
Abstract
Castleman's disease is a group of rare lymphoproliferative disorders. The plasmablastic multicentric Castleman's disease is frequently discovered in HIV-infected individuals in association with Kaposi sarcoma (HHV-8). Thirty-five year old male presented to our care with the main compliant of severe back pain for one week. His past medical problems include acquired immune deficiency syndrome diagnosed 12 years prior and Kaposi sarcoma, currently on highly active antiretroviral therapy (HAART). Radiographic imaging revealed hepatomegaly and diffuse lymphadenopathy. The HIV viral load was <20 polymerase chain reaction copies/mL, absolute CD4 count was 453 cells/mcL (490-1740 cells/mcL) and CD8 count was 4142 cells/mcL (180-1170 cells/ mcL). Excisional biopsy of the left supraclavicular lymph node was performed with pathological findings of HHV8+ Kaposi sarcoma in the background of multicentric Castleman's disease (plasmacytic variant). No evidence of transformation into large B-cell or plasmablastic lymphoma was noted. He was discharged on HAART and follow up to receive chemotherapy with cyclophosphamide, adriamycin, vincristine plus prednisone was started and rituximab plus prophylaxis for
Introduction
Castleman's disease (CD) is a group of rare lymphoproliferative disorders with heterogeneous manifestations that range from being asymptomatic to recurrent episodes of widespread lymphadenopathy with systemic symptoms. 1 CD is classified as either localized (unicentric) or generalized (multicentric) lymphadenopathy. CD is further divided into variants based on the characteristic lymph node findings. Three variants have been described, hyaline vascular, plasma cell or mixed. The hyaline vascular variant is the most common type of CD and accounts for 70% of cases and is equally distributed among both genders. 2 A single node or chain of lymph nodes is involved, most commonly in the mediastinum. The plasma cell variant represents 10-20% of cases. 2 This variant will have constitutional symptoms and enlarged lymph nodes.
The hyaline-vascular variant is characterized by abnormal follicles with regressed germinal centers surrounded by widened mantle zones composed of small lymphocytes in an onion ring-like arrangement. 3 The plasma cell variant has a hyperblastic germinal center and a large accumulation of polyclonal plasma cells in the interfollicular area. 3 The mixed variant, demonstrates the presence of both hyaline vascular and plasma cell characteristics. The plasma cell type has been further defined into a less common subvariant form that is characterized by large plasmablasts harboring human herpesvirus-8 (HHV-8) with the potential to progress to plasmablastic monoclonal lymphoma.3,4 This subvariant has an outer mantle zone of the follicles with an increased number of plasmablasts. The HHV-8 plasmablasts can rapidly multiply and coalesce to form microlymphomas that eventually could progress to plasmablastic B-cell lymphoma.2,5
The plasmablastic multicentric Castleman's disease (MCD) is multifocal, aggressive and is associated with polyneuropathy, organomegaly, endocrinopathy, monoclonal gammopathy and skin changes (POEMS).1,5 This type is frequently found in HIV-infected individuals. It is clinically characterized by severe inflammatory symptoms attributable to disarray in cytokines such as elevations in interleukin-6 (IL-6) and interleukin1-10 (IL-10).2,6 The clinical presentation of MCD is more varied and commonly features fever, night sweats, anorexia, hepatosplenomegaly, weight loss, or failure to thrive. 7 The amount of HHV8 in peripheral blood mononuclear cells or plasma cells has been noted to correspond with symptoms during MCD flare.1,6 Laboratory abnormalities could include an elevated acute phase reactants anemia, hypoalbuminemia, polyclonal hyperglobulinemia, elevated transaminases and renal disease.2,5,7
Dispenzieri
Case Report
Thirty-five year old Hispanic male presented to our care with the main compliant of severe intermittent mid to lower back pain that had progressively worsened since 1 week. The back pain was further described as radiating to both lower extremities and aggravation of the pain with movement such as bending forward and walking with occasional numbness in both lower extremities. He denied any trauma, weakness in his back or lower extremities, saddle anesthesia, urinary or fecal incontinence. His past medical problems include acquired immune deficiency syndrome (AIDS) diagnosed 12 years prior and Kaposi sarcoma.
One year prior to admission he began to develop systemic symptoms such as fever, chills and diffusely swollen lymph nodes. He underwent a fine needle (FNA) aspiration biopsy of right axillary lymph node with pathology revealing the presence of reactive cells for human herpes virus 8. Five months afterwards he had an excisional biopsy of the left inguinal lymph node and a punch skin biopsy that tested positive for Kaposi's sarcoma. He was treated with doxorubicin for a total of 6 cycles. Despite this, he had persistence and worsening of his symptoms but now associated splenomegaly and pancytopenia. Two months prior he had a splenectomy with pathological findings of multicentric Castleman's disease, plasmablastic variant with evidence of Kaposi sarcoma and areas of extensive infarction. However, he had not been treated for the multicentric Castleman's disease and was compliant with antiretroviral therapy.
Initial vital signs on admission were significant for a fever of 38.5ºC and tachycardia. Physical exam findings included generalized lymphadenopathy, bilateral non-pitting lower extremity edema, right sided ptosis and facial droop. Hyperpigmented purple/erythematous maculopapular skin lesions were noted on both thighs that were characteristic of Kaposi sarcoma. The initial laboratory findings (Table 1) were significant for thrombocytopenia and hypoalbuminemia.
