
Abstract
Since nasal NK/T cell lymphoma and NK/T cell lymphoma nasal type are rare diseases, gastric involvement has seldom been seen. We report a unique case of a patient with a primary NK/T cell lymphoma nasal type of the stomach with skin involvement. The patient had no history of malignant diseases and was diagnosed with hematemesis and intense bleeding from his gastric primary site. Shortly after this event, exanthemic skin lesions appeared with concordant histology to the primary site. Despite chemotherapy, the patient died one month after the first symptomatic appearance of disease.
Introduction
According to the WHO classification of lymphoma, the NK cell type can be classified into 3 subgroups: NK/T cell lymphoma nasal/nasal type, NK cell leukemia and chronic lymphoproliferative disorders of NK cells.1,2 Among non-Hodgkin's lymphomas, NK/T cell lymphoma nasal type is a very rare subtype, predominantly found in East Asia. There it makes up 2–10% of NHL (non-Hodgkin's lymphoma). 3 It is primarily located in the nasal/nasopharyngeal region (75%), the skin (4%), the gastrointestinal tract (6%), the bone marrow and the spleen. 4 NK/T cell lymphoma nasal type is diagnosed by immunophenotyping. The typical phenotype has been described as CD2+, CD3/Leu4−, CD3ε+, CD3−, CD56+, TCR germline and generally EBV+. 5 Based on histological criteria, angiocentric and/or angiodestructive behavior with mixed in cell morphology (small, medium and large cells) is often found. 6 This type is known to be highly aggressive and associated with a very poor prognosis in disseminated disease. 7 Primary gastric lymphomas are rare, especially of the NK/T cell nasal type. 8 According to literature only 2 cases of primary gastric NK/T cell lymphoma nasal type have been reported.9,10 These patients did not show involvement of other sites except stomach. They died shortly after diagnosis.
Case Report
A 69-year old Caucasian man was first hospitalized with hematemesis and melena. The endoscopic examination revealed a bleeding duodenal ulcer, Forrest 1a and a second ulcer in the antrum of the stomach (Figure 1). Biopsies were taken from the gastric ulcer. The pathological examination revealed a high-grade lymphoma of the stomach. Roughly, the histomorphology showed an angiocentric and angiodestructive growth pattern with a mixed cell population accompanied by a heavy admixture of inflammatory cells. Immunohistochemistry revealed positivity for CD2, CD56, and a weak expression of CD20, as well as a negative stain for CD4, CD5, CD7, CD8, CD30, CD33, CD34, CD79a, CD103, CD117 and CD138 (Figure 2). A CD3ε, stain on a fresh tissue sample was also positive. The neoplastic cells showed strong granular staining for the cyto-toxic molecules granzyme B, perforin and TIA1. The immunostaining with a monoclonal antibody for the anaplastic lymphoma kinase (ALK) was negative. The molecular analysis of the TCR γ-chain-locus showed a germline configuration. By analyzing the samples for IgH gene rearrangement by PCR analysis, no clonal rearrangement could be found. 11 Although EBER (EBV encoded small nuclear RNAs) expression was negative which is an unususal finding for nasal NK-T-cell lymphoma; we performed an LMP-1 stain, revealing strong cyto-plasmatic and surface membrane expression in almost all lymphoma cells. Therefore, presence of an EBV-related lymphoma could be concluded. A NK/T cell lymphoma, nasal type with partial aberrant expression of CD20 was diagnosed. The patient underwent the usual staging examinations with clinical exam, computertomographic assessment of the chest, the abdomen and the pelvis, a bone marrow biopsy and a positron emission tomography. None of these assessments uncovered another involved site. In particular, the nasal and nasopharyngeal regions as well as the bone marrow, were free of disease. No lymphadenopathy was found. The patient had no history of celiac disease and serological analysis was negative for specific antibodies. The LDH was 865U/L at time of diagnosis. The patient's medical history was insignificant apart from newly diagnosed diabetes and the loss of 10% body weight in the previous four months rated as B-symptoms. The patient met the Dawson criteria for primary intestinal lymphoma. 12
Endoscopic appearances of primary gastric NK−/T-cell lymphoma: ulcerative type.
