
Abstract
Hidradenocarcinoma is a rare aggressive form of cutaneous adnexal skin carcinoma originating from the sweat gland. Due to its low incidence, prognostic and treatment strategies are still being explored both for primary and advanced disease. This tumor most often presents as either solid or cystic appearing subcutaneous nodules, which may be associated with pruritus or ulceration. To date the mainstay of treatment for local disease has been surgical excision; however, the paucity of historical data available has shown that these tumors often behave aggressively with high rates of local recurrence, metastasis, and poor overall outcomes. There are few case reports describing the utility of radiation therapy in the treatment of hidradenocarcinoma. Herein, we present a case of metastatic apocrine hidradenocarcinoma in a 32-year-old Caucasian male. The patient initially underwent excisional biopsy which confirmed the diagnosis of poorly differentiated, highly infiltrative, apocrine hidradenocarcinoma. He received systemic chemotherapy for metastatic disease, followed by radiation therapy to areas of grossly palpable adenopathy. Prior to radiation therapy the patient had an enlarged hypermetabolic conglomerate of lymph nodes in the right axilla, and borderline enlarged low activity nodes within the left axilla. He received 3 cycles of chemotherapy followed by tamoxifen and radiation therapy (50.4 Gy in 28 fractions) to areas of progressive disease in the bilateral axilla, lower neck, and axillary skin. Following treatment, the patient had complete resolution of skin nodules and improvement of his pruritus. While the role of radiation therapy in the treatment of hidradenocarcinoma has not been well established, this case report demonstrated the potential benefit of external beam radiotherapy in the management of this rare disease.
Introduction
Hidradenocarcinoma was first described in 1954 by Keasby and Hadley as a clear cell eccrine carcinoma. 1 Hidradenocarcinoma, the malignant counterpart of hidradenoma, is an extremely rare malignant tumor, which may exhibit an aggressive clinical course with common occurrence of metastasis. 2 Reflecting its rarity, hidradenocarcinomas have a prevalence as low as 0.05%. 3 In one study of 450,000 consecutive biopsy specimens received in a dermatopathology laboratory over a period of 20 years, only two cases of hidradenocarcinoma (<0.001%) were diagnosed. 4 There have been over 50 case reports and small case series, but there is little information available on the natural history and management of this rare tumor. 3 The disease usually presents as an ulcerated reddish nodule on the face or axillary region of elderly patients, but has also been reported to occur on the extremities, anogenital region, and chest.5,6 The tumor is most distinctly characterized by its frequent clear cell morphology, and often arises de novo, but may also arise out of its benign counterpart (hidradenoma). Both cytonuclear atypia and increased mitotic activity, in addition to infiltrative borders, vascular and neural invasion, and lymph node metastases, may help distinguish it from hidradenoma. Macroscopically, compared to its counterpart, hidradenocarcinoma appears to be larger, less well-demarcated, and more asymmetrical. Reports suggest more than 60% of patients experience metastases within the first 2 years. Hematogenous metastases to lymph nodes, bones, lung, pleura, and other viscera have all been reported. Hidradenocarcinoma is traditionally regarded as a malignancy of eccrine cutaneous sweat glands. 1 Herein, we present a rare case of hidradenocarcinoma in a patient with apocrine features whose disease responded well to radiation therapy both for local control and symptom relief.
Case Report
A 32-year-old Caucasian male first noted a growth in his right axilla two years prior to diagnosis. He was asymptomatic, and the area was followed with observation. However, 2 years later, the lesion began to grow and develop ulceration. Biopsy revealed a poorly differentiated, highly infiltrative apocrine hidradenocarcinoma. Cytokeratin was immunopositive, along with CD34 and carcinoembryonic antigen; however, S-100 and Melan-A were negative. Tissue stained positive for AE1/AE3, cytokeratin 7, estrogen receptor and progesterone receptor, and negative for human epidermal growth factor receptor 2 [(HER-2/neu) Figure 1]. There was evidence of involvement of the epidermis, dermis, and possible lymphatic invasion. A positron emission tomography-computed tomography (PET/CT) showed an enlarged hypermetabolic conglomerate of lymph nodes in the right axilla, measuring 2.1×1.5 cm, with a max standardized uptake value (SUV) of 7.1, non-enlarged, level IV, right-sided, cervical nodes with a max SUV of 1.9, left axillary lymph nodes with a max SUV of 1.9, and a hypermetabolic lytic lesion in the posterior right fifth rib, with a max SUV of 7.1 (Figure 2A). Biopsy of a left axillary subcutaneous lesion was also positive for hidradenocarcinoma, confirming metastatic disease. The patient had palpable subcutaneous nodules in bilateral axilla, groin, face (lip and chin), neck, and chest wall, which were not evident by PET/CT.

