
Abstract
Kaposi’s sarcoma is a well-known multifocal vascular tumor initially described by pathologist Moritz Kaposi. This report presents the case of a 38-year-old bisexual male who consulted the infectious diseases department with non-itchy maculopapular and purpuric lesions on the skin with the involvement of the oral mucosa, suggesting a diagnosis of Kaposi’s sarcoma. Biological and radiological investigations were performed. The patient was found to be human immunodeficiency virus positive with a viral load of 251.000/mL and a CD4 count of 182/mm3. In addition, secondary syphilis was diagnosed. Histopathological examinations confirmed HHV-8 KS. The patient was treated with Extencilline® and antiretroviral therapy. After 10 months of chemotherapy, a favorable outcome was noted with complete resolution of skin and oral mucosa lesions.
Introduction
Kaposi’s sarcoma (KS) is a well-known multifocal vascular tumor initially described by pathologist Moritz Kaposi in 1872. 1 It is the most common neoplasm in patients with acquired immune deficiency syndrome (AIDS). 2 Although its occurrence has significantly decreased in developed countries, KS remains the most frequent tumor in human immunodeficiency virus (HIV)-infected patients worldwide. The average age of patients with KS/AIDS is 38–40 years. 3 HIV-related opportunistic infections and malignancies continue to cause morbidity and mortality in HIV-infected individuals. In this context, we present the case of an HIV infection revealed by mucocutaneous KS and secondary syphilis manifestations in a bisexual male patient.
Case presentation
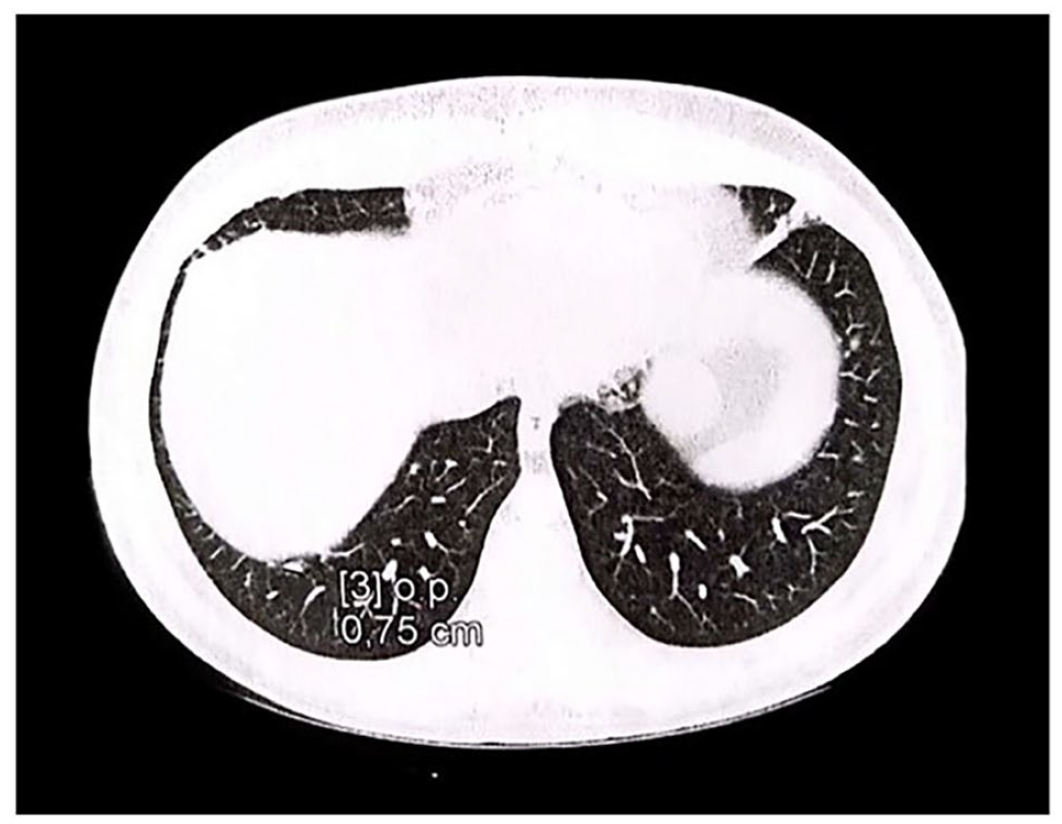
Informed consent was obtained from the patient. The case presentation involves a 38-year-old bisexual male with a medical history of splenomegaly secondary to viral hepatitis. He presented to the infectious diseases department with non-itchy maculopapular skin lesions and fever. He is a non-smoker and occasionally consumes alcohol. Clinical examination revealed maculopapular lesions on the upper and lower limbs, trunk, back, and both feet soles. Purpuric lesions were also noted on the lower 1/3 of both legs, suggesting a diagnosis of KS. No neurological symptoms were recorded. The rapid HIV test was positive. Biological investigations showed WBCs = 5500/mL, lymphocytes = 1200/mL, Hb = 14.1, and platelets = 133.000/mL. Serological examinations for syphilis (VDRL (Venereal Disease Research Laboratory) and ECLIA (ElectroChemiluminescence ImmunoAssay) positive), HIV, and CMV (Cytomegalovirus) (IgM