
Abstract
Leiomyosarcoma (LMS) is a rare malignant tumor of smooth muscle origin that generally stems from soft tissues and uterine tissue. Although, a small percentage of these may originate from the smooth muscle or vessel walls, most of which are of venous origin. Renal leiomyosarcomas may arise from the smooth muscle fibers of renal pelvis, renal capsule or renal vessels, last one is the most frequent. We report a case of renal LMS that could be originated in the renal capsule.
Case Report
We present the case of 69-year-old woman who was found to have a large left abdominal mass in evaluation for diffuse abdominal pain accompanied by asthenia and nauseas. Non abnormalities were observed in routine laboratory examination, except a ferriprive anemia: hemoglobin 10.8 mg/dL (12-14 mg/dL). A computed tomographic scan imaging demonstrated an 18 cm lesion from the left kidney; no thrombus in renal vein or cava and neither regional lymph nodes or adrenal gland involved were informed (Figure 1). Open right radical nephrectomy by lumbotomy without lymph adenectomy (intraoperatively no grossly visible lymph nodes were identified) was performed. The surgical specimen revealed a solid multinodular mass measuring 18×15 cm (Figure 2) which probably originates in the renal capsule (Figure 3). The histopathogical examination demonstrated a renal high-grade leiomyosarcoma, which renal capsule infiltration but without extend over there (Figure 3A), and did not extend to pelvis, renal vein or adrenal gland. All excised hilar fat lymph nodes were free of disease. The immunohistochemical profile with smooth muscle actine was difusely positive (Figure 3B). Focal immunostaining were found for desmin, vimentin and CD117 (KIT). No immunostaining were observed for melan A, HMB-45 and S-100 protein. Adjuvant chemo therapy was not performed based upon not data in survival benefit. Five years after the operation, she was in good health with no sign of recurrence or metastases.

Computed tomographic scan imaging: mass in upper pole of left kidney.

Surgical specimen. Tumor in capsule of upper renal pole.
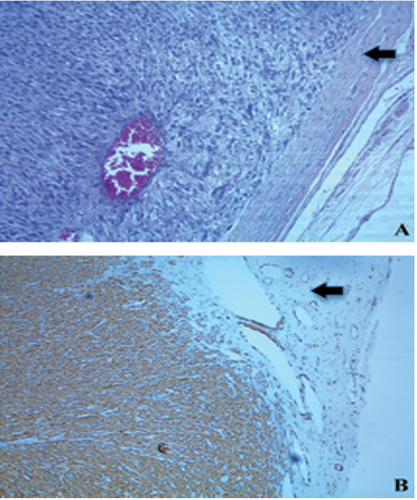
Microscopic examination of the tumor. A) Hematoxilyn-eosin staining demostrating high-grade sarcomatoid cells. B) Immunohistochemistry showing difuse actin expression in smooth muscle fiber cytoplasm. Renal capsule (arrow).
Discussion
Primary sarcomas constitute from 0.8 to 2.7% of renal tumors in adults. 1 Renal leiomyosarcomas may arise from the smooth muscle fibers of renal pelvis, renal capsule or renal vessels, last one is the most frequent. 2
Leiomyosarcoma of the kidney has a preponderance in women, with a gradually incidence in the later period of life. 2 These tumors usually have an insidious presentation, with symptoms an signs occurring at late stages of the disease: abdominal pain, palpable mass, vomiting, hematuria and weight loss. 3 Neither ultrasonography, tomography or magnetic resonance are able to differentiate between leiomyosarcomas an renal cell carcinomas. 4
Renal LMS usually have an aggressive biological behavior with poor prognosis. Radical nephrectomy is the treatment of choice. 5 The major prognostic factor is total surgical resection, 5 when it is completed, 5 years disease free survival could be of 60%. Although the role of lymphadenectomy in renal cancer remains controversial, given the extent of the tumor in the present case, this could have been done.6 Also surgical margins, major prognostic factor becomes histological grade, with 5 years disease-free survival of 90% for low grade tumors, and 30% for high grade tumor.5,7 No role for postoperative chemotherapy or radiotherapy has been determinate, although, adjuvant therapy is generally used to tumors with partial resection. 8 To date, in complete resection sarcoma, published studies show better local control of the disease but no survival benefit for adjuvant treatment with chemotherapy and radiotherapy.9–11 The possibility of treatment with KIT tyriosine kinase inhibitors such as sunitinib has been reported in phase II trial. 12
Conclusions
In this case report we show a rare primary LMS, which differential diagnosis is only possible for histopathological analysis, and the good prognosis seems to be related with complete surgical resection.