A) Metastatic hidradenocarcinoma involving a lymph node. Hematoxylin and eosin (H&E) stain, magnification 200×, B) Metastatic hidradenocarcinoma involving a lymph node. H&E stain, magnification 400×; C) metastatic hidradenocarcinoma. Immunohistochemistry showing strong reactivity for estrogen receptor (magnification 400×).
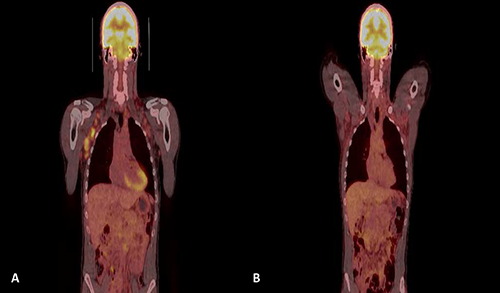
A) Coronal positron emission tomography/computed tomography (PET/CT) prior to radiation therapy showing multiple enlarged axillary lymph nodes with areas of conglomeration and hypermetabolic activity within the right axilla, consistent with patient's biopsy proven apocrine hidradenocarcinoma. B) Coronal PET/CT 15 months post radiation therapy showing resolution of lymphadenopathy and metabolic activity within the bilateral axilla.
The patient received three cycles of chemotherapy with carboplatin 6AUC and paclitaxel 200 mg/m2 given every 3 weeks, with pegfilgrastim support. Restaging CT scan of the chest, abdomen, and pelvis following chemotherapy showed increasing size of bilateral axillary lymphadenopathy with stable disease elsewhere. The patient was started on tamoxifen. Due to localized progression of disease, radiation therapy was recommended to the bilateral axilla. The patient received external beam radiation therapy to the axilla and surrounding subcutaneous nodules to a total dose of 50.4 Gy in 1.8 Gy fractions (Figure 3). He tolerated this treatment well with minimal toxicity including dry desquamation of the bilateral axilla, minimal nausea, and esophagitis. Clinically, his subcutaneous nodules flattened, and radiographically, the axillary lymph nodes normalized. The patient underwent restaging CT of the chest, abdomen, and pelvis every 3 months following completion of radiation therapy while on tamoxifen, which remained stable for 10 months.
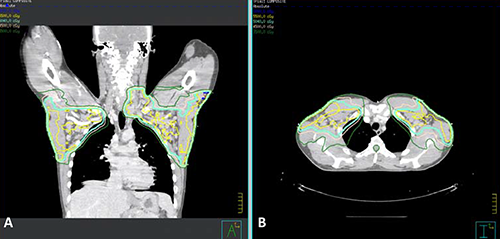
A) Coronal computed tomography (CT) showing isodose lines for the bilateral axilla and left supraclavicular radiation treatment fields. B) Axial CT showing isodose lines for the bilateral axilla and left supraclavicular radiation treatment fields.
Cancer exome sequencing was performed, which showed somatic mutations in the following genes:
Unfortunately, he developed increasing rapid growth of subcutaneous nodules in the perirectal area and bilateral groins, as well as additional, but limited, nodules of the lower back and scalp. These became increasingly pruritic and painful. Biopsies of the left lower back and right upper inner thigh were positive for metastatic hidradenocarcinoma. A PET/CT showed increasing growth of subcutaneous soft tissue nodules in the occipital region, anterior abdomen, lower anterior pelvis, and back; however, the bilateral axilla remained free of lymphadenopathy and showed no significant metabolic activity greater than 15 months after radiation therapy. Given his symptomatic metastatic disease, he received palliative radiation therapy to the bilateral groins, perineum, and suprapubic areas. He received en fosse electron therapy to a total dose of 40 Gy in 16 fractions. He did experience moist desquamation of the perianal region, but had a near complete response of all subcutaneous lesions 3 months after radiation therapy. He was started on vismodegib chemotherapy due to the presence of a mutation in
The patient subsequently developed progression of disease outside of the radiation treatment fields and was initiated on Anti-LAG3 monoclonal antibody therapy. He had progression of disease shortly thereafter and is currently being considered for therapy with an Anti-Pd-1 agent.