and IgG positive) were positive, while they were negative for hepatitis B, C, and toxoplasmosis. The patient was immunized for hepatitis A (IgM and IgG positive). The diagnosis of HIV was confirmed by a positive serological examination with a viral load of 251.000/mL and a CD4 count of 182/mm3. Secondary syphilis was also confirmed by serological tests. Pulmonary tuberculosis (TB) was ruled out following negative results of the intradermal tuberculin test and the sputum smear test. Indeed, no specific lesions of TB were displayed by the chest X-ray. The patient was treated with Extencilline® 2.4 MUI/week for 3 weeks and started on Atripla® (ART). Histological examination of a skin biopsy from the leg lesions showed a regular epidermis bordering the sample. The dermis exhibited tumoral proliferation of spindle cells without a defined fasciculate architecture and monomorphic nuclei. These tumor proliferations were dotted with vascular slit-like spaces lined directly by spindle cells. Mitoses were rare. Immunohistochemistry analysis revealed the expression of anti-HHV-8 antibodies, confirming the diagnosis of KS (WHO clinical stage 4) (Figure 1 (a) and (b)). Abdominopelvic examination revealed hepato-hilar adenomegaly, common femoral and bilateral inguinal adenomegaly with minor centimetric axis. Chest X-ray and computed tomography scan displayed multiple bilateral solid nodules and micronodules at the lung bases (Figure 2).
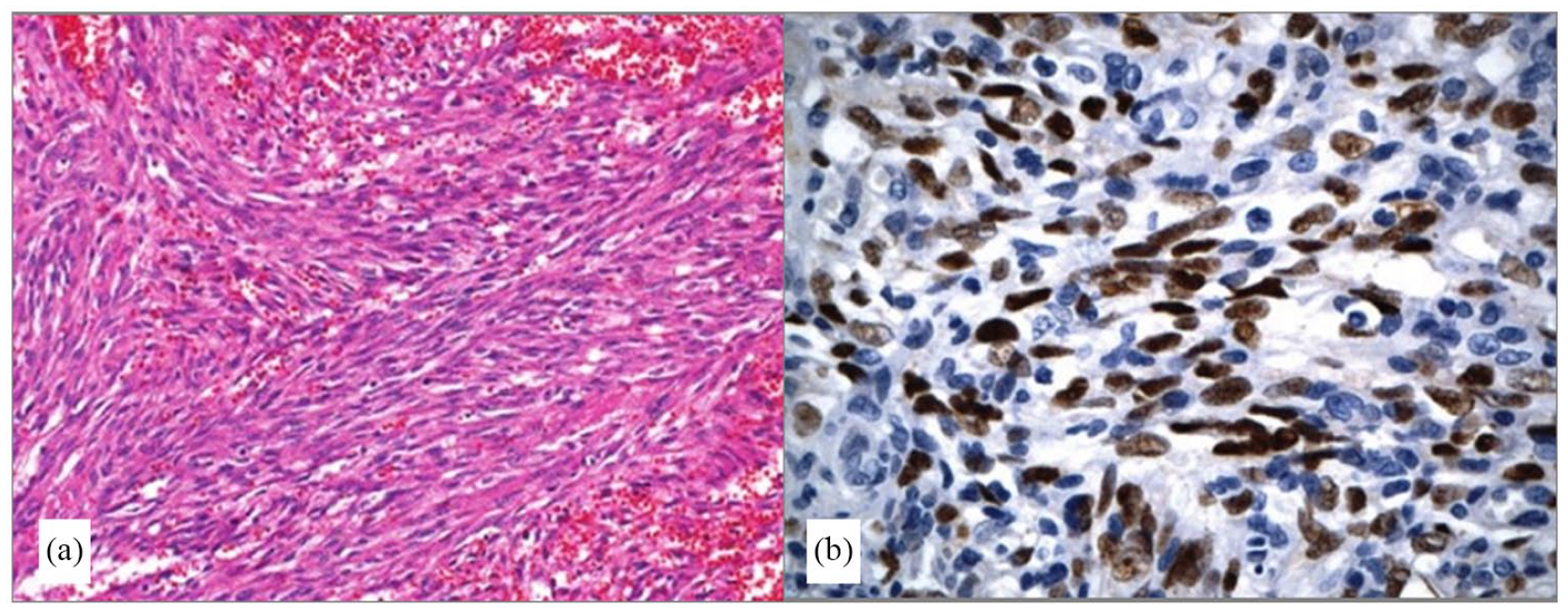
(a) The tumor is composed of intersecting fascicles of uniform spindle cells with intervening blood-filled spaces (HE stain ×100). (b) The tumor cells show strong nuclear immunostaining with HHV8 (immunostain ×400).
A computed tomography scan of the lung in an axial view shows multiple nodules at the lung bases.
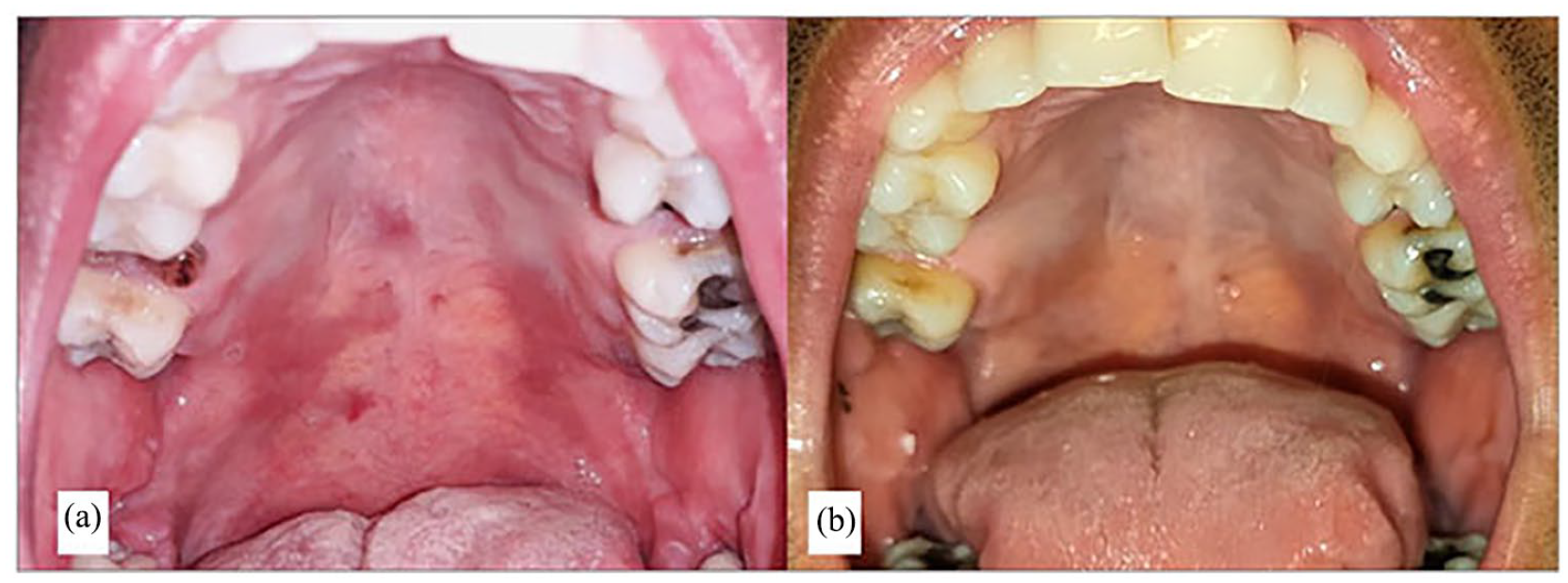
Oral examination in the department of dental medicine revealed maculopapular lesions in the mouth involving the hard and soft palate mucosa (Figure 3(a)). White lesions were also observed on the cheek and tongue mucosa, suggesting HIV-related leukoplakia. In addition, a painful ulcer (1 cm in diameter) induced by cutting edges of the decayed left mandibular first molar was present. The patient also had several decayed and restored teeth, gingivitis, and spontaneous bleeding. An oral examination was completed with a panoramic radiography. Before undergoing chemotherapy, the cutting edges of the decayed first molar were softened and the third left mandibular molar was extracted. The ulcer completely resolved