
Abstract
Oncocytic variant of medullary thyroid carcinoma (OV-MTC) is a very unusual entity, up to date only 17 cases have been reported in the literature. MTC is a neuro-endocrine malignancy arising from the para-follicular C cells of the thyroid gland. It generally has a slight female predominance and appears as a single lesion. However in the Multiple Endocrine Neoplasia Syndrome 2, linked to the point mutation of
Introduction
Oncocytic changes are common findings in benign as well as in malignant thyroid conditions. Oncocytic metaplasia is invariably detected in Hashimoto thyroiditis and can be observed in single follicular structures entrapped in lymphoid nodules as well as in the form of nodular follicular hyperplasia. Oncocytic variant of follicular adenoma may also occur. On the other hand well-differentiated thyroid carcinomas, both papillary and follicular types also have oncocytic variants.
Medullary thyroid carcinoma (MTC) is a relatively rare thyroid malignancy. It was first described by Hazard in 1959,
1
and currently represents 5-10% of all thyroid malignancies.
2
About 80% of MTC are sporadic, while 20% are linked to familiar conditions such as Familiar Medullary Thyroid Carcinoma and Multiple Endocrine Neoplasia Syndrome 2 (MEN2) as a result of the point-mutation of the
RET is an oncogene coding for a tyrosine kinase receptor also involved in a fraction of papillary thyroid carcinoma where
MTC seems to be closely related to C-cell hyperplasia. Two types of lesions can be recognised: a
Different variants of MTC have been described in the literature: papillary or pseudopapillary, glandular, giant cell, spindle cell, small cell, paraganglioma-like, clear cell, oncocytic, angiosarcoma-like, squamous cell, melanin producing and amphicrine. 6 Among these, the oncocytic variant, first described by Harach, 7 appears to be exceptional. In fact, only 17 cases have been reported so far. 8
The surgical and oncological therapy for MTC is consistently different from that required for well-differentiated thyroid carcinomas. For this reason it is important to recognize the oncocytic variant of MTC because it can be easily misdiagnosed.
Here we describe a rare case of sporadic multifocal and bilateral oncocytic variant MTC (OV-MTC), carrying
Case Report
A 75-year-old man underwent a neck eco-scan showing a thyroid goiter extending to the upper region of the chest cavity and dislocating the trachea. The thyroid showed a heterogeneous echo pattern with multiple confluent nodules with merging and undefined borders. Multiple enlarged latero-cervical lymph nodes were also detected bilaterally, but their morphological features were suggestive for an inflammatory origin.
Fine needle aspiration cytology of the prevalent thyroid nodule was performed elsewhere and a cytological report of benign thyroid condition (Thy-2 according to the British Thyroid Association) was provided. 9
Routine laboratory analysis including thyroglobulin level, TSH, FT3 and FT4 were in the normal range whereas calcitonin level was found to be 62.7 pg/mL (RIA normal range: 0-17 pg/mL). The patient revealed a family history for colorectal adenocarcinoma and underwent simple nephrectomy in the past years for renal cell carcinoma. During last last follow-up a magnetic resonance imaging (MRI) scan highlighted adrenal enlargement compatible with cortical nodular hyperplasia.
Because of symptoms and high serum calcitonin levels a total thyroidectomy with central nodal dissection was performed.
Grossly the thyroid appeared normal in shape, fairly enlarged (left lobe 6×3.5×2.5 cm, isthmus 2.5×1 cm, right lobe 7×3×2.5 cm). Cut sections showed the aspect of a colloid goiter with 5 whitish areas with irregular edges, 0.3-0.7 cm in diameter scattered in both thyroid lobes, which were sampled for histological examination. At histology a multinodular goiter (hyperplasia) was confirmed, but scattered neoplastic cells showing large eosinophilic and loosely granular cytoplasm, arranged in nests and in a trabecular fashion were detected bilaterally. Their nuclei showed salt-and-pepper-textured chromatin, enhancement of nuclear membrane and occasional prominent nucleoli. No alterations suggestive of PTC were visible (Figure 1A,B). All of the nine examined lymph nodes showed chronic reactive lymphadenitis.

