
Abstract
Objectives:
Leiomyosarcomas are relatively rare uterine smooth muscle tumors. Surgery is the most common therapy choice for uterine leiomyosarcomas. However, controversy exists over the appropriate initial surgical management, especially about the role of lymph node sampling. The aim of our study is to analyze the prognostic factors and the role of lymphadenectomy in overall survival and in disease-free survival.
Methods:
We analyzed retrospectively 31 patients suffering from uterine leiomyosarcomas at Institute of Salah Azaiez during 2000–2014. Demographic and clinical features such as age, menopausal status, stage, tumor size, and management options were examined, and pathological characteristics such as mitotic count, lymphovascular space invasion, and tumor necrosis were evaluated.
Results:
Out of 31 patients treated for uterine leiomyosarcomas, pelvic lymphadenectomy was done for 18 patients. No para-aortic lymphadenectomy was performed. Median number of resected lymph nodes was 13 ± 7 (range: 3–27). Lymphatic metastasis was observed in 2 out of 18 patients with clinical stage IA and IIIB. The distribution of different variables (age, International Federation of Gynecology and Obstetrics stage, tumor size, mitotic count, and adjuvant treatment) between the group of patients, who had or had not lymphadenectomy done, had no significant difference. The 5-year overall survival and disease-free survival were 61% and 50%, respectively. Clinical stage, presence of lymphovascular space invasion, and lymph nodal dissection were found to be relevant for disease-free survival on univariate analysis. Only age and menopausal status were found to be a prognostic factor for overall survival.
Conclusion:
Hence, routine lymph node dissection was not generally recommended. Our study demonstrates that lymphadenectomy has a statistically significant effect on disease-free survival but not on overall survival.
Introduction
Leiomyosarcomas (LMS) are relatively rare uterine smooth muscle tumors.1,2 Their occurrence was estimated in 0.64 per 100,000 women. 3 They are aggressive tumors with a poor prognosis.4,5 Often, diagnosis of LMS is made at the time of myomectomy or hysterectomy for presumed benign leiomyomas. 6 Surgery is the most common therapy choice in uterine LMS. 7
However, controversy exists over the appropriate initial surgical management, with few data to help guide decisions. Most would agree that at a minimum of a total abdominal hysterectomy should be performed. However, the role of lymph node sampling remains unclear. The incidence of lymph node metastasis in uterine LMS is reported to be 6%–26%. 4
The aim of our study is to analyze the prognostic factors and the role of lymphadenectomy in overall survival (OS) and disease-free survival (DFS).
Materials and methods
A retrospective analysis of 40 patients with uterine LMS treated at Institute of Salah Azaiez during 2000–2014 was performed. Only 31 patients were eligible for analysis. Nine patients had been excluded from the study because of insufficient records.
In a few cases, a presumptive diagnosis was possible using a combination of vaginal ultrasound and histology after hysteroscopy and curettage of the uterine cavity. Demographic, clinical, pathological, and treatment-related data were abstracted from the patients’ records. Pathological slides of patients were reviewed.
Demographic and clinical features such as age, menopausal status, stage, tumor size, and management options were examined. Pathological characteristics such as mitotic count, lymphovascular space invasion, and tumor necrosis were evaluated.
Staging was undertaken according to the 2009 International Federation of Gynecology and Obstetrics (FIGO) staging system. All patients underwent a median laparotomy. No patient had intra-abdominal fragmentation of the specimen. At least total abdominal hysterectomy with or without bilateral salpingo-oophorectomy was done. No patient had intra-abdominal fragmentation of the specimen.
The decision for lymphadenectomy was taken according to intraoperative findings (extrauterine spread, strong suspicion for malignancy, and enlarged lymph nodes) or frozen-section result, known pathology before surgery (endometrial sampling or after myomectomy), and discretion of the senior surgeon. If lymphadenectomy was performed, it included only pelvic areas; no para-aortic lymphadenectomy was done. The extent of anatomic landmarks of pelvic lymphadenectomy was defined by the aortic bifurcation as an upper limit and included the common, external, internal iliac artery, and the obturator fossa.
Adjuvant treatment modalities were classified as no adjuvant treatment, chemotherapy, radiotherapy, or chemotherapy followed by radiotherapy. A chemotherapy regimen was adriamycin plus ifosfamide. The period from surgery to recurrence or last visit was defined as DFS, and the period from surgery to death or last visit was defined as OS.
