1), dimly positive for BCL-1, and negative for CD56, CD117, LEF1, SOX11, MUM-1, and BCL-6. The Ki-67 proliferation rate was 5%.
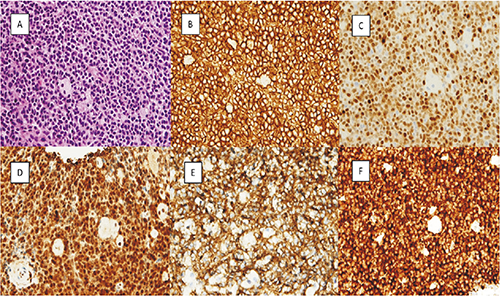
Diagnostic pathologic findings for lymphomatous presentation of hairy cell leukemia. All stains at 400× except BRAFV600E (F) at 600×. A. Hematoxylin & Eosin stain showing small to medium sized cells with interspersed histiocytes. Further positive stains including CD20 (B), cyclin D1 (C), annexin A1 (D), CD200 (E), and BRAFV600E (F). Diagnostic clues and confirmatory pathologic findings are listed in Table 1.
Diagnostic clues and confirmatory pathologic findings.

The patient was referred to our institution for a second opinion for primary refractory B-cell lymphoma. A comprehensive pathological review was performed. In terms of differential diagnosis, we considered marginal zone lymphoma and lymphoplasmacytic lymphoma on the basis of the lesions’ morphology and immunophenotype (CD5-, CD10-, CD23-); we also considered mantle cell lymphoma on the basis of cyclin D1 expression or a lymphomatous presentation of HCL on the basis of cyclin D1and CD200 expression in the absence of positive markers for chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL). Mantle cell lymphoma was ruled out by negative FISH testing for t(11;14). As cyclin D1 and CD200 are characteristically expressed in HCL, we performed further stains for HCL. This diagnosis was confirmed by strong expression of annexin A1 and BRAFV600E. Polymerase chain reaction (PCR) identified a BRAFV600E mutation but no MYD88 mutation. The patient was initiated on cladribine therapy with a single 7-day continuous infusion. 2 Evaluation four weeks after treatment revealed that he had achieved a partial response with near resolution of the chest wall masses and a reduction in the SUV max from 11.7 and 14.1 to 2.0 and 5.6, respectively.
Discussion
Although rare, the diagnosis of classic HCL (HCL-c) can reliably be made by recognizing a typical clinical and pathological presentation, but diagnosis can be challenging when presentation is atypical. HCL-c lymphoma cells tend to have a predictable pattern of immunohistochemical (IHC) staining, including bright staining for pan B-cell markers CD19, CD20, and CD22; positive staining for CD 11c, CD25, CD103 and CD123; and negative staining for CD5, CD10, and CD23. 1 Recently, the near universal prevalence of BRAFV600E mutation, identified by IHC staining and/or PCR analysis, has been reported as a diseasedefining feature 3 and can be used as a confirmatory test. However, a variant form of HCL (HCL-v), accounting for approximately 10% of all cases, with similar morphologic features but a different IHC staining pattern and a negative BRAFV600E mutation status has also been well described. This disease variant does not respond to cladribine therapy like HCL-c.4,5 Other unusual presentations of HCL-c involving non-lymphoid, non-reticuloendothelial tissue, 6 including bones, 7 soft tissues, 8 and the brain, 9 have also been reported; however, these have been in the setting of other classic clinical features of HCL. Occasionally, usually at advanced stages, HCL-c may involve lymph nodes, most often in the abdomen or retroperitoneum. 10 There have been few cases reported so far in the medical literature where HCL presents as an extra-nodal mass (soft tissue or bone), without cytopenias, splenomegaly, bone marrow involvement, or circulating hairy cells,11–16 as outlined in Table 2. As is the pattern with HCL-c, five of six patients published have been middle-aged males.
Comparison of reported cases of lymphomatous presentation of Hairy cell leukemia without involvement of bone marrow, splenomegaly, or cytopenias.

IHC: immunohistochemistry
The presentation of hairy cell lymphoma without leukemic phase, splenomegaly, or bone marrow involvement could morphologically mimic other nonspecific small to moderate sized B-CLPDs. It could have been misdiagnosed as a mantle cell lymphoma given weak cyclin D1 staining, though the lack of CCND1/IGH translocation excluded this possibility.
Morphologically, it may appear similar to a lymphoplasmacytic lymphoma, and rarely, it may even have associated paraprotein production; however negative results from MYD88 mutation testing can help exclude this. It could also be misdiagnosed as an atypical small lymphocytic lymphoma (SLL) due to the strong CD200 staining; however the remainder of the IHC stains lean toward an HCL diagnosis. CD200 can be used to help distinguish between chronic B-CLPDs, as it is strongly expressed in CLL/SLL and HCL, but less so in splenic marginal zone lymphoma and follicular lymphoma and weak to negative in other lymphomas. 17 Annexin A1 can also be used as a confirmatory test as it is highly specific to HCL, with specificity reported at 100%, although caution must be used in the interpretation of results because it can also stain myeloid and T cells. 18 Confirmative testing for BRAFV600E (exon 15) secured a diagnosis in our case, leading to effective treatment. In the rare event that this mutation is negative, one could consider testing exon 11 for alternate BRAF mutations. 19 Table 1 lists diagnostic clues and confirmatory tests.
Conclusions
Given the rarity of this entity, an accurate diagnosis can be challenging and pathologists and clinicians must maintain a high index of suspicion when confronted with a B-CLPD with an atypical staining pattern, especially if the tumor does not respond to the initial treatment. Patients respond predictably to treatment with infusional cladribine. In cases of incomplete response, relapse, or no response to treatment, clinicians can now also consider using the BRAF inhibitor vemurafenib. 20 Our case highlights and also questions the under-recognition of hairy cell lymphoma, which might masquerade as a refractory low-grade B-cell lymphoma and lead to ineffective treatment.
Footnotes
Acknowledgements
The auhtors would like to thank Scientific Publications for their assistance in manuscript preparation.