A) Different neoplastic foci, arranged in sub-centimetric nodules, scattered in the thyroid parenchyma [haematoxylin and eosin (H&E), magnification 25×]. B) Neoplastic cells show large eosinophilic and loosely granular cytoplasm. Nuclei are characterized by salt-and-pepper-textured chromatin, enhancement of nuclear membrane and occasional prominent nucleoli (H&E, magnification 100×). C) Medullary carcinoma stained for calcitonin: there is extensive infiltration of the thyroid parenchyma by tumor cells (Indirect immunoperoxidase with calcitonin specific mAB, magnification 25×). D) Sustentacular cells occur within the nodules, embracing neoplastic cells (Indirect immunoperoxidase with S-100 specific mAb, magnification 100×).
Neoplastic oncocytic foci were immunoreactive for calcitonin, galectin-3 and TTF1. Immunostaining for S100 protein highlighted the substentacular cells located at the periphery of the neoplastic cell nests (Figure 1C,D). Congo Red histochemical staining did not show any amyloid deposition.
According to morphology and immunophenotype, a diagnosis of multifocal and bilateral oncocytic variant of medullary carcinoma was made.
Considering the co-existence of bilateral adrenal lesions revealed at MRI-scan, the possibility of a MEN syndrome was investigated. In order to exclude a genetic form of disease,
Since about 98% of patients with autosomal dominant heredity form of medullary thyroid carcinoma (MTC), known as multiple endocrine neoplasia type 2 (MEN2) presents hotspot mutations in exons 2, 5, 8, 10, 11, 13, 14, 15 and 16 of the
Oncocytic variant of MTC is very rare and considering the possibility of additional
Discussion
Oncocytic variant of medullary thyroid carcinoma is an extremely rare entity and only 17 cases have been reported in the literature until now. Nevertheless it appears oncologically relevant to recognize this entity, because it can be misdiagnosed with several benign oncocytic changes occurring in the thyroid gland.
Canberk S. and colleagues highlight how difficult can be to recognize the oncocytic variant of medullary thyroid carcinoma on cytological bases. 8 The morphology of neoplastic cells, the disposition like single cells or cell nests, presence of nuclei with clumping chromatin and inconspicuous nucleoli, lack of the typical nuclear features of papillary carcinoma, will arise a suspect of MTC that will be supported by serological (high serum levels of calcitonin) and immunohistochemical data, although very rare cases of MTC with abortive calcitonin secretion have been reported also. 12
In the present case the patient underwent fine needle aspiration-cytology for thyroid nodules classified as Thy2 (benign) in a regional hospital. This approach likely provided a cytological sampling of the prevalent thyroid nodules, whereas the neoplastic sub-centimetric multifocal lesions were missed.
Histologically, the most relevant diagnostic aspects were the multifocality and bilaterality of the lesion, which put the differential diagnosis between a multifocal and bilateral MTC oncocytic type or a focal neoplasia arisen in a context of multifocal C-cell hyperplasia with oncocytic changes, two entities which are difficult to be distinguished. 3
Even if the small dimension of the vast majority of neoplastic foci could lead to a diagnosis of C-cell hyperplasia, we rejected this hypothesis in consideration of the number of cells characterising each foci, the presence of cellular atypia and most important the common oncocytic phenotype among the neoplastic foci. The latter suggests a clonal multifocal expansion rather than the occurrence of common oncocytic change in scattered hyperplastic calcitonin producing cell aggregates. Moreover this case lacks of the mutation of
Oncocytic variant of medullary thyroid carcinoma reported in the literature.
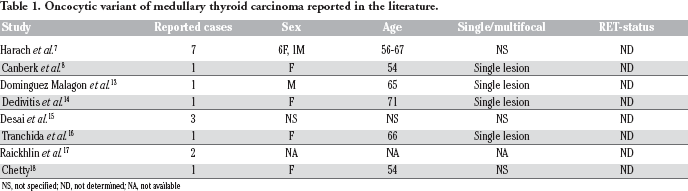
NS, not specified; ND, not determined; NA, not available
Conclusions
Oncocytic variant of MTC is a very uncommon thyroid malignancy, which is remarkably important to recognize in the spectrum of oncocytic lesions of thyroid gland. Future investigations are needed to evaluate the pathophysiology of oncocytic metaplasia in parafollicular C-cells hyperplasia and derived tumors.
Footnotes
Acknowledgements
The authors would like to thank AIRC Italian Association for Cancer Research that partially supported this work.