after 1 week. Unfortunately, the patient did not return for further dental treatments. Chemotherapy (Vinblastine® 10 mg) for KS was administered once a week for 10 months (nine sessions) along with ART treatment for HIV. The outcome was favorable, with complete resolution of skin and oral mucosa lesions (Figure 3(b)). Eight months later, lung and abdominopelvic ultrasound revealed complete resolution of the lung solid nodules and micronodules, as well as regression of the size of adenopathies. The patient’s viral load significantly decreased after ART treatment and reached an undetectable level (<38 copies/ml), along with an increase in the CD4 count, indicating good adherence to treatment. VDRL testing was negative after 1 year. After this favorable outcome, the patient was ready to complete dental treatments. He is still monitored by the infectious diseases department.
(a) Clinical view notes maculopapular lesions in the mouth involving the hard and the soft palate mucosa. (b) Clinical view showing complete resolution of the lesions after chemotherapy.
Discussion
This case report concerns a clinical presentation of diffuse mucocutaneous manifestations of KS in a bisexual male, along with secondary syphilis leading to the diagnosis of HIV/AIDS status. KS is the most common neoplasm in homosexual and bisexual men with AIDS. 4 Since the emergence of HIV infection, there has been an increase in the prevalence of opportunistic diseases, especially KS, worldwide. Its incidence in the past was over 20.000 times higher in patients with AIDS than in the general population. The etiopathogenesis of KS is known to include exposure to infectious agents, especially HHV-8, which is found in more than 90% of KS lesions in individuals with AIDS.5,6 A consistent gradual decline in KS incidence has occurred among people living with HIV since the introduction of highly active antiretroviral therapy. 7 On the other hand, syphilis is known to be the “great imitator” and is difficult to diagnose due to its variable clinical presentations, especially in HIV-infected individuals. 8 It is a sexually transmitted disease caused by the spirochete microorganism Treponema pallidum. Syphilis and HIV co-infections are particularly common among men who have sex with men, prostitutes, and intravenous drug users. Although syphilis presentation in patients with HIV is largely similar to that in patients without HIV, differences in its manifestations may be present. 9
