
Abstract
Since nasal NK/T-cell lymphoma and NK/T-cell lymphoma nasal type are rare diseases, colonic involvement has seldom been seen. We report a case of a patient with a primary NK/T-cell lymphoma nasal type of the colon. The patient had no history of malignant diseases and was diagnosed after exhaustive study in the context of fever of unknown origin. The first therapeutic approach followed the DA-EPOCH-protocol: etoposide, prednisone, doxor-rubicin, vincristine and cyclophosphamide. The persistence of constitutional symptoms after the first treatment course motivated the switch to a second line following the SMILE-protocol: dexamethasone, metotrexate, ifosfamide, E.coli L-asparaginase, and etoposide. Despite intensive chemotherapy, the patient died 2 months after the diagnose of an extranodal NK/T-cell lymphoma of the colon and 4 months after the first symptomatic appearance of disease.
Introduction
Extranodal NK/T-cell lymphoma, nasal type, is a rare and severe disease which is more frequent in Asia and South America. It is thought to arise from natural killer (NK) cells or, occasionally, from a subset of or cytotoxic T cells and it shows striking association with Epstein-Barr virus (EBV). Usually, extranodal NK/T-cell lymphomas primarily involve the nasal cavity or other parts of the upper aerodigestive tract but sometimes occur in extranasal sites without involving the nasal cavity or nasopharynx. The World Health Organization classification has proposed the term nasal type to describe both the disease that arises in the nasal cavity and in the extranasal sites. 1 The nasal/ nasopharyngeal localization represents 75% of the cases. Other sites involved are the skin (4%), the gastrointestinal tract (6%), the bone marrow and the spleen. 2 NK/T-cell lymphoma nasal type is diagnosed by immunophenotyping. The typical phenotype has been described as CD2+, CD3/Leu4−, CD3 +, CD3–, CD56+, TCR germline and generally EVB+. Based on histological criteria, angiocentric and/or angiodestructive behavior with admixed cell morphology (small, medium and large cells) is often found. 2 This type is known to be highly aggressive and associated with a very poor prognosis in advanced cases. 3 Primary colonic lymphomas, especially NK/T-cell nasal type, are rare even in the most numerous reported series from China and India.4–6 There is no consensus treatment. Localized NK/T-cell lymphomas often respond to radiotherapy.1,7 In contrast, patients who have extensive disease or who relapse after radiotherapy have a very poor outcome.1,8
We report the unique case of a primary colonic nasal type NK/T-cell lymphoma that represented a diagnostic challenge and had an ominous outcome despite intensive treatment.
Case Report
A 52-year old Caucasian male was admitted with fever and constitutional symptoms. He had a past medical history of hypertension, asthma, tobacco addiction and a cardiac surgery because of a severe coronary disease five months before the mentioned admission. After the cardiac surgery, he developed cellulitis in the site of the surgical safenectomy that was successfully treated with antibiotics according to the bacteriological growth. In the previous three weeks, the patient referred fever with chills, initially without a regular pattern. Because of the persistence of an eritematous area over the safenectomy scar, and after taking blood and urine cultures, an empirical treatment with cephalosporins was initiated. Despite antibiotics, fever persisted in peaks up to 40°C, now accompanied by constitutional symptoms that motivated the admission to further evaluation. Several cultures were persistently negative. He was studied with a sonography of the soft tissue that showed neither collections nor thrombosis, a trans-esophageal ultrasound that showed no vegetations and a moderate deterioration of the ventricular ejection fraction (31%). A computed tomography (CT) scan showed an enlarged sigmoid as unique pathologic finding, rectal wall with rarefaction of the perisigmoid adipose tissue and adenomegalic regional lymph nodes (intercavo-aortic, para-aortic and bilaterally, peri-common iliac