
Abstract
Cardiac sarcomas are extremely rare primary malignant tumors of the heart. In this article, we present the case of a 70-year-old female, who was found to have a left atrial mass during a routine outpatient transthoracic echocardiography. Further investigation with cardiac magnetic resonance imaging confirmed the presence of a bilobulated mass with heterogeneous enhancement. Left atrial myxoma was the first diagnostic consideration, followed by other primary cardiac tumors, and thrombus. The patient subsequently underwent resection of the mass, utilizing cardiopulmonary bypass. Upon pathological examination, the mass was found to be an intimal sarcoma. The objective of this report is to describe a case of this rare disease entity, and to discuss its presentation, pathological findings and management.
Case Report
A 70-year-old female with past medical history of hypertension, gastroesophageal reflux disease, atrial fibrillation, and supraventricular tachycardia presented to her cardiologist's office for a routine follow-up visit. In addition to these co-morbidities, she also had a previous history of smoking. Her home medications included 200 mg of labetalol twice daily, 5 mg of apixaban twice daily, and a combination pill of trimaterene 75 mg and hydrochlorothiazide 50 mg once daily. Routine transthoracic echocardiography was performed during her outpatient visit, which revealed the presence of a left atrial mass. The patient was subsequently referred for a contrast enhanced computed tomography (CT) scan to further visualize the mass. The scan revealed a well-circumscribed mass within the left atrial cavity. Differential diagnosis included atrial myxoma, other primary cardiac tumor or less likely, a thrombus.
The patient was subsequently hospitalized for further management. Cardiac magnetic resonance imaging was performed using a 3T scanner. Images were obtained before and after the administration of 40 mL of gadolinium contrast. These images revealed that the atrial mass was bilobulated and measured about 5.8×3.4×4.9 cm. The mass was also noted to have increased T2 signal with heterogeneous enhancement and cause obstruction of bilateral inferior pulmonary veins (Figure 1). A collaborative decision was taken to proceed with the resection of the mass. Cardiac catheterization was performed prior to proceeding with the resection in order to determine the patient's need for coronary artery bypass grafting. The procedure was performed using a radial artery access without any complications. No significant coronary artery disease was visualized. The patient underwent resection of the left atrial tumor two days later using cardiopulmonary bypass (CPB) and cardioplegic arrest. An intraoperative transesophageal echocardiography performed prior to placing the patient on CPB revealed a 4×3.47 cm bilobed left atrial mass attached to the interatrial septum and posterior wall of the left atrium. A right atriotomy was used to expose and incise the interatrial septum and fossa ovalis. The tumor was glistening white, hard, smooth, bilobed, and adherent to the left side of interatrial septum, but not invading fossa ovalis such that only a limited resection of the fossa was required. The invasive origin of the tumor was located on the posterior free wall of the left atrium, which was resected circumferentially en bloc with the tumor. The tumor did not appear to invade any major blood vessels. Patient did not have any significant postoperative complications and was subsequently discharged to a skilled nursing facility on postoperative day number 7.

Two chamber post-contrast cardiac magnetic resonance imaging revealing the left atrial mass.
The patient's resected cardiac mass was sent for pathological examination in formalin. The macroscopic appearance of the mass was solid and polypoid, and measured 4.5×4×3 cm. It had a smooth outer surface and cut surfaces revealed a 3 mm thick capsule, and a central white-yellow fleshy area in a whorled pattern with a focal area of gelatinous appearance (Figure 2). Histologically, the specimen showed a hypercellular cytologically malignant spindle cell neoplasm with fascicular growth pattern and areas of necrosis. The tumor cells showed pale eosinophilic cytoplasm, and tapering, variably hyperchromatic nuclei with readily identifiable mitotic figures. On hematoxylin and eosin exam, the tumor showed close resemblance to a smooth muscle neoplasm (Figure 3). No convincing lipoblasts were identified. Immunohistochemical stains showed focal positivity for alpha smooth muscle actin (a-SMA), and multifocal positivity for murine double minute 2 (MDM2) (Figure 4) and pan keratin. In light of strong MDM2 positivity, a fluorescent in situ hybridization was performed which confirmed the presence of MDM2 gene amplification (Figure 5). Positivity was also noted for desmin, Ki-67 (>20%) and CD68. The case underwent expert consultation and interdepartmental review. A diagnosis of intimal sarcoma was made. The positivity for SMA and desmin in this context may reflect myofibroblastic differentiation. Adjacent atrial muscle wall and resection margins were free of tumor.

