
Abstract
Solitary bone plasmacytomas are part of a wide range of monoclonal neoplasms that share a common progenitor in the B lymphocyte lineage. In their particular case, a single bone lesion is found, most frequently on the axial skeleton, having evidence of no other osteolytic lesions or systemic involvement. Diagnosis can sometimes prove to be difficult as they are rare tumors, occurring in 3 to 5% (up to 10% in some series) of patients with plasma cell neoplasms, with important considerations regarding the differential diagnosis. We report a case of a solitary bone plasmacytoma, found on the ala of the left ilium of a patient during a routine consult due to hip pain.
Case Report
A 54-year-old woman, with medical history of hypertension, type II diabetes, dyslipidemia and osteoarticular degenerative disease of the spine already being studied at our institution, was admitted to our emergency department complaining of bilateral hip pain following a minor trauma. Radiographic studies performed showed no fractures or apparent bone lesions. One week later, after having sustained a fall from her own height, the patient was admitted again to the emergency department. At this time, and having worsening of the complaints, another set of radiographic studies were performed and showed fracture of the right ischiopubic and iliopubic rami, as well as a large osteolytic lesion on the left ilium ala (Figure 1). Conservative course of treatment was decided for the fractures and the patient was referenced to the outpatient consult at our institution to have the lesion studied. A CT was performed and confirmed the lesion suspected on the x-rays. Besides the iliopubic and ischiopubic fractures on the right pelvis already known, MRI showed a solid large mass extending from the left ilium to the left sacroiliac joint, with approximately 13.4×13×8.9 centimeters wide, with necrotic areas (Figure 2). Bone scintigraphy could not characterize better the lesion but excluded other bone lesions. The patient was referenced to the hemato-oncology specialist. Bone marrow biopsy showed no involvement by clonal cells. Histopathologic studies confirmed the diagnosis of solitary bone plasmacytoma of the pelvis (Figure 3) and radiotherapy cycle was initiated.
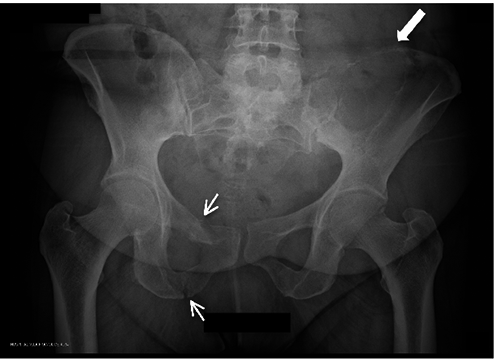
Radiography: small arrows showing fracture of the right ischiopubic and iliopubic rami; large arrow: large osteolytic lesion on the left ilium ala.

Magnetic resonance imaging: arrows pointing to solid large mass extending from the left ilium to the left sacroiliac joint, with approximately 13.4×13×8.9 cm wide. A) T1-weighted coronal view; B) T2-weighted coronal view; C) T1-weighted axial view; D) T2-weighted axial view; E) T1-weighted sagittal view.
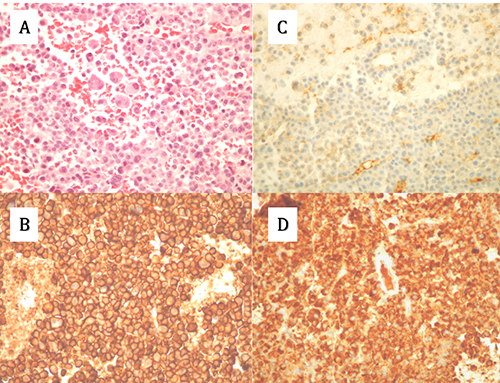
Histologic features of plasmacytoma. A) Sheets of well-differentiated plasma cells (Hematoxylin and eosin 400×). B) CD 138+ staining (400×). C) Absence of kappa light-chain expression (400×) D) lambda light-chain positivity (400×).
Discussion
Plasmacytomas take part on a vast group of clonal disorders that affect plasma cells. These disorders also involve other types of neoplasms that, due their common origin, make their characterization difficult. 1 The site of tumor and the presence of systemic manifestations can usually, but not always, point the type of tumor present. Solitary plasmacytomas can be classified into 2 groups according to their location: solitary bone plasmacytomas (SBP) – affecting the skeletal system – and extramedullary plasmacytoma (EMP) affecting virtually every lymphoid tissue, being more frequent in upper respiratory tract.1–4 Over the last decades, clinical data recognized specifically SBP and other unusual monoclonal gammapathies like EMP as different identities, with proper clinical presentation, specific diagnostic criteria, treatment strategies and prognosis.1,5,6 Nonetheless, clinical aspects overlap, thus making directed diagnostic and therapeutic strategies difficult. Importantly, SBP are more prone to evolve to multiple myeloma (MM) than EMP, thus having a poorer prognosis. 7
Population-based data about SBP are sparse although all studies refer to them as uncommon tumors, occurring in 3-5% of patients with plasma cell neoplasms (in some western series up to 10%).