arteries). The physical examination was negative and there was no correlation with the CT findings. A colonoscopy examination was performed. A small ulceration of the mucosa was found at the recto-sigma union, giving the macroscopic impression of an ischemic lesion (Figure 1). The ulceration was biopsied and the immunophenotyping revealed a T (CD3+, CD5+ and CD45RO+) lymphoproliferative process. The only remarkable laboratory data were a mild normocytic normochromic anemia, elevated alkaline phosphatase (454 UI/L), and elevated PCR (345 mg/L) with normal LDH levels. The surgical resection of the involved area was performed sixty days after the beginning of the constitutional symptoms (Figure 2) and a week after the colonoscopy. Because of the alkaline phosphatase levels, hepatic biopsies were also taken. A laparoscopic sigmoidectomy was performed with a termino-terminal anastomosis. There was no macroscopic lesion in the resected tissue. Thus, the topographic area to be biopsied was estimated with the information provided by the colonoscopy. The pathological examination revealed a high grade lymphoma infiltrating the medium and large size vessels walls and also intravascular presence of the same elements with complete involvement of the vascular structure. The subserosal adipose tissue was also infiltrated with extended areas of atypical lymphoid elements associated with necrosis and hystiocytosis. The regional lymph nodes showed the same atypical medium and large-size elements with irregular nucleus in the sinus T area. Inmunohistochemistry revealed positivity for CD2, CD56 and weak expression of CD20, as well as negative stain for CD30. A CD3 stain was also positive intra-cytoplasmatic. The neoplastic cells showed strong granular staining for the cytotoxic molecules granzyme B and perforin. The EBV stain, revealed strong cytoplasmatic and surface membrane expression in almost all lymphoma cells. The Ki67 positivity was estimated around 40% (Figure 3). A NK/T cell lymphoma, nasal type extranodal and extranasal was diagnosed. The liver showed no lymphomatous involvement. The patient underwent the usual staging examinations with clinical exam. A CT assessment of the neck completed the assessments of chest, abdomen and pelvis already performed, a bone marrow biopsy, and the evaluation of the cerebrospinal fluid. None of these assessments uncovered another involved site. In particular, the nasal and nasopharyngeal regions as well as the bone marrow were free of disease. The patient had no history of celiac disease and serological analysis was negative for specific antibodies. The patient had a stage IIB E, IPI 2 before the start of the therapy. Chemotherapy using the DA-EPOCH protocol (etoposide, prednisone, doxorrubicin, vincristine, cyclophosphamide) was applied and the therapy was well tolerated by the patient. He developed grade IV hematotoxicity but presented no infectious complications after the first course. He persisted with B symptoms, though. The persistence of constitutional symptoms as well as the nature of the lymphoma were the reasons to change the treatment protocol to one containing L-asparaginase. The second course of therapy followed the SMILE-protocol combining dexamethasone, 40 mg/body intravenously on days 2–4; metotrexate, 2 g/m2 intravenously over 6 h on day 1; ifosfamide, 1.5 g/m2 intravenously on days 2–4; E.coli L-asparaginase, 6000 U/m2 on days 8,10,12,14,16,18, and 20; and etoposide, 100 mg/m2 intravenously on days 2–4. 9 The schema was well tolerated by the patient. He presented fever, and grade 4 neutropenia and mucositis on day 14 post chemotherapy. Supportive care was provided with antibiotics, parenteral support, transfusion of hemocomponents and G-CSF. Despite all efforts, the patient died of a multiple organ dysfunction due to a refractory septic shock, after 9 days of intensive treatment, 2 months after his diagnose and 4 months after the unspecific symptoms begun.
Endoscopic appearance of primary colonic NK/T-cell lymphoma: marked mucosal and submucosal edema of the recto-sigma union with a small ulcerative lesion pointed by a black arrow.