Resected polypoid appearing left atrial mass.

A) Spindle tumor cells in fascicles with nuclear pleomorphism and mitotic figures; B) spindle tumor cells in fascicles with prominent necrosis; C) tumor cells with chondroid differentiation; D) tumor cells with myxoid change.
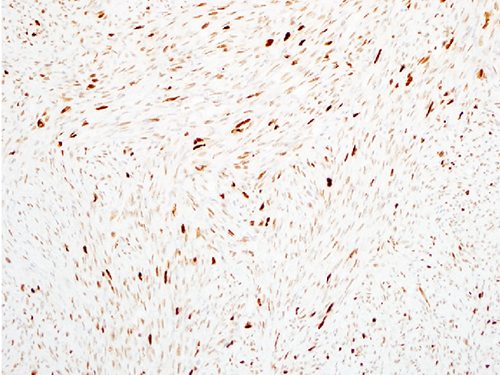
Immunohistochemical study showing multifocal positivity for MDM2.
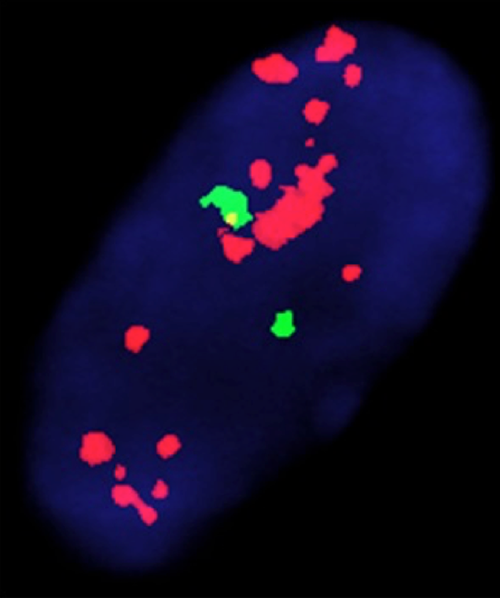
Fluorescent in situ hybridization (FISH) study showing MDM2 gene amplification. (MDM2/CEP12 FISH assay: MDM2-red signals, CEP12-green signals).
Patient had no evidence of metastatic disease on any of the initial scans performed as a part of her staging work-up. About 3 months later, a repeat CT abdomen-pelvis revealed widespread metastatic lesions involving the peritoneum, liver, kidneys, and the adrenal glands. CT chest revealed metastatic lesions in both the lungs along with axillary and thoracic adenopathy. Additionally, widespread metastatic lesions involving thoracic and lumbar spine were also noted on these scans. Patient had a detailed discussion with her oncologist regarding her prognosis and the various treatment options. She opted to undergo chemotherapy for her metastatic disease. A decision was taken to start the patient on docetaxil and gemcitabine regimen.
Discussion
Cardiac tumors have been reported since the early 16th century. However, due to their rarity, primary cardiac tumors continue to pose a challenge to physicians. Studies based on the autopsy findings have suggested an incidence of 0.001 to 0.056%, with approximately three quarters being benign and nearly half of those being myxomas.1,2 In an analysis of 12,485 autopsies, metastasis to the heart was found to be much more common than the primary tumors, and had a prevalence of 1.23%. 1 As non-invasive diagnostic modalities have become increasingly sensitive and readily available, a significantly larger number of patients are being diagnosed with cardiac tumors. 3
Differential diagnosis of an intracardiac mass is broad, and includes thrombi, benign tumors, primary malignant tumors, and secondary (or metastatic) cardiac tumors. As mentioned earlier, 75% of the cardiac tumors are benign, and atrial myxoma is the commonest subtype. Other common benign tumors include fibroma, fibroelastoma, lipoma, teratoma, and hamartoma. On the other hand, sarcomas are the most frequently encountered primary malignant cardiac tumors. Different histological subtypes of cardiac sarcomas include, but are not limited to angiosarcoma, leiomyosarcoma, fibrosarcoma, rhabdomyosarcoma, synovial sarcoma, osteosarcoma, undifferentiated pleomorphic sarcoma, and intimal sarcoma. Other extremely rare primary malignant tumors include lymphoma, paraganglionoma, and plasmacytoma.