6
Comparing to MM, SBP are sixteen times less frequent and the incidence of EMP is 40% lower than SBP.
8
Regarding SBP, males are twice likely to be more affected than females (65%
Clinically, at presentation, the most common symptom is pain at the site of the bone lesion, due to destruction,1,9 although sometimes asymptomatic disease can be found in routine radiographic tests or when soft tissue extension of the lesion produces a palpable mass. Regarding the site of lesion, involvement of the axial skeleton is more likely than the appendicular skeleton (83%
In face of clinical suspicion, some criteria must be followed to make the diagnosis: i) single area of bone destruction due to clonal plasma cells; ii) normal marrow without clonal disease; iii) normal results on a skeletal survey and magnetic resonance imaging of the spine, pelvis, proximal femora and humeri; iv) no anemia, hypercalcemia, or renal impairment attributable to myeloma; v) absent or low serum or urinary level of monoclonal protein and preserved levels of uninvolved immunoglobulins, 9 although recent criteria may include a small M-component that can be present in serum or urine in 50% of patients. 1
Besides the above criteria of diagnosis, imaging studies play an important role in the diagnostic, treatment considerations and prognostic aspects. A recent retrospective series of 10 patients with histological confirmation of SBP of the pelvis, analyzed the correlation between CT, MRI and histopathologic features. 10 Although few patients were analyzed (with 50% cases affecting the ilium), this study found a correlation between imaging characteristics and histopathologic grade, with superiority of CT on characterizing the type of bone destruction and concordance with histology findings, and MRI with better value as a prognostic method for reexamination after radiotherapy.
Course of treatment has been discussed over the last decades, with consensus of local radiotherapy as first line option. Correct dose of radiation has yet to be established, although most studies found good response with local radiotherapy at doses of 3500-4500 cGy (4000 cGy for vertebral lesions). Higher doses can produce toxic effects without proved therapeutical benefit. 9 Monitorization of M-protein (when present) was proposed as a marker of therapy response as it could predict the progression to MM, 13 although many patients maintain long-term stability even with M-protein persistency after radiotherapy.1,6,9 Imaging methods, particularly MRI can have a role in evaluating therapy response. Besides radiotherapy, some patients (particularly those with vertebral involvement), can show neurological impairment due to vertebra instability or pathological factures with compression of the spinal chord and/or its roots, and may benefit of surgical fixation. 9 Adjuvant chemotherapy has been discussed, with some authors defending less progression rate to MM, 14 although others found no other differences either than a lesser time to MM diagnosis. 15 However, most studies did not find beneficial effects of adjuvant chemotherapy, and in fact can raise problems with systemic toxicity and appearance of resistant clone cells. 16
Age is an important prognostic factor. Older age at the time of diagnosis has a striking effect on 5 year-survival according to most studies. Patients younger than 60 years appear to have a better prognosis. Size of tumor (solitary plasmacytomas >5 cm) appear to have a greater conversion to MM. 17 Progression to MM, can occur (being this rate increased in advanced age, especially in SBP when comparing to EMP), although this is not common, especially if radiotherapy provides good response. Indeed radiotherapy may prevent local relapse in 90% of patients, 18 although it has been described that progression to overt MM can occur in 50% of patients but taking approximately 15 years to do so. 1 When progression occurs earlier on the course of disease, subclinical myeloma should be suspected as present at the time of the initial diagnosis. 9 On the other hand recurrent solitary plasmacy-tomas (other bone lesions with no evidence of MM) can occur in up to 5-10% of patients. Reported in most series, 10-year survival is about 50%, being 25-40% of patients disease free at that time.
Recent studies did not found survival differences regarding location (axial
Conclusions
Solitary bone plasmacytomas are rare tumors, and their diagnosis can be challenging even by experienced professionals. Clinical presentation can often mislead on the pursuit of the correct diagnosis. Pelvic involvement by these tumors has been rarely described in the literature. The presentation of this case should make awareness on the occurrence of these neoplasms for prompt diagnosis and initiation of treatment.