Macroscopic view of the colonic resection: showing no alteration of the external appearance of the organ, although the mucosa looks homogeneously white, pale and edematous with the typical fish-meat like appearance.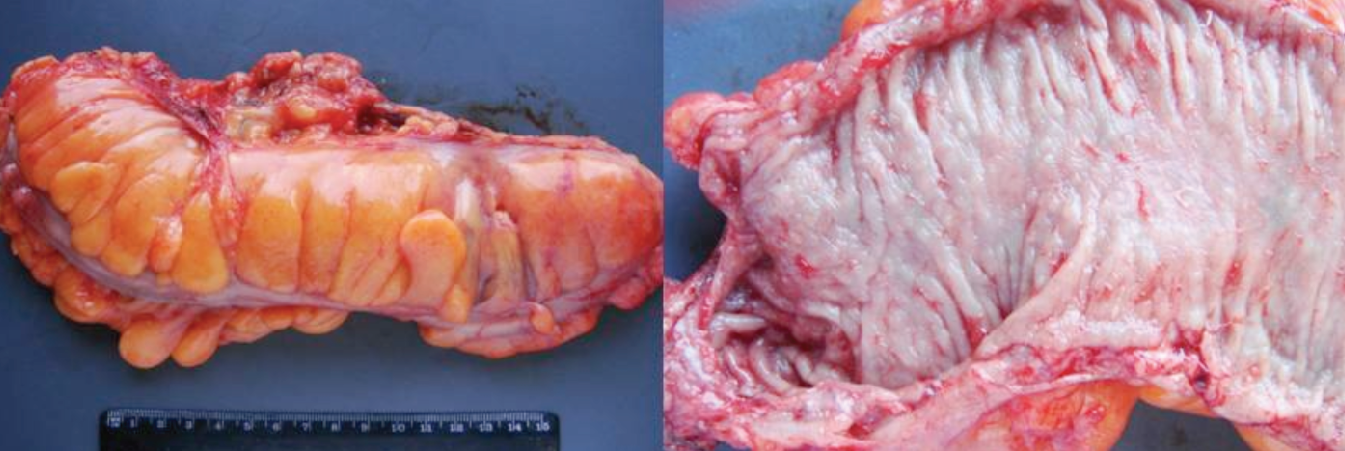
Haematoxylin & Eosin staining of a section containing a small artery (upper left), in which the lymphoma's angioinvasive behavior is clearly depicted. The immunostaining with monoclonal antibodies directed against CD3, CD56, CD2, granzime B, perforine and EBV were positive in the infiltrating cells with an estimated Ki67 positivity around 40% on the neoplastic NK/T-lymphocytes.
Discussion and Conclusions
Patients with extranodal NK/T-cell lymphoma have a cumulative 5-year survival probability of around 40%. Although involved-field radiotherapy seems to be the preferred option for localized disease, this therapy remains poorly effective, with the suggestion that high-dose irradiation associated to combination chemotherapy with P-glycoprotein (P-gp)-unrelated agents may give better results. 1 Chemotherapy protocols generally used to treat lymphomas of other histological subtypes have very little efficacy in patients with disseminated disease or disease recurrence after radiotherapy.
The mechanism of extranodal NK/T-cell lymphoma resistance to conventional chemotherapy is not fully understood, but could be related to the frequent expression of P-gp by lymphoma cells, which is responsible for the multidrug resistance phenotype. 10
L-asparaginase is not affected by multidrug resistance and has an original antitumoral mechanism: tumor cells unable to synthesize L-asparaginase die when their stores of L-asparagine are depleted by L-asparaginase.
