
Abstract
Rosai-Dorfman disease (RDD) is a rare, benign histiocyte disorder originally described by Rosai and Dorfman in 1969 as sinus histiocytosis with massive lymphadenopathy. It most typically presents as massive, painless cervical lymphadenopathy, and it is most often found in adolescents and young adults. Extranodal involvement is a common feature of RDD and may occur in more than 40% of patients. Less commonly, the disease can be seen in the bone. There are scattered case reports discussing the use of radiotherapy in the treatment of RDD. Here, we present a case of extranodal RDD of the femur in a 49-year-old African American female. The patient underwent three surgical procedures prior to undergoing radiotherapy. Pathology was consistent with extranodal RDD. The cells stained positive for CD68 and S-100. Pathognomonic features such as emperipolesis and replacement of the bone marrow by diffuse infiltrating of histiocytes and intervening bands of plasma cells proliferation were noted. Prior to radiotherapy, the patient required a walker to assist with ambulation and was utilizing a wheelchair while in the clinic. The decision was made to proceed with 30 Gy of external beam radiotherapy in 15 fractions. After five fractions, the patient's pain resolved entirely. She no longer required pain medication and was ambulating without assistance. She experienced no adverse events from the radiation. Extranodal RDD is a rare disorder, and evidence for treatment is derived from scattered case reports. Previous reports have indicated a dose response to radiotherapy in the 20-30 Gy range for RDD; however, our patient developed complete resolution of her symptoms after 10 Gy. While the optimal dose regimen has not yet been established, symptomatic patients appear to benefit from external beam radiotherapy for extranodal RDD.
Introduction
Rosai-Dorfman disease (RDD) is a rare benign histiocyte disorder originally described by Rosai and Dorfman in 1969 as sinus histiocytosis with lymphadenopathy.1,2 It typically presents as massive, painless cervical lymphadenopathy, and it is most often found in adolescents and young adults. Extranodal involvement is a common feature of RDD and may occur in more than 40% of patients.3,4 Most often, however, it is seen in the head and neck, upper aero-digestive tract, orbits and the paranasal sinuses. Less commonly, the disease can be seen in the bone.1–4 When symptomatic, RDD is often treated with surgery and or high dose prednisone.3,5–8 There are scattered case reports discussing the use of radiotherapy in the treatment of RDD. Here, we present a case of extranodal RDD of the femur treated with surgery and radiotherapy.
Case Report
A 49-year-old African American female patient first noted pain in her distal right thigh in April 2008, which was managed with narcotic medication until December 2009. The patient underwent bone debridement at an outside institution. Pathology from this initial surgery was inconclusive. The patient underwent bone debridement once again in January 2010 at the same institution, as a result of her continued lower extremity pain and imaging abnormalities; pathology was again inconclusive but was thought to be consistent with osteomyelitis. The patient received several weeks of antibiotic therapy with vancomycin and daptomycin. She discontinued narcotics after this initial resection.
The patient was pain free until November 2010, at which time she sought an evaluation with an orthopedic surgeon and was again started on narcotic analgesics. She was ultimately referred to our clinic and underwent repeat magnetic resonance imaging (MRI) in March 2011, at which time was noted abnormal signal and enhancement about the bone/cement interface around the mid distal femoral bone cement with interval focal cortical erosion compatible with residual or recurrent lesion or infection. A CT-guided biopsy was performed and demonstrated lymphocytic infiltrate with increased B-cells. Molecular analysis by polymerase chain reaction (PCR) analysis did not show a clonal immunoglobulin gene rearrangement, arguing against a lymphoproliferative disorder.
In May of 2011, the patient underwent surgery at our institution. The cement was removed, the lesion was aggressively curettage, tissue was obtained for histology and culture, and antibiotic-impregnated cement beads were placed in the bone defect. Pathologic evaluation showed the lesion to be consistent with extranodal RDD. Pathognomonic features such as emperipolesis and replacement of the bone marrow by diffuse infiltrating of histiocytes and intervening bands of proliferating plasma cells were noted. The histiocytes stained positive for CD68 and S-100 by immunohistochemical study (Figure 1). Tissue cultures were negative and the patient was taken back to surgery for removal of the antibiotic-impregnated beads and packing of the cavity with allograft bone.

The bone marrow is completely replaced by the diffuse infiltrating of histiocytes, intervening by bands of plasma cells proliferation (A, Hematoxylin & Eosin 10×). Emperipolesis is easily identified in the histiocytes (A). Immunohistochemical study of S-100 is positive in numerous histiocytes and highlights the emperipolesis (B, Hematoxylin & Eosin 20×).
The patient did well for approximately a year, at which time her pain recurred. Imaging indicated resorption of the bone graft consistent with recurrence of disease. The orthopedic oncologic surgeon consulted with colleagues at several institutions across the country; the consensus opinion was to repeat aggressive curettage. This procedure was performed followed by packing of the bone defect with allograft bone in July 2012. Pathology examination again confirmed extranodal RDD, with the same features as before.
