
Abstract
We report the case of a young man diagnosed with dermatofibrosarcoma protuberans lung metastases seven years after primary tumor resection. Notably, no previous local recurrences had been observed. A multimodal approach was used for the management of this patient: surgery, radiotherapy and targeted therapy with Imatinib. The patient is alive with stable disease after thirty months of the metastases diagnoses. Dermatofibrosarcoma protu-berans metastasizes very rarely, and when it does, it is usually either after local recurrence or whenever fibrosarcomatous transformation is found in the histopathological analysis, which confers an increased risk of local recurrence and metastases. This is the second report of a metastatic dermatofibrosarcoma protuberans occurring in a patient with no previous local recurrence or histological fibrosar-comatous features, emphasizing the rarity of the disease presentation and the importance of targeted therapy in improving patient quality of life and survival.
Introduction
Dermatofibrosarcoma protuberans (DFSP) is a rare cutaneous soft tissue sarcoma of the skin. 1 It constitutes 0.1% of all cancers and 1% of all soft- tissue sarcomas. 2 It frequently recurs locally, but it rarely metastasizes. Recurrence rate has been reported as high as 60%1,2 but it decreases to less than 10% after wide local excision. Metastases occur only in 0.5-5% of the cases, usually after repeated local recurrences, being the most common sites lung, bones and regional lymph nodes. 3
Whenever histological features of fibrosarco-matous transformation are found in the surgical specimen, the likelihood of recurrence and metastases significantly increases. 2
Surgery is the treatment of choice for primary DFSP, local recurrences and metastases. Moreover, DFSP has been described as a radiosensitive tumor; local tumor control has been reported in up to 84% of patients when radiotherapy is used in the adjuvant setting. 4 More than 90% of DFSP cases are characterized by the presence of a t(17;22)(q22;q13)(COL1A1/PDGFB), which causes overexpression of the PDGF-β receptor. Therefore, imatinib can be used to inhibit PDGF-β activity in patients with a translocation bearing tumor. 5 In this line, there are two prospective clinical trials that have demonstrated an effect of imatinib treatment in unresectable, recurrent and metastatic DFSP patients, achieving partial and complete remissions.4,6
Case Report
Here we present the case of a 31 year-old male, with no significant past medical history. In 2005, he underwent a wide local excision surgical procedure of a tumor lesion in his left arm which was diagnosed as DFSP and treated with post-surgical adjuvant radiotherapy (60 Gy dose). No evidence of recurrence was suggested through follow-up visits. Due to the low risk of relapse, further follow-up visits were suspended in 2011.
In 2012, seven years after the initial surgery, the patient complained several times of a persistent cough. Antitussives were prescribed without any improvement of the symptoms. A few months later, he developed chest pain and an X-ray was performed, which displayed the presence of a big mass in the left lung. A chest computed tomography (CT) scan revealed a huge mass in the upper left hemitorax which measured 14.6×11.1×11.5 cm (Figure 1). The mass appeared to depend on the pleural space. The mass moved above the main left bronchus decreasing the bronchus's size. The anterior cortex of the posterior arch of the fifth, sixth, seventh and eighth left ribs were thickened, which could be suggestive of periosteal reaction by a slow-growing tumor lesion.

Chest X-ray and computed tomography scan displaying a huge left mass.
Bronchoscopy demonstrated mucosal inflammation of the left main bronchus, and the patient underwent biopsy of the affected area. Histopathologic analysis of the biopsy specimen exhibited a spindle cell tumor of low histological aggressiveness which was reported as highly suggestive of a solitary fibrous tumor.
Surgery was scheduled and the patient was operated on February 2013. During the surgical procedure, a firmly attached giant mass located on the left upper and inferior lobes, posterior wall and vertex was observed and the tumor infiltrated all the pulmonary parenchyma. Frozen section analysis of the lesion was performed rendering a histological diagnosis of sarcoma, after which surgeons proceeded to perform a left pneu-monectomy reaching even the ribcage.
Final pathological examination revealed a malignant mesenchymal tumor, a fusiform cell proliferation with atypical storiform pattern and positive for CD34, highly suggestive of metastatic DFSP (Figure 2). The lesion reached the surgical resection edges, but the bronchial resection margin was free. The tumor was submitted for a t(17,22) FISH study, which turned out to be positive.

Fusiform cell proliferation with atypical storiform pattern and positive for CD34. Original magnification 200× (Hematoxylin and Eosin; CD34).
Diagnosed with bulky metastasis of DFSP after left pneumonectomy, the patient was presented at the Thoracic Multidisciplinary meeting for guidance regarding decisions for further treatment options. From May to June 2013 he received radiotherapy on the surgical bed of left pneumonectomy, up to 60 Gy (Figure 3), with grade I radiodermitis as the main toxicity.
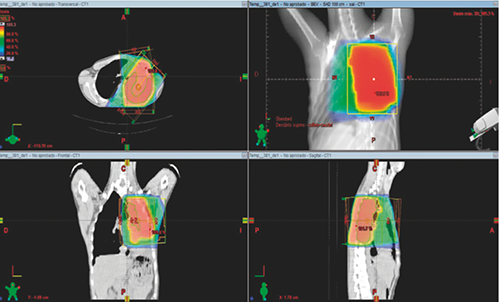
Postsurgical radiotherapy treatment planning.