Discussion and Conclusions
Apocrine hidradenocarcinoma is an extremely rare malignancy, which makes its diagnosis and treatment particularly challenging. To date, only small case series and institutional reports can be found in the literature.7–9 Due to its low incidence, the feasibility of a sufficiently powered prospective clinical trial is unlikely, making population-based analysis and retrospective data of particular value for this tumor. Apocrine hidradenocarcinoma typically has an aggressive course of progression with an initial presentation of locally advanced disease, followed by a short interval change to metastatic disease.4,9 Spread from the initial primary lesion typically involves the regional lymph nodes followed by hematogenous spread to bone, lung, pleura, and in rare cases, other visceral organs, as evidenced by our patient. Tumor involvement of the lymph nodes has been shown to have a significant negative impact on median survival based on SEER database statistics. 10 Previously published studies have shown a decrease in median survival from 55 months to 33 months for patients with positive lymph nodes, and a further decrease to 14.5 months with distant disease. 8
Aggressive local surgical excision has historically been the standard of care for localized disease, but the extent of negative margins necessary remains a topic of debate.7,8 In the surgical literature, debate remains regarding standardization of sentinel lymph node biopsy for hidradenocarcinoma. 1 Some authors have speculated that there may be a larger role for adjuvant therapy based on the grade, close or positive margin status, perineural extension, angiolymphatic invasion, and regional metastasis. This would more closely parallel the treatment recommendations for other high-grade carcinomas of the skin, including melanoma, Merkel cell cancer, and squamous cell carcinoma, which have similarly shown a high propensity toward local recurrence and a high rate of metastasis.1,4
There are presently a limited number of case reports which describe radiation treatment details or outcomes for patients with apocrine hidradenocarcinoma. A previously published review and case report have suggested adjuvant radiation therapy for large tumors (>5 cm), positive margins following surgery (<1 cm), and moderate to poorly differentiated tumors with lymphovascular space invasion. 5 Additionally, adjuvant therapy should be considered for patients with >4 involved lymph nodes or extranodal extension.5,11 Published case reports have shown the utilization of external beam radiation therapy doses ranging from 42-66 Gy, typically in the adjuvant setting.3–5,11–13 One study noted a dramatic response and local control achieved after 50 Gy of radiation therapy to both the supraclavicular fossa and axilla; however, the patient later succumbed to metastatic disease. 5 Another report describes the surgical treatment of a right midline apex scalp tumor with Mohs surgery followed by 50 Gy of radiation therapy delivered to the right posterior hemiscalp and postauricular/occipital lymphatic basins. The patient remained free of clinical recurrence at 12 months. 4 The highest delivered dose of 66 Gy was utilized for a patient with a parotid gland recurrence 5 months after surgery. The patient was subsequently treated with 66 Gy to the primary tumor bed and upper neck lymphatics, with an additional 50 Gy delivered to the ipsilateral, supraclavicular nodal region. The patient showed good local control at 15 months following radiation with minimal treatment toxicity (Figure 2B). 13 Little data exists regarding the usage of radiation therapy in the setting of metastatic hidradenocarcinoma; however, here we provide additional support of the utilization of an equivalent dose of 50 Gy for improved local control and palliation of symptoms.
The addition of chemotherapy for the treatment of locoregional and metastatic disease also remains an area of interest within the field of Oncology. A number of chemotherapy regimens have been utilized to treat apocrine hidradenocarcinoma with varying degrees of success. More recently, the widespread availability of immunohistochemical and genomic testing has opened the door to more targeted agents. There have been reported cases showing success utilizing trastuzumab for HER-2/neu expressing apocrine hidradenocarcinoma, as well as hormonal directed agents such as tamoxifen for those with estrogen receptor positivity.5,14 The success of agents such as anti-PD-L1 inhibitors for the treatment of metastatic melanoma lends a possible line of therapy for hidradenocarcinoma in the future, as well as a model for the possible efficacy of gene directed therapies.