We compared the findings in the present patient with a recent analysis on the largest series of KN/T-cell lymphoma. 11 As it was seen in this collective, CD2, CD3e, granzynme B and CD56 stainings were positive. Although CD30 was negative in our extranasal case, it was negative in 37% of cases in this series and it is not a prerequisite according to WHO classification. The EBV positivity was an obligatory inclusion criterion in this study. Its strong expression in the present case points towards an EBV-associated lymphoma. In EBV-associated lymphoid malignancies, increases in circulating EBV DNA are normally found, due to viral DNA release from apoptosis of proliferating tumor cells. Serial EBV DNA quantifications by quantitative polymerase chain reaction in NK cell lymphoma have been found to correlate with disease control.3,12,13
Several authors have advocated the establishment of a prognostic model for NK/T-cell lymphoma nasal type that is more reliable than IPI (International Prognostic Index).11,14 Factors significantly associated with a worse prognosis are male gender, the presence of B-symptoms, high LDH, advanced stage and CD30 negativity. In our case, the patient possessed all negative prognostic factors except the advanced stage. We did not perform a PET-CT, which might have been useful to detect uncovered compromise, considering the high avidity for fluorodesoxyglucose (18F; 18F-FDG) of this lymphoma. 8 The patient died shortly after diagnosis. Past experiences with the CHOP-regimen indicated that it might not be an adequate therapeutic approach for advance stage disease. Some authors have suggested high-dose chemotherapy associated with autologous or allogeneic transplantation for patients with NK/T-cell lymphoma nasal type and poor prognosis.1,7–9,15 The optimal treatment strategy of NK cell lymphoma remains not well defined. With the increased understanding of these malignancies, several important principles have nevertheless emerged. 8 For nasal NK cell lymphomas, the best treatment results are obtained with a combination of chemotherapy and radiotherapy. Chemotherapy is the mainstay of treatment for non-nasal NK cell lymphoma. In this particular reported case, the election of the infusional DA-EPOCH protocol as first line intended to intensify the CHOP scheme, whose combination of drugs has been reported efficacious, although it is probably not the best therapeutic approach for advance stage disease.8,9,15 The bulk of information documenting the superiority of the SMILE-protocol above other therapeutic approaches was at that time scarce. This is the reason why we kept that option as second line in case of progression or relapse. In our reported case, the persistence of B-symptoms after the first course of DA-EPOCH and the presence of adverse prognostic factors, motivated the change to the SMILE- protocol for the second course. 9 To our knowledge, this patient is the second report of primary NK/T-cell lymphoma of the colon. Recently, the group of Shumei Zheng et al. 6 has analyzed the clinical data of 25 Chinese cases with the diagnose of primary intestinal NK/T cell lymphoma, representing the most important series reported. The patients represented all hospitalized patients with diagnosis of primary intestinal NK/T cell lymphoma admitted at the West China Hospital of Sichuan University between May 1999 and May 2010. Twenty from the 25 reported cases had primary involvement of the colon. Clinically, the most common symptoms were abdominal pain (60%), fever (56%) and weight loss (56%). These symptoms were also present in our reported case. In the reported series, the majority of the patients (64%) presented the lymphoma localized to one site. As well as in our case, in the 84% of the cases, the identified lesion was an ulcer. Endoscopically, intestinal NK/T cell lymphomas most commonly showed focal, multifocal or diffuse pleomorphic ulcers that most frequently occurred in the ascending colon. 64% were either Stage IIIE of Stage IVE at diagnose. The authors described also their difficulties to achieve an early diagnosis, because the lymphoma might mimic intestinal tuberculosis or Crohn's disease in some cases. Furthermore, in some of the described cases the endoscopic biopsy failed confirm the diagnosis, despite the clinical suspicion of intestinal malignant lymphomas, Twenty percent of the patients were misdiagnosed as ulcerative colitis, Crohn's disease, intestinal tuberculosis, peptic ulcer and duodenal carcinoma. All patients that were in clinical conditions to receive chemotherapy underwent chemotherapy following CHOP protocol and after a median follow-up of 7 months, 3 of 25 patients were alive. To date, no conclusive theory has been described to explain why this type of lymphoma remains confined to these unusual locations. Furthermore, the extranasal disease has a poor clinical outcome for all prognostic subgroups. 11 Hence, primary extranasal disease per se should lead to consideration of novel therapies.