Unfortunately, the patient's pain recurred once again in January 2013 and imaging was again consistent with recurrent disease. At that time she was referred to the radiation oncology clinic. She was complaining of severe right lower extremity pain that was exacerbated by movement. The pain would last for several days and only resolve with narcotic medication and bed rest. Repeat imaging in April 2013 (Figure 2A) noted a lobulated focus of signal abnormality and enhancement along the postero-lateral aspect of the femoral shaft at the posterior-superior margin of the bone graft window defect, which was worrisome for recurrence. On exam, she had weakness of the right lower extremity with pain on knee extension and tenderness to palpation of the surgical incision region in the lateral distal thigh. No significant edema, skin discoloration or warmth was noted. The patient was ambulating with the assistance of a walker and required a wheelchair to move around the clinic. The decision was made to proceed with palliative external beam radiotherapy, 30 Gy in 15 fractions (Figure 3). The dose was selected after conducting a literature review to determine the dose response of this disease to radiotherapy. Though limited evidence is available, it appeared that there are a high rate of non-responders if a dose less than 30 Gy is utilized. 3 After 5 fractions over the course of five days, the patient's pain resolved entirely. She no longer required pain medication and was ambulating without assistance. She experienced no adverse events from the radiation. She began physical therapy and rehabilitation shortly after completion of radiotherapy. At her first follow-up in June 2013, the patient had no clinical symptoms. Initial follow-up MRI noted an area of signal abnormality and enhancement at both the proximal and distal aspects of the curettage bed that had increased in prominence; due to the patient's lack of symptoms, this was felt to be inflammation related to radiotherapy, and the decision was made to continue observation. Subsequent imaging in October 2013 and January 2014 found this area to be stable, and the patient remained asymptomatic (Figure 2B). At the time of report, the patient had been disease free and asymptomatic for approximately 15 months.
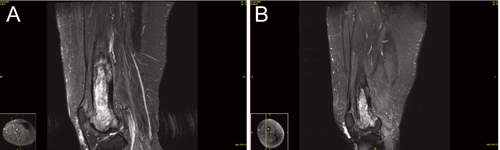
Pre- and post-treatment magnetic resonance images. Pre-radiotherapy sagittal T2 STIR magnetic resonance image demonstrates a lobulated focus of signal abnormality and enhancement along the postero-lateral aspect of the femoral shaft at the posterosuperior margin of the bone graft window defect. B) Post-radiotherapy sagittal T2 STIR magnetic resonance image demonstrates stable abnormal signal and enhancement about the curettage cavity compatible with stable tumor burden and post-treatment change.
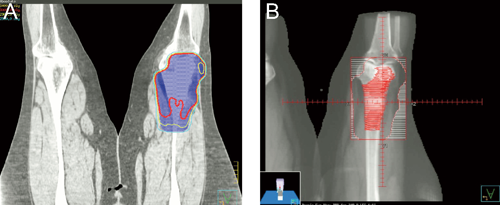
Six MV photons were used in AP/PA technique. The red line in A) represents the 30 Gy isodose line; the blue line represents 25 Gy. In panel B), which represents a beam's eye view of the treatment plan, the nodularity noted on MRI is contoured in red. Blocks were draw in an attempt to spare as much of the skin and joint space as possible.
Discussion and Conclusions
The diagnosis of RDD is notoriously difficult, especially when the disease presents in the bone. This is thought to be due to the extensive component of fibrosis and less conspicuous evidence for emperipolesis when RDD is found in the bone. 9 Clinical features parallel those seen in malignant bone tumors, sarcomas, inflammatory pseudotumors, and Langerhans cell histiocytosis. Some authors believe that RDD is likely underdiagnosed, both due to the difficulty of the diagnosis as well as the self-limited nature of the disease seen in some patients. 9 The difficulty in diagnosis coupled with the rarity of the disease may help explain why our patient had been symptomatic for greater than three years and had undergone two prior surgical interventions before a diagnosis was determined.
As less than 5% of reported cases of RDD include skeletal involvement, it is difficult to determine the best treatment for these patients.4,9 While many authors have argued that the disease is generally indolent and tends to wax and wane with regard to symptoms, others have argued that without treatment 70-80% of patients experience persistent disease with at least intermittent symptoms.1,2,4,8 Our patient experienced a similar course, requiring narcotics intermittently throughout the course of her disease. Nevertheless, most authors agree that surgical removal of the lesion is a mainstay of treatment. A more aggressive surgical approach could have been considered, namely en block resection of the distal femur. While the risk of local recurrence would have been negligible after such a surgery, the patient would have required reconstruction of the skeletal defect with a distal femoral replacement knee arthroplasty, thereby significantly increasing the risk of surgical complications and potential for long-term implant related problems. Given the benign nature of the condition and the patient's high functional status, such an en bloc resection was not favored.
The role of radiotherapy as a treatment modality for RDD is inconclusive. Radiotherapy dosing recommendations vary broadly, with some authors recommending doses between 20 to 30 Gy3,4,9 and other authors reporting treatment doses higher than 50 Gy5–8,10,11 Given the proximity of our patient's lesion to the joint space, we opted to pursue a dose of 30 Gy; however, we were prepared to retreat the patient after a several month interlude should she not have experienced a good clinical response.
Most authors agree that chemotherapy is of limited benefit in the treatment of these patients.3,4 Agents such as antimetabolites, alkylators, and vinca alkaloids have all been used, but mostly with limited benefit. Thus, after consultation with our colleagues in medical oncology, we opted to observe the patient after completion of her radiotherapy.
Due to the rarity of the disease, it is unlikely that there will ever be definitive clinical guidelines for the treatment of extranodal RDD. Clinicians will have to rely on case reports such as this one to determine the most appropriate treatment for their patients. While the optimal dose regimen has not yet been established, symptomatic patients do appear to benefit from external beam radiotherapy for extranodal RDD. We would recommend the use of radiotherapy in patients whose symptoms persist or recur after surgical intervention or for those patients who are found to be unsuitable candidates for surgery.
Footnotes
Conflict of interests: the authors declare no potential conflict of interests.
Acknowledgments
The authors would like to thank Kelly Viola, ELS for her assistance with the editing of this manuscript.