
Abstract
Esophageal schwannoma is a rare tumor first described in 1967 by Chaterlin and Fissore. These tumors are most commonly found incidentally or from diagnostic work up of dysphagia or dyspnea. This entity cannot be diagnosed on clinical or radiographic basis alone. Histology demonstrates palisading spindle cells, few if any mitotic figures, and a peripheral cuff of lymphoid cells. Immunohistochemically, tumor cells stain positive for S100, a characteristic marker of Schwann cells. Once diagnosed, surgical enucleation is the typical treatment method employed.
Keywords
Case Report
A 69-year-old female with a history of coronary artery disease, recurrent pneumonias, mild dysphagia and gastroesophageal reflux presented with a productive cough and fever for three days. The patient was started on moxifloxacin for presumed pneumonia. The chest radiograph did not demonstrate any consolidations however a subsequent non-contrast chest computed tomography (CT) confirmed the presence of pneumonia as well as incidentally identified an esophageal mass at the level of the thoracic inlet causing anterior displacement of the trachea and luminal narrowing of both the trachea and esophagus (Figure 1A-C).

Axial (A), sagittal (B), and coronal (C) images from a noncontrast chest computed tomography demonstrating an esophageal mass at the level of the thoracic inlet, exerting mass effect on the trachea and esophagus. D) Posteroanterior image from an esophagram demonstrating a smooth rounded indentation of the proximal esophageal lumen which did not impede passage of orally administered barium.
A barium swallow was performed which demonstrated a smooth rounded indentation of the proximal esophageal lumen which did not impede passage of orally administered barium (Figure 1D).
Esophagogastroduodenoscopy excluded an intraluminal origin of the mass and confirmed esophageal compression was extraluminal. Bronchoscopy excluded endobronchial pathology and a left cervical exploration with enucleation of the esophageal mass was subsequently performed. Gross examination revealed an elongated nodular mass measuring 5.0×2.3×2.0 cm with a smooth uniformly yellow surface. The mass was dissected off of the muscular layers without complication, leaving the mucosa layer intact. Microscopic examination demonstrated the mass to be composed of spindle cells with a prominent lymphoid cuff peripherally (Figure 2).
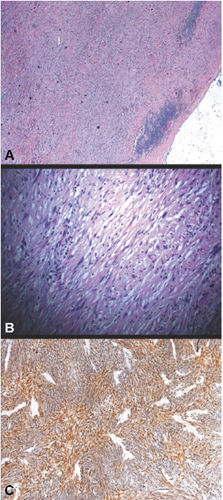
A) Low power microscopic examination demonstrating spindle cells with a prominent lymphoid cuff peripherally. B) High power microscopic examination demonstrating spindle cells. C) Immunohistochemical analysis demonstrating cells staining strongly positive for S100.
There was no necrosis or hemorrhage. Immunohistochemically, the mass was strongly positive for S100 (Figure 2), and was diagnosed as an esophageal schwannoma. The patient had an uneventful postoperative course.
Discussion
Esophageal schwannoma is a rare tumor which can demonstrate benign or malignant features. This entity was first described in 1967 by Chaterlin and Fissore, 1 and to date, less than 30 cases have been described in the English literature, four of which have been shown to demonstrate malignant characteristics. 2 Murase et al. and Sanchez et al. reported two cases in which lymph node metastasis occurred from a primary esophageal schwannoma.3,4
These rare tumors predominantly present in the 5th-6th decades of life and demonstrate a female-to-male ratio of approximately 4 to 1. 2 In 2011, Choo et al. had reported the youngest case of esophageal schwannoma, describing a 22-year-old Asian American male complaining of dyspnea with progressive development of dysphagia. 5 Of the cases described, there is a strong predominance for this disease entity in the Asian population, with 16 of 25 cases reported from Asian institutions in a 2011 study by Kassis et al. 2
Typically dyspnea and dysphagia are the most common presenting symptoms however other reported signs and symptoms include chest pain, stridor, hematemesis, cough and a palpable neck mass. Strictly on a clinical and radiologic basis this entity is impossible to definitively diagnose. On CT, the lesion is well marginated, and homogeneous in attenuation which may or may not show enhancement. 6 This is indistinguishable from the more common esophageal leiomyoma. Diagnosis is made on histological and immunohistochemical basis. Histologically, esophageal schwannomas are typically characterized by palisading spindle cells, few or absent mitotic figures, and a peripheral cuff of lymphoid cells containing germinal centers. Immunohistochemically, tumor cells stain positive for S100, a characteristic marker of Schwann cells. Markers such as CD117 and CD34 will be negative, differentiating it from gastrointestinal stromal tumors (GIST). Smooth muscle cell markers, actin and desmin, will also be negative, differentiating it from leiomyomas.2,5–8 Several histologic characteristics may be useful in distinguishing malignant schwannomas from benign, including mitotic figures, nuclear atypia, cellularity and tumor necrosis. Of these it is believed greater than 5 mitotic figures in 50 high-power fields is the most reliable indicator of malignancy. 8 Additionally, the utility of PET imaging for evaluating malignity of such lesions had been postulated, however in 2009 Matsuki et al. concluded there was no correlation between malignant potential and fluorodeoxyglucose uptake. 9 The treatment for esophageal schwannomas is surgical resection, with the approach dependent on tumor size. Very small well demarcated lesions can be removed endoscopically, although typically surgical enucleation is performed. In cases of local invasion or mucosal involvement, esophagectomy and local lymph node dissection have been reported. 8
Conclusions
Esophageal schwannomas are rare mediastinal tumors that are typically benign and are either found incidentally or because of symptoms from mass effect. A definitive diagnosis is made by histology. Treatment is typically surgical enucleation and the prognosis is excellent.