
Abstract
Spindle cell rhabdomyosarcoma is a rare variant of embryonal rhabdomyosarcoma that affects young males and most commonly involves the paratesticular region. We report a case of paratesticular spindle cell rhabdomyosarcoma in a 14-year-old boy, who presented with a painless scrotal mass. Left inguinal orchidectomy was performed. Histopathological and immunohistochemical examination of the mass revealed spindle cell rhabdomyosarcoma of the paratesticular region.
Introduction
Rhabdomyosarcomas (RMS) are uncommon; only 7% of all rhabdomyosarcomas are of paratesticular origin. They are most often observed in children and adolescents and usually presents as a painless scrotal mass. 1 It originates from mesenchymal tissue of the spermatic cord, epididymis and testicular tunics. Because of its superficial location, an early diagnosis leading to its complete surgical resection is possible. However, there is significant morbidity and mortality if the diagnosis is delayed. 2 We report a case of spindle cell RMS of the paratesticular region.
Case Report
A 14-year-old boy presented with a gradually increasing left-sided painless scrotal swelling for the past year. On clinical examination, there was a left sided scrotal mass measuring 10×4.5 cm. The mass was firm in consistency, occupying the left hemiscrotum. The overlying skin was freely mobile over the mass. Testis could not be palpated separately. A nodule measuring 3×2 cm was palpable at the left inguinal region. No lymphadenopathy was noted in the right inguinal region. Clinically a diagnosis of primary malignant tumor of left testis with inguinal metastasis was made
Laboratory investigations revealed high level of serum lactate dehydrogenase (3536 U/L), however; serum levels of -fetoprotein and β-human chorionic gonadotropin were within normal range. A contrast enhanced computed tomography (CECT) scan of abdomen showed a hypodense mass measuring 10×6×2.5 cm in the left paratesticular region with left inguinal lymphadenopathy. However no lombo-aortic lymphadenopathy was revealed. The thoraco-abdomino-pelvic CT scan did not reveal any metastases. Bone marrow aspiration was done, which was negative for infiltration. Left high inguinal orchiectomy was performed. The metastatic nodule in the left high inguinal region was also excised.
On gross examination, the tumor was globular, grey-white and measured 10×6×3 cm. On cut section, the tumor was solid and grey-white in color. Normal testis with intact tunica measuring 1.5×1×0.8 cm was entrapped within the tumor (Figure 1a). Microscopic examination demonstrated a highly cellular tumor composed of fascicles of spindle cells with ovoid hyperchromatic nuclei with blunted ends and containing eosinophilic cytoplasm (Figure 1b). Also seen interspersed were elongated cells with more cytoplasmic eosinophilia (rhabdomyoblasts) (Figure 1c). There were large areas of necrosis. The testis showed infarction and was compressed within the tumor, however was uninvolved. The resected end of the spermatic cord as well as the left inguinal node showed involvement by the tumor. On immunohistochemistry, the tumor cells were positive for desmin and MyoD1 (Figure 1d) and negative for smooth muscle actin (SMA), CD34 and S-100. Based on morphological and immunohistochemical features, diagnosis of paratesticular spindle cell RMS with left inguinal nodal involvement was made. The tumor was staged as stage 3 according to the Intergroup Rhabdomyosarcoma Study Group (IRSG) staging system, and as group II according to the IRSG post-surgery pathologic groups. Four cycles of chemotherapy was administered using the VAC regimen (vincristine, actinomycin-D and cyclophosphamide). However the patient's condition worsened and the patient expired 12 months following initial diagnosis.
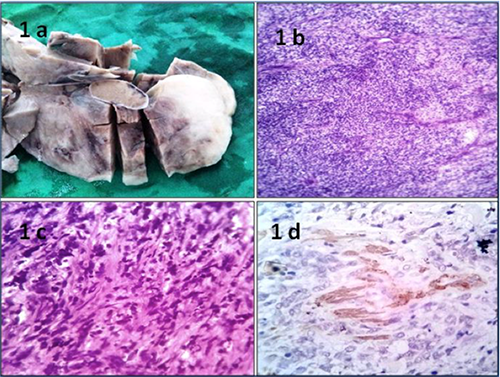
a) Normal testis with intact tunica was entrapped within the tumor. b) A section shows a highly cellular tumor composed of fascicles of spindle cells with ovoid hyperchromatic nuclei. (Hematoxylin & Eosin, 40×) c) Elongated cells with blunted ends and cytoplasmic eosinophilia. (Hematoxylin & Eosin, 100×). d) The tumour cells are positive for MyoD1.