In July 2013, after sperm cryopreservation and due to the high burden of disease resected, the patient was started on Imatinib 800 mg with an initial adjuvant intention, extrapolating data published on metastatic and unresectable disease. 6
A chest and upper abdomen CT performed in September 2013 revealed a small nodule suspected for recurrence or persistent disease in the left lung apex, between the first and second costal arches. A positron emission tomography (PET)/CT analysis confirmed this finding.
After discussing the case again in the multidisciplinary meeting, surgery was technically eliminated as a potential treatment and histological processes could not confirm whether the nodule corresponded to disease persistence or recurrence. Continued treatment with 800 mg of imatinib was determined to be the most beneficial option. The patient has been with this treatment for 2 years now, with a survival of 30 months after metastasis diagnosis. Profuse tolerance of the treatment has only been stifled by mild emesis and minor fatigue. No progression of the disease has been found in the subsequent CTs. The patient will continue being treated with 800 mg of imatinib and CT scans being performed minimally every six months.
Discussion
Metastases of DFSP are very rare, they occur in less than 5% of the diagnosed cases and are usually associated with multiple local recurrences and fibrosarcomatous transformation of the tumor.2,3 Here we present a case of metastatic DFSP without previous local recurrence and a latency time of 7 years. To our knowledge there are only four other reported cases of DFSP metastasis without previous local recurrence,3,7,8 with only one of them occurring without the presence of fibrosarcomatous transformation, as is represented in this reported case. 8
Regarding surgery, the efficacy of Mohs micrographic surgery in the treatment of DFSP has been documented in several studies with a median recurrence rate of less than 1% (range of 0-8.3%). Recent science has prioritized this treatment because of its accuracy and thoroughness in margin evaluations.4,9,10
DFSP follow-ups after surgery are recommended for a minimum of three years, in six months intervals, because although limited research has been conducted to validate this observation, most local recurrences happen within this time period.1,2,11 As DFSP metastasizes in less than 5% of the cases, evaluations with CT scans, blood cell counts and liver function tests are not recommended. 2 In our case, the patient had follow-ups without any evidence of recurrence for 6 years, and then suddenly developed a largely size and harmful metastatic disease, without previous local recurrence. It is imperative that the medical community be vigilant of the potential for metastases even years after the primary tumor, despite the rarity. If patients with a previous DFSP appear to have any thoracic symptoms, an X-Ray should immediately be performed.
In an article published recently, DFSP with fibrosarcomatous variant is described to have a more aggressive behavior and worse prognosis manifested by a lower recurrence free survival and a greater metastatic potential. 12 Other cases at higher risk of metastases are either recurrent lesions that have progressed for many years or head/neck location. 13 Our patient did not have any of these characteristics.
In our case, surgery was considered the best treatment, due to the massive tumor burden in the thoracic cavity. Neoadjuvant treatment would have also been a good alternative in this case considering the affected margins after surgery. Imatinib is currently the gold standard in the treatment of locally advanced or metastatic DFSP. Typically doses between 400 mg and 800 mg have been used. In modern science, even though there have been around 100 cases treated with neoadjuvant therapy with imatinib with tumor reduction of 50%, the clinical use of neoadjuvant treatment remains to be determined. 14 Furthermore, tumors lacking the t(17;22) (q22;q13)(COL1A1/PDGFB) may not respond to this treatment. 15 Thus, molecular analysis of the tumor using RT-PCR or FISH before the administration of imatinib would be beneficial.
The use of PDGF receptor inhibitors has the potential to change the standard of care for DFSP in future years. Several questions are still opened regarding possible resistances to this targeted therapy. 2 Recently, CDK4/6 pharmacologic inhibition has been described as a preclinically effective treatment against P16 negative, imatinib-resistant fibrosarco-matous DFSP, and these data provide a rational to clinically evaluate CDk4/6 inhibition as a therapeutic strategy in patients with unre-sectable or metastatic imatinib-resistant DFSP. 16
Conclusions
The case discussed here is the second one reporting metastatic DFSP with no previous recurrence or fibrosarcomatous transformation. This case indicates that targeted therapy with imatinib in patients with DFSP harboring a t(17;22)(q22;q13)(COL1A1/PDGFB) could result in very long survivals. It is actually described as the first line treatment for metastatic or unresectable disease. Although the role of imatinib in neoadjuvant and adjuvant setting needs to be determined, the standard of care could change with the use of PDGF receptor inhibitors in the near future. Multi-institutional collaborations will be important to determine the role of imatinib in the perioperative treatment.
Footnotes
Acknowledgments
We would like to thank the Departments of Medical Oncology, Pathology, Radiation Oncology, Radiology, and Thoracic Surgery in Hospital Universitario de la Princesa which participated in the multidisciplinary meetings every week and in taking care of this patient and many others. We would like to thank Melanie Lab for her help with the language grammar and style. We would like to thank Dr. Castillo-Martin for her critical review of this work.