
Abstract
Paratesticular fibrous pseudotumors (PFPs) are rare pathologies with quite wide and variable topographic-morphological features. It is difficult to distinguish PFPs from malignant masses. Treatment can be done by resection of the mass. We reported a young patient's findings about this rare pathology.
Introduction
Also known as chronic proliferative periorchitis, inflammatory pseudotumor, and reactive periorchitis, paratesticular fibrous pseudotumors (PFPs) are rare pathologies with quite wide and variable topographic-morphological features, and their etiology is not fully understood. 1 The term fibrous pseudotumor was first defined Balloch in 1904. 2 In general, fibrous pseudotumors are considered benign lesions of the paratesticular structures. 3 PFPs account for approximately 6% of all paratesticular lesions. 4 It is difficult to distinguish PFPs from malignant masses via clinical and radiological findings or to establish the diagnosis in the preoperative period. Therefore there is still not a consensus about treatment procedure.
In this article, we present clinical, radiological, pathological, and surgical findings of this rare pathology in a young patient in light of the current literature.
Case Report
A 41-year-old male patient with one child presented due to small, pain-free, solid, palpable structures in the right testicle. Physical examination revealed two palpable soft tissues with a mild solid consistency, smaller than 1 cm, adjacent to the right testicle. The testicles were normal. In ultrasonography, nodular thickenings were observed in the left grade 3 varicocele and the right tunica vaginalis, and magnetic resonance imaging (MRI) was recommended. In MRI, intensely contrasted foci (possibly vascular structures, a mass originated from the tunica vaginalis) of 7 mm and 9 mm outside the testicle and medial of the right testicle were found, giving the impression of having originated from the tunica vaginalis, as well as 8 mm cranial of the right testicle adjacent to the epididymis; these showed a hypointense signal (Figure 1). All biochemical markers were within the normal range. All biochemical analyses including level immunglobulin G4 (IgG4) were normal. Testicular tumor markers were within the normal level.
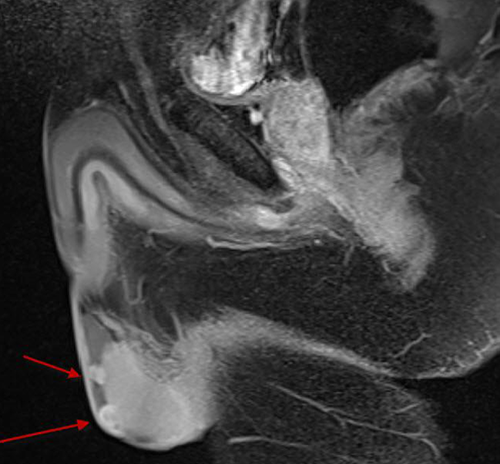
Magnetic resonance imaging of the case.
Surgical exploration was selected. The testicle and its attachments were delivered; when the tunica vaginalis was opened, multiple small, diffuse nodular structures in addition to large nodules were seen (Figure 2). A large nodule was evaluated via frozen section. After it was reported that this was not malignant, sparing the testicle, the tunica vaginalis was excised and the mass was totally removed. In microscopic examination of the material, the sections revealed tumoral formations consisting of the vascular structures that in general were not connected with each other. These comprised fibrous connective tissue in large areas, sometimes with a small diameter, and lumina filled with erythrocytes. There were abundant vascular structures with cd 34 staining and, sometimes, fibrous connective tissue with vimentin (Figure 3). The definitive pathological diagnosis was reported as PFP.
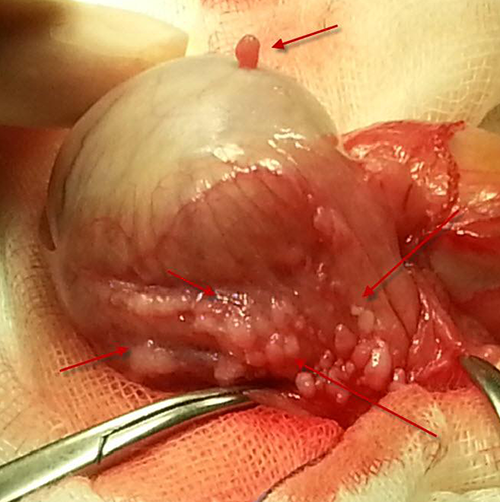
Surgical exploration image of the case.