A similar case to ours was reported in a patient with syphilis, HIV co-infection, and genital KS. This case reinforces the fact that multiple factors regarding the virus and the patient’s immune system may lead to carcinogenesis. 6 Our patient presented maculopapular lesions on the upper and lower limbs, trunk, back, both feet soles, and on the oral mucosa. Clinically, there are four types of KS based on its biological behavior and morphologic features: nodular, florid, infiltrative, and lymphadenopathic. 10 Patch-stage cutaneous KS should be differentiated from fibrous histiocytoma, targetoid hemosiderotic hemangioma, and interstitial granuloma annulare. As for the plaque-stage KS, the differential diagnosis includes microvenular hemangioma, tufted angioma, acroangiodermatitis (“pseudo-Kaposi sarcoma”), and targetoid hemosiderotic hemangioma. According to the literature, KS has been identified in almost every site in autopsy, but it is mostly present on the skin. Aside from that, the oral cavity, gastrointestinal tract, and lungs are the most common sites where the disease was found. HHV-8 was also located in the peripheral blood mononuclear cells, saliva, oropharyngeal mucosa, semen, cervicovaginal secretions, and prostate glands, explaining its possible vertical and horizontal transmission. 11 Oral manifestations of KS are frequent, and KSHV DNA was detected in oral cells. Indeed, it was reported that untreated HIV patients who develop KS of the oral cavity are exposed to higher death rates than patients affected only in the cutaneous area.12,13 KS can occur at any stage of HIV infection, but it is more likely to take place at a lower CD4+ T-cell count. Our patient had a CD4 count of 182/mm3 with oral, cutaneous, and pulmonary manifestations. Even though in the era of new ART, the majority of cases of KS occur in the late phases of HIV infection. It is worth noting that KS was also observed in a patient on successful long-term ART, with well-controlled HIV infection and a CD4+ count >200/mm3. 14 Based on previous studies, the immune system of patients with long-term infection with HIV is no longer capable of controlling KSHV (Kaposi Sarcoma-associated HerpesVirus), which could eventually represent a possible “new” epidemiologic phenomenon, given the growing number of well-controlled people living with HIV. However, in these patients, the clinical presentation is much less aggressive in comparison with KSHV in untreated patients. 15
