
Abstract
Outcomes of external beam radiotherapy (EBRT) in advanced medullary thyroid carcinoma (MTC) are largely unknown. Retrospective review of data from patients with MTC, diagnosed from June 1, 1970, through December 31, 2007. Overall survival and locoregional tumor control rates were calculated. Seventeen patients had adjuvant or palliative EBRT delivered to 41 sites. Six patients initially had adjuvant EBRT (median, 60.80 Gy); none had relapse in the treated area. Five patients with locoregional recurrence after surgery were treated (median, 59.40 Gy), and durable disease control was achieved in 3. Twelve patients received palliative EBRT to 29 sites of metastatic disease (median, 30.00 Gy), which provided sustained symptom relief at 45% of sites. Five- and ten-year overall survival rates were 44% and 19%, respectively. Adjuvant EBRT may be most effective for prevention of locoregional recurrence. EBRT may provide sustained control of advanced, metastatic disease in select patients.
Introduction
Medullary thyroid carcinoma (MTC) is a relatively rare malignancy that accounts for approximately 5 to 10% of thyroid cancers.1,2 Derived from the calcitonin-producing parafollicular cells, it arises sporadically in the majority of cases (80%) but also can occur in the context of multiple endocrine neoplasia syndromes.1,2
Appropriate initial treatment for MTC has long been considered to be total thyroidectomy and nodal dissection of the central compartment of the neck because up to 80% of patients with palpable disease will have nodal metastases.
3
Significant controversy remains regarding the practice of
Radiotherapy is sometimes offered as adjuvant treatment for advanced or invasive MTC; more often, it is used in a palliative setting for management of gross residual or recurrent disease. 4 However, there is a paucity of data regarding outcomes of radiotherapy, 1 the practice is controversial, and considerable uncertainty remains regarding indications for its use. Historically, some have viewed MTC as a radioresistant tumor, but recent series have questioned that notion.5–11
We sought to determine the effectiveness of external beam radiotherapy (EBRT) in the management of resected, recurrent, and metastatic MTC. We reviewed a cohort of patients with MTC who received adjuvant, salvage, or palliative EBRT at our institution.
Materials and Methods
After obtaining approval from the Mayo Clinic Institutional Review Board, we performed a retrospective review of data from all patients with MTC who were treated with adjuvant, salvage, or palliative EBRT at Mayo Clinic (Rochester, Minnesota, USA). All patients were diagnosed from June 1, 1970, through December 31, 2007. In accordance with Minnesota law, all living patients had authorized review of their medical records for research purposes before the study commenced. For patients treated with postoperative EBRT immediately following surgical resection and for patients treated with EBRT for unresectable locoregional recurrence, local disease control was defined as a complete response with no physical or imaging evidence of disease. The Kaplan-Meier method was used to estimate survival using JMP statistical software (version 8.0; SAS Institute Inc, Cary, North Carolina).
Results
Patient Characteristics
We identified 17 patients with MTC diagnosed during the study period. The median age at diagnosis was 48 years (range, 14-76 years). Median duration of follow-up was 3.4 years (range, 0.1-21.9 years). Adjuvant, salvage, or palliative EBRT was delivered to a total of 41 sites.
Adjuvant and Salvage External Beam Radiotherapy
Characteristics of the 11 patients receiving postoperative EBRT (adjuvant or salvage therapy) are shown in Table 1. Six patients received initial adjuvant EBRT to the neck, with or without inclusion of the mediastinum (median adjuvant dose, 60.80 Gy; range, 55.00-70.00 Gy) (Table 2). This occurred after surgery that was deemed
Characteristics of patients treated with locoregional adjuvant or salvage external beam radiotherapy (n=11).

Characteristic was determined at the initial surgery (
Treatment history and locoregional tumor control for patients receiving postoperative adjuvant or salvage external beam radiotherapy.