Patients age at diagnosis (⩽50 vs >50 years), maximal tumor diameter (⩽110 vs >110 cm), clinical stage (I vs II–IV), lymphovascular space invasion (yes or no), mitotic count per 10 high power field (HPF; 0–15 and >15 counts per 10 HPF), necrosis (yes or no), performance of lymphadenectomy (yes or no), and adjuvant postoperative treatments were the variables analyzed for a clinical significance with respect to both DFS and OS. These thresholds were chosen arbitrarily and with respect to the distribution of patients’ values.
The analysis was conducted with the SPSS, version 20 (IBM Corporation, Armonk, USA) statistical software program. The normality of quantitative variables was tested with the Kolmogorov–Smirnov test. Normally distributed quantitative variables were expressed as mean ± SD, while non-normally distributed variables were expressed as the median and range. Categorical variables were expressed by frequency counts and percentages. The student’s t-test and non-parametric tests (Mann–Whitney U test) were used to compare quantitative data. Chi-square test was used to compare qualitative data. Categorical variables were analyzed with Kaplan–Meier survival analysis using log-rank test to determine whether they had statistically significant effects on DFS and OS. Factors having a p value less than 0.05 in univariate analyses were considered statistically significant for the results.
Results
Means age of patients was 50 ± 11 years (range: 27–70). The most common presenting symptoms were abnormal vaginal bleeding in 21 cases, pelvic mass in 7 cases, recurrent abdominal pain in 5 cases, and in 2 cases, uterine mass was accidentally discovered. Only 11 patients had dilation and curettage before surgery, confirming uterine LMS. For the remaining patients, sarcoma was diagnosed by hysterectomy.
A total of 23 patients were admitted primarily to our institute. Eight patients were undergoing myomectomy for presumed benign fibroids in other centers and were found to have LMS on final pathology. They had referred to us postoperatively for completing staging procedure within 1 month. Finally, 23 of these patients had total abdominal hysterectomy and bilateral salpingo-oophorectomy, 6 had colpohysterectomy, and 2 patients had inter-adnexal hysterectomy.
Pelvic lymphadenectomy was done in 18 patients. No para-aortic lymphadenectomy was performed. Median number of resected lymph nodes was 13 (range: 3–27). Lymphatic metastasis was observed in 2 out of 18 patients with clinical stage IA and IIIB. The distribution of different variables (age, FIGO stage, tumor size, mitotic count, and adjuvant treatment) between the group of patients, who had or had not lymphadenectomy done, had no significant difference (Table 1).
Comparison of patients with lymphadenectomy versus without lymphadenectomy.

TAHBS: total abdominal hysterectomy and bilateral salpingo-oophorectomy; FIGO: International Federation of Gynecology and Obstetrics.
It should be noted that from 20 patients with stage I, 8 patients had first myomectomy in another center. Adjuvant treatment was used in 19 patients: 13 patients were treated with adjuvant radiotherapy, 4 patients were treated with adjuvant chemotherapy, and 2 were treated with chemotherapy followed by radiotherapy. Median follow-up for patients was 28 months (range: 1–207 months).
Disease recurrence was observed in 13 cases with a median follow-up of 14 months postoperatively: four recurrences were limited to the pelvic and were treated by a combination of chemotherapy and surgery, four patients had both distant metastases and pelvic recurrence, four patients had only distant metastasis, and one had progression disease.
At the final time of analysis, 10 patients died of the disease. The 5-year OS and DFS were 61% and 50%, respectively. Clinical stage, presence of lymphovascular space invasion, and lymph nodal dissection were found to be significant factors for DFS on univariate analysis (Figures 1 and 2). Patients aged ⩽50 had the best OS than older women (p = 0.03; Table 2).

Kaplan–Meier disease-free survival curve by stage.