Intimal (spindle cell) sarcoma is a mesenchymal tumor that is more commonly encountered in the great vessels and pulmonary veins. It rarely involves the heart. To our knowledge, only seven cases have been reported till date.4–10
Cardiac sarcomas can present in a number of ways and are known to be great mimickers of other conditions. 2 Patients may often remain asymptomatic until the advanced stages. In our case, the patient was largely asymptomatic, and the mass was seen on transthoracic echocardiography that was performed as a part of her routine follow-up. Symptomatic cardiac sarcomas usually present with dyspnea, orthopnea, paroxysmal nocturnal dyspnea, or lower extremity edema.5,8 Patients can also present with the features of metastatic disease in advanced stages. 7
Intimal sarcomas are poorly differentiated malignant tumors characterized by the formation of tightly packed spindle shaped cells with fascicular growth pattern, and often show areas of necrosis. These tumors can frequently resemble smooth muscle neoplasms such as leiomyosarcoma, just like the one in our report. 7 They exhibit variable degrees of necrosis, cellular atypia and nuclear polymorphisms, and rarely show areas with morphological features similar to angiosarcoma, rhabdomyosarcoma, and osteosarcoma.7,11 It was believed that angiosarcoma and undifferentiated pleomorphic sarcoma were the most frequently occurring cardiac sarcomas. However, in a recent study, intimal sarcoma has been reported as the most frequently occurring primary cardiac sarcoma (42%) with MDM2 gene amplification being its characteristic pathological feature. 12 Immunohistochemical analyses of these tumors typically show positive reactivity for MDM2, osteopontin and vimentin. Variable positivity is seen for -SMA, desmin, CD117, CD68, P53 and BCL-2. CD31, CD34, and Factor VIII are typically negative, but may be positive in areas with angiosarcomatous differentiation.7,13
The prognosis of cardiac intimal sarcoma is generally poor. Factors that are associated with worse prognosis include necrosis, high mitotic count, and metastasis.11,13 Another important factor determining the prognosis is the anatomical location of the tumor within the heart (intra-cavitary vs. intramural). It has also been found that the left sided tumors usually carry a better prognosis than right-sided tumors.11,13
Due to the frequent involvement of vital structures and early metastasis, cardiac sarcomas are associated with high mortality and morbidity. Intimal sarcomas are highly aggressive with the mean survival being 3 months to 1 year, although survival up to 11 years has been reported. 9 Patients with complete tumor resection are known to live twice as long as those without the surgical resection. 11 Thus, early diagnosis and complete resection are of paramount importance in the management of intimal sarcomas.
Although the achievement of tumor free margins with surgical resection is the mainstay of treatment in cardiac sarcomas and associated with improved survival, it is important to understand that surgical resection may not be possible in almost 50% of the cases due to the involvement of vital structures. However, in a recent study, about 65% of the patients with planned surgical management could undergo complete resection. 14 Furthermore, local recurrence and metastasis occur frequently and early, usually within 1 year. 13 Thus, there is a role for other treatment modalities such as chemotherapy and radiation therapy in the management of cardiac sarcomas. Ifosfamide-epirubicin (or doxorubicin) and CyVADIC (cyclophosphamide, vincristine, doxorubicin, and dacarbazine) are the two main regimens used in adult soft tissue sarcomas, and may confer survival advantage in patients with cardiac sarcomas as well. 13 Two meta-analysis have demonstrated that adjuvant chemotherapy improves the time to local and distant recurrence as well as the overall survival.15,16 The addition of ifosfamide further improves these benefits, but these should be weighed against the toxic effects arising from its use. 16 Gemcitabine based chemotherapy regimen (single agent or in combination with docetaxil) may also be tried in patients with cardiac sarcomas based on the favorable response to these drugs in various trials evaluating their role in the treatment of soft tissue sarcomas.17,18 Apart from the conventional chemotherapeutic regimens, there could also be a role for tyrosine kinase inhibitor pazopanib in the treatment of advanced disease, especially in those with poor response to the abovementioned drugs. Pazopanib was approved in the United States in 2012 for treating patients with advanced soft tissue sarcomas who had received prior chemotherapy, based on the data from PALETTE trial. 19
Conclusions
Cardiac intimal sarcoma is a rare, but aggressive disease entity with poor prognosis. Owing to its variable presentation, diagnosing this entity could be very challenging, and requires a high degree of suspicion while encountering patients with characteristic findings on the imaging studies. Although surgical excision with tumor free margins is the mainstay of treatment, complete surgical excision may often not be possible because of the involvement of the vital structures. Owing to the high rates of recurrence and metastasis, adjuvant chemotherapy must be used in all the patients diagnosed with this disease. Finally, it cannot be stressed enough that early diagnosis and prompt treatment are extremely crucial in improving outcomes in patients with this tumor.