Immunostain-ing with monoclonal antibody directed against CD56 (A) and CD2 (B). Nearly all the stomach infiltrating cells were positive.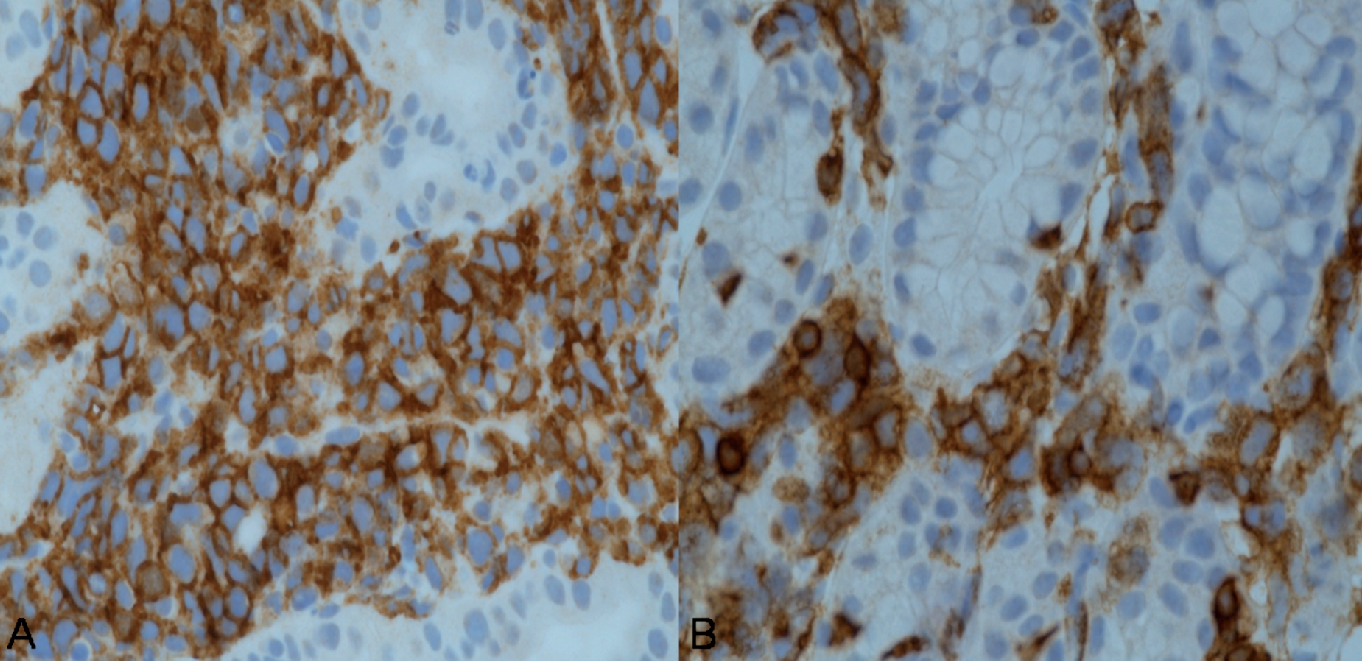
In addition, shortly after the symptomatic appearance of his disease, the patient developed exanthemic non-pruriginous skin lesions. A biopsy was performed and the immunohistochemical assessment showed the same expression profile as described above (Figure 3). Dermal spread of the NK/T cell lymphoma nasal type was concluded. It can be deducted that the patient had a stage IVB disease before the start of the therapy.
Immunostain-ing with monoclonal antibody directed against CD56 (A) and CD2 (B). About 80% of the skin infiltrating cells were positive.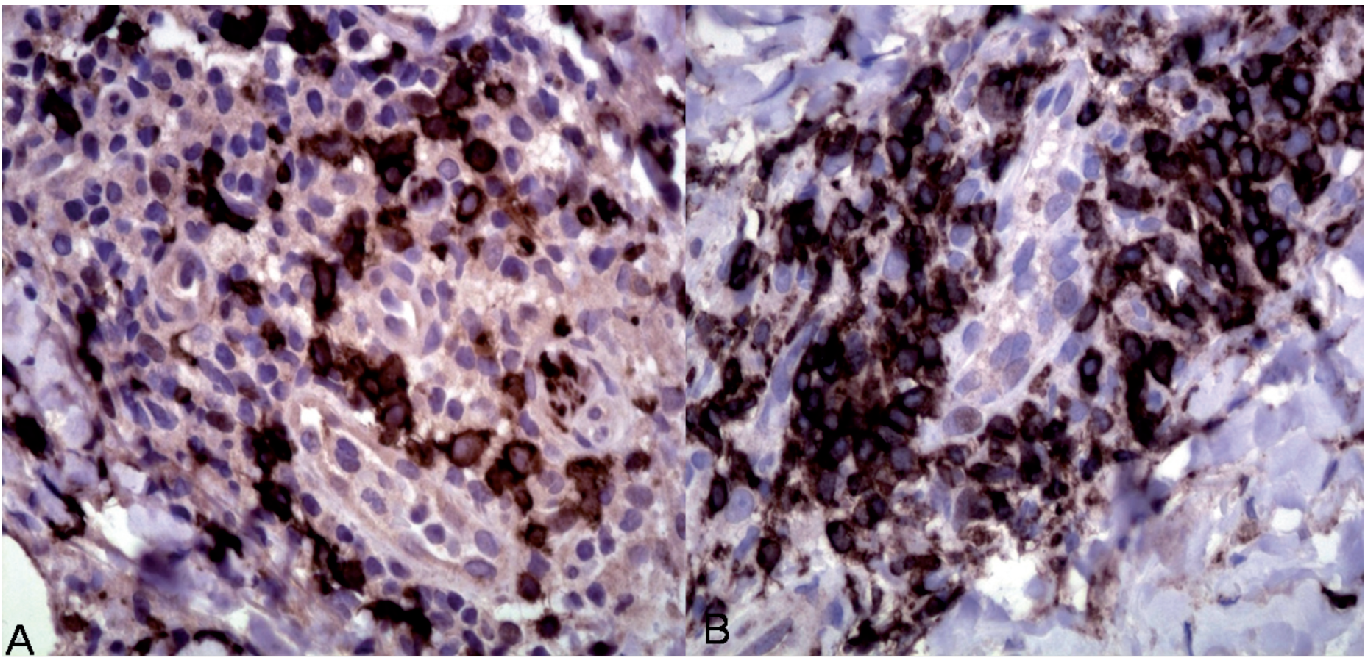
Chemotherapy using the CHOP-protocol (cyclophosphamid, hydroxydaunorubicin, oncovin, prednison) was applied and well tolerated by the patient. About a week later, the patient developed grade IV hematoxicity, becoming aplastic and septic. Supportive care was provided with antibiotic escalation and parenteral support. Meanwhile skin infiltration increased with several new lesions. Despite all efforts, the patient died of septic complications, mostly due to a severe pneumonia. The patient's relatives declined autopsy.