As for the treatment, standard KS therapy has not changed in the last years; however, newer modalities are discussed depending on the extent and rate of tumor growth, disease stage, lesion distribution and evolution pattern, symptoms, immune status, and concurrent complications of HIV infection. 16 Recent studies have stipulated the contribution of cytokines and HIV in the pathogenesis of KS. The presence of KSHV is the primary and fundamental factor in the development and occurrence of this tumor. Furthermore, immunosuppression in the host seems to play an important role as a cofactor in the clinical expression of KS in some KSHV-infected patients. This exponential relation between clinical lesions and immunosuppression underscores the unusual pathology and clinical course of this proliferative disease and hints that KS may not be a conventional neoplasm. 17
Conclusion
Diagnosis of HIV in an immunocompromised patient with a malignant tumor and an opportunistic infection still occurs despite the introduction of ART. Understanding the relationship between HIV, HHV8 infection, and syphilis in terms of clinical presentations and disease progression is important to ensure appropriate treatment planning and management. Clinical staging represents the most important factor for choosing the optimal treatment plan with a multidisciplinary approach. The role of the dentist is crucial in confirming the oral location of the tumor and in removing infectious foci from the mouth before chemotherapy initiation.
Footnotes
Acknowledgements
The authors thank the patient for his precious contribution.
Author contributions
All authors made a significant contribution to the case reported whether that is in the conception, data collection, and paper drafting. All authors have read and agreed on the journal to which the article has been submitted.
Data Availability Statement
Data related to clinical and biological investigations are available upon request from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The International Association for Dental, Oral and Craniofacial Research (IADR, ![]() ) funds this study in the context of the Regional Development Program Award ($18,290) in 2021.
) funds this study in the context of the Regional Development Program Award ($18,290) in 2021.
Ethical approval
Ethical approval to report this case was obtained from the committee of ethics of the faculty of pharmacy, University of Monastir, Tunisia, under the reference CER-SVS/ISBM 013/2020. The present case report is part of Latifa Berrezouga’s research project on PLHIV.
Informed consent
Written informed consent was obtained from the patient(s) for their anonymized information to be published in this article.