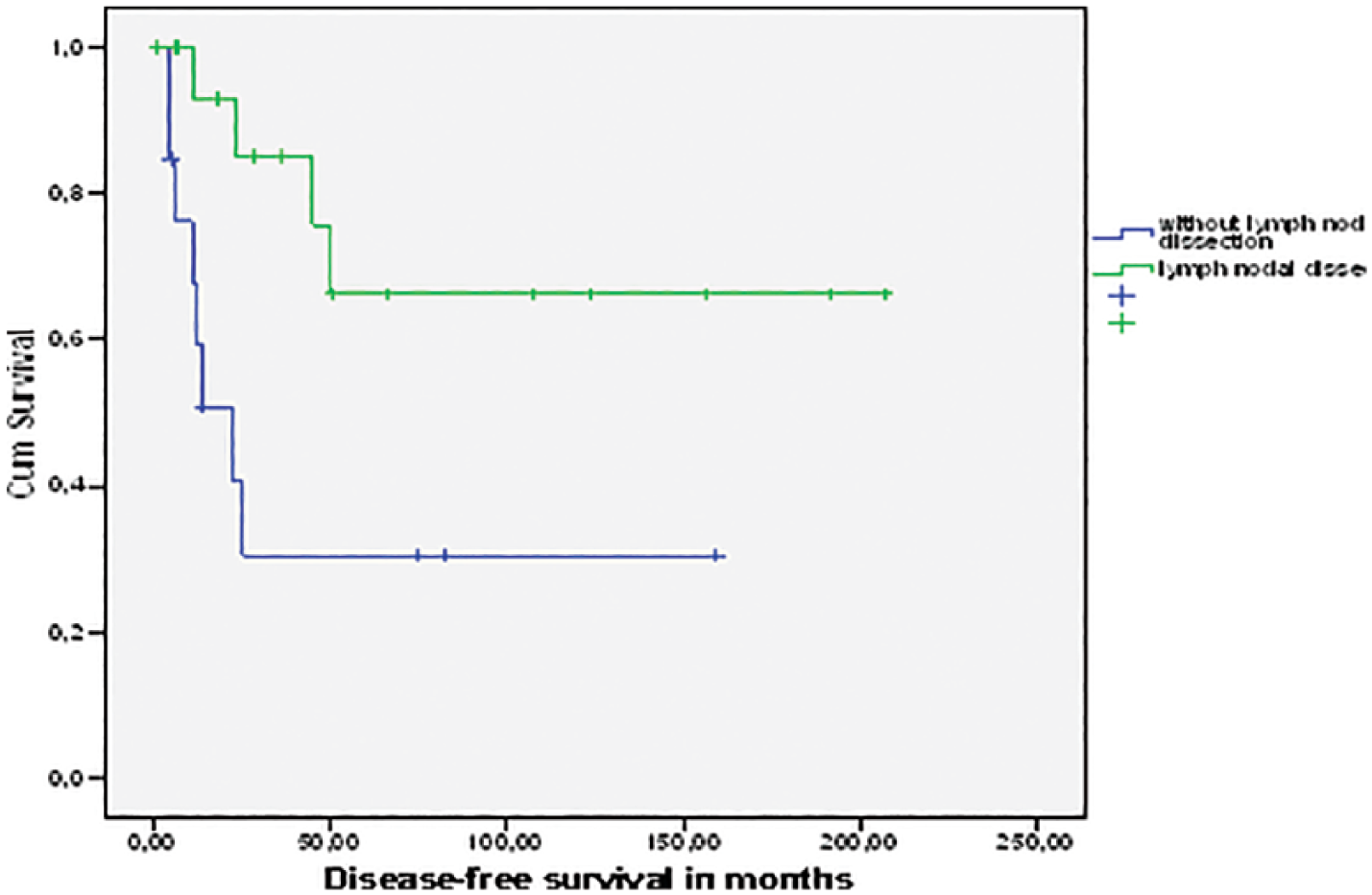
Kaplan–Meier disease-free survival curve by impact of lymphadenectomy dissection.
Clinicopathologic characteristics of patients and their associations with DFS and OS.

A subgroup analysis of patients with early stage could not reveal a significant difference among who had or not lymphadenectomy done both on DFS and the OS (p = 0.2 and 0.9, respectively).
Discussion
The gold standard in primary therapy of uterine LMS is surgery consisting of total abdominal hysterectomy with intact uterine removal for women with uterine-limited disease. 8 The National Comprehensive Cancer Network (NCCN) treatment guidelines on uterine sarcoma and soft tissue sarcoma recommend an intact “en bloc” surgical resection of the tumor with negative pathologic margins. 9
To date, the role of lymphadenectomy in the staging and prognosis of uterine LMS remains unclear. However, in carcinosarcoma, lymphadenectomy was recommended by gynecologic oncology group (GOG) study. 10 Similarly, for endometrial stromal sarcomas, lymph node dissection had a clinical value.11,12 Many authors were focused on evaluation of benefit and impact of lymphadenectomy of LMS; however, their results were controversial.