EBRT, external beam radiotherapy; NA, not applicable; ND, no data.
Treatment-specific information was not available (initial treatment was at another institution).
Patient died of an unrelated cause 5 days after completing EBRT.
Five patients were treated with salvage EBRT for locoregional recurrence after failure of initial surgery (median dose, 59.40 Gy; range, 35.00-70.00 Gy) (Table 2). For these 5 patients, disease status at the time of EBRT was considered not amenable to complete surgical removal. Margins at time of initial surgery were negative in 4 patients and unknown in 1 patient. Durable local disease control (complete response by physical examination and imaging) was achieved in 3 of the 5 patients. One patient died of an intracranial bleed unrelated to treatment 5 days after completing EBRT. Another patient received a total dose of 70.00 Gy to the neck to treat nodal recurrence after failure of initial surgery with negative margins. This patient ultimately had recurrence in the neck 54 months after salvage EBRT.
Palliative External Beam Radiotherapy for Metastatic Disease
Six of the 11 patients treated adjuvantly or for locoregional disease subsequently had metastases that were treated with palliative EBRT (17 sites). Six patients received only palliative EBRT for distant metastases (12 sites). The median palliative dose was 30.00 Gy (range, 19.80-50.00 Gy). This treatment provided documented, sustained relief of symptoms, with tumor control at 45% of irradiated sites (Table 3).
Treatment history and locoregional tumor control for patients receiving palliative external beam radiotherapy.
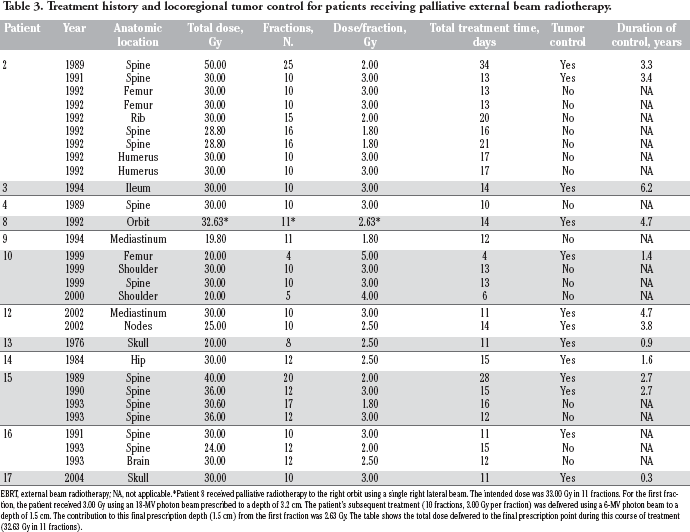
EBRT, external beam radiotherapy; NA, not applicable.
Patient 8 received palliative radiotherapy to the right orbit using a single right lateral beam. The intended dose was 33.00 Gy in 11 fractions. For the first fraction, the patient received 3.00 Gy using an 18-MV photon beam prescribed to a depth of 3.2 cm. The patient's subsequent treatment (10 fractions, 3.00 Gy per fraction) was delivered using a 6-MV photon beam to a depth of 1.5 cm. The contribution to this final prescription depth (1.5 cm) from the first fraction was 2.63 Gy. The table shows the total dose delivered to the final prescription point during this course of treatment (32.63 Gy in 11 fractions).
Survival
A Kaplan-Meier curve of overall survival (OS) is shown in Figure 1. The 5-year and 10-year OS rates were 44% and 19%, respectively. The median survival was 48 months. For the 6 patients treated with postoperative EBRT after the initial diagnosis or for salvage of locoregional recurrence (without evidence of distant metastasis at the time of EBRT), the median OS was also 48 months.

Overall survival of patients with medullary thyroid carcinoma who received external beam radiotherapy (n=17).
Discussion
In the setting of clinically apparent MTC, clinicians often recommend a total thyroidectomy with central neck dissection and either image-guided or prophylactic lateral neck dissection.1,4 Patients with locoregionally advanced disease have high risk of recurrence after surgery for MTC, as do patients with locally invasive or incompletely resected disease. Only a minority of patients with lymph node-positive disease has undetectable calcitonin levels after surgery with curative intent,
13
and locoregional recurrence affects up to half of patients with locally advanced or node-positive disease.
14
Grozinsky-Glasberg
The current analysis further supports the growing body of data on the efficacy of adjuvant EBRT after initial surgery and salvage EBRT after disease recurrence. We studied 11 patients who received adjuvant or salvage EBRT for advanced-stage disease, yet only 1 had locoregional relapse during follow-up. Five of the 11 patients had follow-up greater than 5 years, which underscores the durability of control achieved with postoperative EBRT. It was not uncommon, however, for patients to eventually have metastatic disease develop outside the treatment volume. Five of the 11 patients had distant metastasis at time of EBRT. Of the other 6 patients, 3 eventually received EBRT for palliation of metastatic disease.
Chemotherapy has historically shown little efficacy in MTC, and unlike differentiated thyroid cancer; radioiodine has not affected disease outcomes. Clinical trials of MTC are examining the effects of several systemic agents, including tyrosine kinase inhibitors and other novel agents,
1
and preliminary results are promising. Until such agents enter routine clinical practice, however, local palliative therapies, most prominently EBRT, remain important tools in the management of metastatic disease.
11
Furthermore, EBRT offers the opportunity to manage symptoms in patients with distant spread of disease. In our experience, EBRT was not as effective in this setting, although many patients benefitted from improved symptom intensity and durable control of tumor growth at treated metastatic sites. Our study was limited by the inherent challenges of its retrospective design and by the lack of adequate, consistent documentation of symptoms such as pain over the almost 40-year study period. We did not attempt to evaluate any association between calcitonin levels and outcome, although this has been extensively studied elsewhere.15,17 We also did not have sufficient data to identify risk factors associated with locoregional failure, which could be used to better identify the patients who might benefit most from postoperative EBRT. Toxicity information was not consistently recorded in our patient group, but others have observed the relatively low toxicity of EBRT in the adjuvant or salvage setting; Schwartz
Patients with MTC potentially may survive for several years, even after development of metastatic disease (the 5-year OS in our patient cohort was 44%). With such longevity, locoregional control is important for improving quality of life. Some clinicians at our institution have raised concern about the possibility of postoperative EBRT making future surgical interventions more difficult. However, adjuvant EBRT may have the benefit of obviating the need for further locoregional surgical interventions, especially in high-risk patients. In our patients, adjuvant EBRT after the initial surgery effectively eliminated the need for subsequent surgery. Thus, continued recommendations for EBRT seem justified. Patients with high-risk features (
Conclusions
Medullary thyroid carcinoma appears to be a radiosensitive tumor. EBRT may be most effective in the adjuvant setting for the prevention of locoregional recurrence, but it may also have a role in providing durable and sustained control of locoregionally advanced or metastatic disease (or both) in select patients.
Footnotes
Acknowledgements
This paper was presented as a poster at the World Congress on Thyroid Cancer, Toronto, Canada, August 6-10, 2009.