Discussion
The presence of this rare tumor lead us to various differential diagnoses. First, an anaplastic large cell lymphoma (ALCL) was discussed. According to the latest WHO classification, these lymphomas are CD30 positive, and are in 80% of all cases ALK positive. As the present lymphoma completely lacked expression of these markers, an ALCL could be excluded. Enteropathy-associated T-cell lymphoma (EATL) was then taken into consideration. The WHO 1 defines the polymorphic form (type I) of EATL as CD3+, CD5−, CD7−, CD8+/−, CD4−, CD103+, TCRβ+/− and cytotoxic proteins positive. The monomorphic form (type II) is defined as CD3+, CD4−, CD8+, CD56+ and TCRβ+. The lymphoma cells were completely negative for these markers except CD56 and the cytotoxic proteins. These markers are insufficient for the diagnosis of EATL. 1 A primary cutaneous γ-δ T-cell lymphoma was excluded because of the negativity for CD3 and the TCR germline configuration, required for diagnosis by the WHO classification. 1 Finally, a peripheral T-cell lymphoma not otherwise specified was considered due to the typical involvement of skin and stomach. 1 CD4+ and clonal TCR gene rearrangement is most frequently seen, in contrast to the present case, albeit a false negative TCR rearrangement and a negative stain for CD4 have been described before. 1 In addition, a peripheral T-cell lymphoma not otherwise specified could only be diagnosed if other lymphoma types are ruled out. As the morphology didn't match the typical morphology of such a peripheral T-cell lymphoma we didn't favor this diagnosis. Because of the CD20 positivity, a B-cell lymphoma was considered, but given the negativity for CD79a and a lack of clonal IgH gene rearrangement associated with the above mentioned immunohistochemical profile, a B-NHL seemed very unlikely. An aberrant expression of CD20 was concluded.
We compared the findings in the present patient with a recent analysis on the largest series of NK/T-cell lymphoma. 13 As was seen in this collective, CD2, CD3ε, TIA-1, granzyme B and CD56 stainings were positive. Although CD30 was negative in our extranasal case, it was negative in 37% of cases in this series and it is not a prerequisite according to WHO classification. The germline configuration of TCR fits into the findings of this series, as most extranasal cases were found negative for TCR rearrangement. The EBER positivity was an obligatory inclusion criteria in this study. The strong LMP-1 expression of the present case, which points towards an EBV-associated lymphoma, can easily weigh out the EBER negativity for EBV diagnosis.
Finally the immunophenotype of this particular tumor concurred only with an extranodal NK/T-cell lymphoma nasal type. The EBER-negativity could be explained by a low quality of preservation of the paraffin wax-embedded blocks 14 or by a lack of expression of EBER-1, as has been reported in other tumors.14,15 Our findings argue in favor of the combination of EBER and LMP-1 analysis to assess EBV status of lymphomas, as is recommended in Hodgkin's lymphomas. 16
Several authors have advocated the establishment of a prognostic model for NK/T cell lymphoma nasal type that is more reliable than IPI1,7,17,18 (International Prognostic Index). Factors significantly associated with a worse prognosis are male gender, the presence of B-symptoms, high LDH, advanced stage and CD30 negativity. In our case, the patient possessed all negative prognostic factors and died shortly after diagnosis.
Past experiences with the CHOP-regimenindicated that it might not be an adequate therapeutic approach for advanced stage disease. 19 Some authors have suggested high-dose chemotherapy associated with autologous or allogeneic transplantation for patients with NK/T cell lymphoma nasal type and poor prognosis.20,21 In this case, the general condition of the patient at the start of the therapy did not allow such an aggressive approach. Therefore, the standard CHOP therapy was chosen in order to improve the overall condition of the patient. 22
To our knowledge, this patient is a unique case of a primary NK/T cell lymphoma of the stomach with skin involvement. To date, no conclusive theory has been described to explain why this type of lymphoma remains confined to these unusual locations. 22 We hope that our experience might help in the understanding of this very rare disease.