Pathological examination of the case.
After 12 months of follow-up neither recurrence of intrascrotal disorders nor any other serious diseases have been noted.
Discussion
PFPs are infrequent, reactive, benign lesions of the testicular tunica. The reactive process can be stimulated by infections, surgery, or trauma. 5 In addition, PFP has also been proposed to be a manifestation of an IgG 4-related sclerosing disease in the paratesticular region. 6 The levels of IgG4 were within the normal limits in our patient.
PFPs may be seen in every age, although the third decade of life exhibits a peak incidence. Of the cases, 50% may be accompanied by hydrocele and 30% by previous trauma or epididymo-orchitis. 7 Our patient was 41 years old and presented with the complaint of a painfree mass in the right hemiscrotum. There was no history of infection or trauma.
Dieckmann and colleagues reported the number of cases described as of 2013 to be about 200. 8 Less than 10% of the cases may have originated from the epididymis or spermatic cord. Patients usually present with the complaint of unilateral and painless masses of various sizes.
In general, ultrasonography is the initial modality of radiological evaluation. In ultrasonography, PFPs are typically seen as a solid lesion with various echogenicities depending on the cellular components of the fibrous tissue and the amount of calcification. Scrotal color Doppler ultrasonography may provide insight into the vascularity of the lesion. MRI can be preferred in the preoperative evaluation and postoperative follow-up. PFPs show intermediate to low signal intensity on T1-weighted images and uniformly very low signal intensity on T2-weighted images. 9
Malignancy is the most important factor that needs to be taken into account in the differential diagnosis. PFPs have no specific tumor markers. Fibrous mesothelioma, fibroma, leiomyoma, neurofibroma, idiopathic fibrosis, adenomatoid tumors, and paratesticular malignant tumors should be considered in the differential diagnosis. 10
Since the diagnosis of PFPs is difficult and they mimic malignant tumors, radical orchiectomy is often performed although these lesions are benign. Intraoperative frozen section is important in preventing unnecessary radical orchiectomy. 11 Some studies have recommended ultrasonography or microscopy for intraoperative evaluation of the mass. 12 In our patient, per-operative frozen section was carried out, and when it was understood there was no malignancy, total mass excision with the tunica vaginalis was applied, thereby sparing the testicle. In their report underlining the importance of intraoperative frozen section, Ba al and colleagues reported that they applied mass resection and saved the testicle in five of six PFP patients. 13 However, in the testicle-sparing approach, total excision of the mass may be challenging. Therefore, in addition to the age of the patient, the anatomical condition of the mass is also important when a surgical procedure is chosen.
In the microscopic examination of PFPs, intermixed hyalinizing and hypercellular areas, heterogeneous inflammatory cells, and intense myofibroblastic proliferation are remarkable. In addition, calcification, ossification, myxoid changes, and chronic inflammatory infiltration of lymphocytes, plasma cells, and histiocytes may also be monitored. 14 Macroscopically, there are circumscribed, solid single or multiple nodules with sizes differing between 0.5 and 8 cm; these mostly originate from the testicular tunica and less frequently from the spermatic cord or epididymis. 15 There were multiple nodules smaller than 1 cm in our patient.
There is no significant information in the literature on the postoperative recurrence of PFPs. However, clinical recurrence could be expected in the cases of incomplete resection, progressing inflammation, and fibrous tissue proliferation. No recurrence was observed at the 1-year postoperative follow-up of our patient.
Conclusions
Because PFPs are a rare clinic entity usually seen in young-adults and can mimic malignancy, preoperative diagnosis is challenging. We believe that intraoperative frozen section will prevent unnecessary orchiectomy. However, further studies with wider series are needed in order to better understand PFPs from a clinical perspective and to determine the appropriate treatment modality.