In our presented study, out of 31 patients operated from LMS, most of the patients had early stage (I; 64.51%). In the eight patients undergoing myomectomy for presumed benign fibroids in other centers, and who were found to have LMS on final pathology, a completion procedure with total hysterectomy and bilateral salpingo-oophorectomy (BSO) was done. In total, 18 patients had undergone a pelvic lymphadenectomy. What is pertinent in our study is that from two patients who had lymphatic metastasis, one had early stage.
Patients who had lymphadenectomy done had a better median DFS (148 vs 57 months; p = 0.017). However, lymphadenectomy was not a significant prognostic factor for OS (p = 0.7). Two others prognostic factors, stage and presence of lymphovascular space, were found to be significant factors for DFS on univariate analysis. Patients aged ⩽50 had the best OS than older women (p = 0.03). Our data had many points in common with several other publications.
Ayhan et al. 4 included 63 patients with uterine LMS and concluded that performing an extended lymphadenectomy had no effect on survival. More recently, the study of Kapp et al. included 1396 patients with uterine LMS, with 348 patients who underwent lymphadenectomy and 23 patients (6.6%) having lymph node metastases. All lymph node-positive was found in patients with advanced stage (III and IV). No impact of lymphadenectomy on 5-year disease-specific survival (DSS) was established. 13
Similarly, another retrospective review of 208 patients with LMS failed to show any effect of lymph node evaluation on DSS. 14 Furthermore, a retrospective meta-analysis 15 shows that lymphadenectomy had no statistically significant effect on OS, so it is not recommended in uterine LMS unless the patient has obvious extrauterine involvement, clinically suspicious enlarged nodes, or advanced sarcomas. 16
Two large series13,17 show that positive lymph node status was associated with decreased survival. However, another study holds different opinions; they indicated that lymphadenectomy could have a survival effect in uterine sarcomas. 18 Tsikouras et al. 2 reported a series of 60 patients with uterine sarcomas including LMS, and they conclude that lymphadenectomy in patients with early stage uterine sarcoma decreased the recurrence and improved survival. However, this study did not evaluate uterine LMS separately from other uterine sarcoma types (endometrial stromal sarcoma and malign mixed Mullerian tumor).
Several other prognostic factors that affect DFS were cited in the literature: age,7,13,19 premenopausal status,20,21 mitotic count,4,7 tumor grade,13,14 stage,7,13,14,19 and LVSI. 19 The most important were tumor stage and grade.13,22 The largest analysis of women with LMS included (n = 7455) from 1998 to 2013 shows that LMS tumor size is an important prognostic indicator. Even more, neither adjuvant treatments (radiation therapy or chemotherapy) demonstrated encouraging results in clinical prognosis in our study.
In the literature, the role of adjuvant therapy for the management of uterine LMS is controversial. Most of the studies did not demonstrate favorable prognostic of adjuvant treatments.23,24 For patients with advanced or recurrent uterine LMS, gemcitabine and docetaxel were interesting strategies. 8 However, the role of chemotherapy in the management of uterine-confined disease was not clear, although the NCCN uterine sarcoma guidelines suggest that either adjuvant chemotherapy (doxorubicin) versus observation may be considered in women with early stage uterine sarcoma after hysterectomy surgery. 25
It is clear that radiotherapy does not improve survival outcomes. However, some authors demonstrate that adjuvant radiotherapy decreases the rate of recurrence but does not affect OS.26,27 In our study, adjuvant treatment was given to 61% of patients. However, it did not improve survival and did not decrease recurrence. Targeted therapies continue to be explored in clinical trials for patients with metastatic uterin LMS with progression of disease. 28
In the PALETTE, a phase III trial by the European Organisation for Research and Treatment of Cancer (EORTC) that randomized 165 patients to pazopanib versus placebo with metastatic uterine LMS after failure of standard chemotherapy was conducted. This trial shows that pazopanib increased significantly median progression-free survival to 4.6 months compared to 1.6 months for placebo, although OS was not significantly different. 29
Conclusion
Hence, routine lymph node dissection is not generally recommended. Our study demonstrated that lymphadenectomy has a statistically significant effect on DFS but not on OS. Even though there are some limitations in our study, such as the small number of our population, retrospective analyses, and the lack of information on estrogen/progesterone (ER/PR) receptors and grading, our study includes only LMS uterine, contrary to other studies that often included a heterogeneous group of all sarcoma subtypes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the medical and ethic committee of the Salah Azaiez Institute.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was not sought for the present study, because we have just utilized data from documents. Patients’ anonymity has been preserved.