Discussion
Spindle cell RMS is a rare variant of embryonal RMS, which is common in young males and most commonly involves the paratesticular region followed by head and neck region. 3 The most common histologic subtype of paratesticular rhabdomyosarcoma is embryonal RMS (84%) followed by alveolar RMS (8%). Spindle cell RMS constitutes about 5% cases of paratesticular RMS. 2
Paratesticular spindle cell RMS is more common in children and adolescents with a mean age of 7 years. 4 The clinical presentation is usually that of a rapidly growing, painless, soft tissue mass. It rarely invades the scrotal skin. Because of its superficial location, an early diagnosis leading to its complete surgical resection is possible. It thus has a very favorable prognosis if diagnosed timely. However, delay in diagnosis leads to significant worsening of the prognosis with increased mortality and morbidity. 2
Histologically, spindle cell RMS shows spindle cells arranged in fascicles and whorls. 4 Immature rhabdomyoblasts are admixed amongst these spindle cells. The presence of these rhabdomyoblasts points towards the diagnosis of RMS. 5 Cytologically, this tumor shows spindle cells with centrally placed nuclei and well defined cytoplasm along with large fragments of grass-like cytoplasmic processes.6,7 The spindle cells as well as the cytoplasmic fragments may show cross-striations. 6
Morphologically, spindle cell RMS has varied differential diagnosis and high on the list is leiomyosarcoma. The other differentials include fibrosarcoma, solitary fibrous tumor, malignant peripheral nerve sheath tumor (MPNST), triton tumor (MPNST with rhabdomyoblastic differentiation), malignant fibrous histiocytoma, inflammatory myofibroblastic tumor and low-grade myofibroblastic sarcoma. 3
Considering the large number of entities included in the differential diagnosis of spindle cell RMS, immunohistochemistry has an important role in its diagnosis. Spindle cell RMS consistently reacts with myogenic markers such as desmin, myoglobin, MyoD1 and myogenin. 3 Desmin often exhibits nonspecific reactivity in smooth muscle cells and myofibroblasts. Therefore desmin should never be used as a sole marker for diagnosis, but as part of a panel of immunostains. 8 SMA shows variable staining in spindle cell RMS. Thus SMA may not be of help in differentiating leiomyosarcoma from spindle cell RMS. 9 However, leiomyosarcoma along with fibrosarcoma, malignant fibrous histiocytoma, inflammatory myofibroblastic tumor and low-grade myofibroblastic sarcoma do not stain for myoglobin, myogenin or MyoD1.3,10 Moreover, CD34 reactivity in solitary fibrous tumor and S-100 reactivity in MPNST and triton tumor helps in differentiating these spindle cell neoplasms from spindle cell RMS. Embryonal RMS shows a variety of cytogenetic abnormalities like extra copies of chromosomes 2, 8, 13 and rearrangements in 1p11-q11 and 12q13. Cytogenetic analysis of spindle cell RMS has shown it to be closely related to embryonal RMS. 11 In the present case, morphology and immunohistochemistry helped in arriving at an accurate diagnosis.
Making the correct diagnosis is of pivotal importance owing to the multimodal treatment used, which include inguinal radical orchiectomy, local radiotherapy (in the case of microscopic or macroscopic residual tumor after initial or delayed surgery), and multiple sequential or cyclic chemotherapy. An adjuvant chemotherapy regimen of vincristine, actinomycin D and cyclophosphamide has been reported to improve survival. The role of retroperitoneal lymph node dissection (RPLND) is controversial.2,12 In our case, in spite of aggressive surgical management followed by adjuvant chemotherapy, the patient expired after 12 months.
Conclusions
Paratesticular spindle cell RMS is a rare tumor occurring in children and adolescents. Morphologically it may mimic other spindle cell neoplasms. Thus immunohistochemistry plays a pivotal role in its diagnosis. Making a correct diagnosis is crucial owing to the different treatment modalities available for this tumor.