Initial laboratory workup.

BUN, blood urea nitrogen; AST, aspartate-aminotransferase; ALT, alanine-aminotransferase; Ig, immunoglobuline.
Radiologic imaging was obtained on the day of admission. This included an abdominal computed tomography (CT) (Figure 1) that showed hepatomegaly and diffuse abdominopelvic lymphadenopathy of the retroperitoneal, periaortic, peripancreatic, mesenteric, pelvic, bilateral iliac and inguinal regions. The thoracic and lumbar magnetic resonance imaging (MRI) also revealed diffuse lymphadenopathy of the bilateral supraclavicular, axillary, posterior mediastinal, retrocrural and paraspinal nodes. On the second hospital day the infectious disease consult service recommended HAART with Raltegravir 400 mg tablet twice daily and Abacavir/Lamivudine 600/300 mg tablet every day. To determine the immunological status of the patients the HIV viral load was <20 PCR copies/mL, HHV-8 viral load was 25,498 DNA copies/mL, absolute CD4 count was 453 cells/mcL (490-1740 cells/mcL) and CD8 count was 4142 cells/mcL (180-1170 cells/mcL). On the fourth hospital day the hematology/oncology consult service was concerned for a plasmablastic lymphoma and therefore recommended a bone marrow biopsy and excisional lymph node biopsy of the supraclavicular lymph node. A MRI brain and lumbar puncture with CSF analysis were performed to further evaluate his neurological deficits but both were unremarkable. On the ninth hospital day the excisional biopsy of the left supraclavicular lymph node was performed with pathological findings (Figure 2) of HHV8+ Kaposi sarcoma in the background of multicentric Castleman's disease (plasmacytic variant). No evidence of transformation into large B-cell or plasmablastic lymphoma was noted. On the twelve hospital day a bone marrow biopsy was performed with pathological findings of hypercellular marrow demonstrating reactive plasmacytosis with polytypic pattern by kappa and lambda light chains immunostains. On the fifteenth hospital day the patient was discharged home in stable condition on HAART and follow up with the infectious disease and hematology/oncology services for further outpatient management. Chemotherapy with CHOP (cyclophosphamide, adriamycin, vincristine plus prednisone) was started and rituximab plus prophylaxis for pneumocystis carinii was included. As an outpatient he received intravenous (IV) cyclophosphamide (750 mg/m2 on day 1), IV adriamycin (50 mg/m2 on day 1), IV vincristine (1.4 mg/m2 on day 1), and oral prednisone (100 mg for 5 days) was administered every month for 4 cycles. The facial droop and ptosis resolved during chemotherapy and the diffuse lymphadenopathy resolved after the complete course of chemotherapy.

Abdomen/pelvis computed tomography. A) Diffuse abdominopelvic lymphadenopathy (red arrows); B) bilateral inguinal and iliac lymphadenopathy (blue arrows).
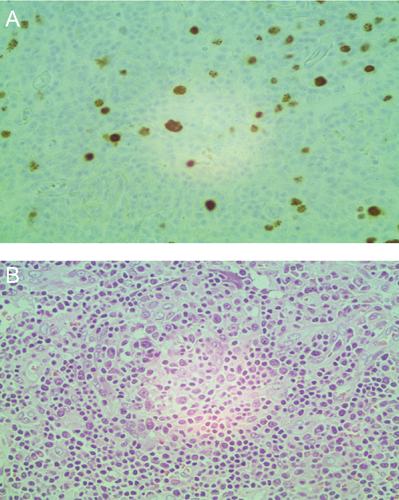
A) Left supraclavicular lymph node: HHV8+ infected plasma cells in lymph node follicle with CD138 and CD79a immunohistochemistry stains. B) Involuted germinal center infiltrated by abnormal plasma cells.
Discussion
Multicentric Castleman's disease has become more relevant in recent years due to its associated with HIV and HHV-8 (Kaposi sarcoma) and its potential to progress into plasmablastic B-cell lymphoma. Dupin
Conclusions
In conclusion, the diagnosis of MCD should be considered in patients with HHV-8 (Kaposi's sarcoma) who present with fever of unknown origin and diffuse lymphadenopathy. 12 The HIV status should always be determined in these cases because it can implicate a different diagnostic, therapeutic, and prognostic approach. Even though MCD occurs with an increased incidence in patients with HIV infection, epidemiologic studies have demonstrated no correlation with CD4 cell count or the use of HAART. A systematic review of all 72 cases of HIV associated MCD published up to 2007 found that 64% of the 48 patients diagnosed with MCD in the HAART era were already on HAART at the time of MCD diagnosis. 13 The progression of MCD to B-cell lymphoma is a concern, especially in patients with HIV infection because it precludes the worst outcome and a high mortality, despite treatment. Hence, further diagnostic evaluation must be performed to rule out this dreaded complication and the early initiation of chemotherapy. The most intriguing part of this case is that MCD occurred in a HIV-positive on HAART and hence a high suspicion is warranted because of the possibly of progression to plasmablastic B-cell lymphoma.