
Abstract
We report a 41-year old male who presented to the Emergency Department after falling while water-skiing. He had a previous medical history included chronic headaches, which had persisted for the last 2-3 months prior to presentation. Computed tomography of the head showed a small hypersensitivity with a small extra axial collection with a maximum thickness of 1mm. Differential diagnoses included an arachnoid cyst, haemangioma, meningioma or a secondary lesion. A diagnosis of Langerhans Cell Histiocytosis was made based on the histopathology examination and the immunoperoxidase staining.
Introduction
Langerhans cell histiocytosis (LCH) is a rare condition that usually affects the pediatric population. The condition can affect almost any organ in the body. It is a rare condition with an estimated annual incidence between 1-7 cases per million of the population. 1 More than 50% of patients are less than two-years of age have disseminated LCH with organ dysfunction and die of the disease. 2 The prevalence of LCH seems to be higher among whites than other races. The incidence of LCH is greater in males than in females, with a male-to-female ratio of 2:1. Recent early data from the U.K. suggest that just as many cases of LCH present in adult life as in childhood. 1 However, it should be noted that at present it remains unclear if these adult cases are de novo or if they are occult cases from childhood. 3 We report a case of adult LCH with his presentation, medical history, clinical characteristics, and radiological findings as well as the success of the surgical intervention.
Literature Search
The search strategy involved the major electronic databases MEDLINE, EMBASE, PubMed and Current Contents (1950-2013) to find all available articles on Langerhans cell histiocytosis affecting the skull specifically in adults. Additional manual searches were made using the reference lists from the selected articles to retrieve other papers relevant to the topic. No language restriction was placed on any of the literature searches. The keywords used, alone and in combination, were Langerhans cell histiocytosis, histiocytosis X, eosinophilic granuloma, Letterer-Siwe disease, Hand–Schuller-Christian syndrome, Histomoto-Prizker syndrome, self-healing histiocytosis, Langerhans cell granulomatosis, Type II histiocytosis and non-lipid reticuloendotheliosis. Articles with cases involving both adults and children were excluded. In addition, foreign language papers identified in the search that were not translatable to English were excluded.
Case Report
A 41-year old male who presented to the Emergency Department after falling while water-skiing at 40-50 km/hr. He landed face first onto the water but did not lose consciousness and remembered that he was in trouble.
The patient recalls his face feeling puffy for 10-15 min but then settled and both his eyes were bleeding for approximately 30 min. He complained of neck and right shoulder pain and a frontal headache. His previous medical history included surgery for lumbar disc prolapse and chronic headaches, which had persisted for the last 2-3 months prior to presentation. Medications included Dothiepin (TCA) and Salazopyrin (Sulfasalazine). On assessment, the patient was conscious (GCS 15), had a BP of 123/92, pulse of 72, and an oxygen saturation of 95%. There was periorbital bruising and swelling with a laceration of the right inner aspect of the upper eye-lid which was bleeding and blood was present in both eyes. A full opthalmology assessment found no abnormalities. Radiological assessment included X-rays of the head (Figure 1), pelvis, C-spine, right shoulder, lumber spine, and a CT of the head. The radiographs showed no evidence of acute fractures/dislocations. The head CT showed a small hypersensitivity with a small extra axial collection with a maximum thickness of 1mm. Differential diagnoses included an arachnoid cyst, haemangioma, meningioma or a secondary lesion. Due to the possibility of a malignant lesion a bone scan was also undertaken and subsequently showed an active lesion. The patient was admitted and had a craniotomy to excise the skull tumor. The excised lesion consisted on bone with soft tissue (30×20×7 mm). Histopathological examination of the specimen, which included immunoperoxidase studies revealed a rounded defect of the bone which consisted of a proliferation of fibrous stroma within which can be seen inflammatory foci (Figure 2).

X-ray showing lesion on skull.

Histopathology of lesion removed from skull.
Immunoperoxidase studies were positive for S100 and CD68 and negative for HMB45 and Cam 5.2. The patient is currently well.
Discussion and Conclusions
Langerhans cell histiocytosis is a clonal proliferative disorder of the antigen presenting Langerhans’ cell and refers collectively to a group of diseases previously known as histiocytosis X, eosinophilic granuloma, Letterer-Siwe disease, Hand-Schuller-Christian syndrome, Hashimoto-Prizker syndrome, self-healing histiocytosis, pure cutaneous histiocytosis, Langerhans cell granulomatosis, Type II histiocytosis and non-lipid reticuloendotheliosis.4,5 Langerhans cell histiocytosis usually affects patients under 10 years of age, however, studies have reported that the average age for presentation is 25 years. 5 Patients mainly present with localized bone pain, dysponea and malaise, and 75% have non-disseminated disease. The skull, femur, pelvis and ribs are most commonly involved. 5 With skull lesions, the orbit and the cranial base are frequently involved and produce the classic triad of bony defects, exophthalmos and diabetes insipidus. 5
Our adult case exemplifies an uncommon presentation of LCH which more commonly occurs in pediatric populations. However, this case illustrates a classic presentation of LCH in adults. Osteolytic bone lesions are a common manifestation of single system LCH in adults. These lesions tend to be unifocal rather than multifocal, often involving the skull or axial skeleton, 4 such as in our patient. Our review of skull vault lesions in adults (Table 1) has confirmed this observation with 4 out of 6 cases of LCH involving the skull having unifocal lesions.6–11 Calvarial lesions are normally found incidentally as was the case with our patient. However they may also present with bone pain, soft-tissue swelling, hearing loss, vertigo and visual disturbances.6–11 Histologically, proliferation of Langerhans cells expressing CD1a and S100 admixed with acute and chronic inflammatory cells are consistently reported.6–11 Immunohistochemical findings in our patient were consistent with these features. This report is interesting and adds valuable information to limited literature available on unifocal skull vault lesions in adults with LCH. Local treatment with excision, systemic chemotherapy and corticosteroid injection is highly successful in treating this disease and patients have excellent prognosis. 5 Over 90% of patients survive 3 to 5 years post diagnosis.5,12,13 Age at diagnosis and initial response to therapy affect the prognosis and rate of recurrence of disease. 5
Case reports of Langerhans cell histiocytosis with skull lesions in adults.
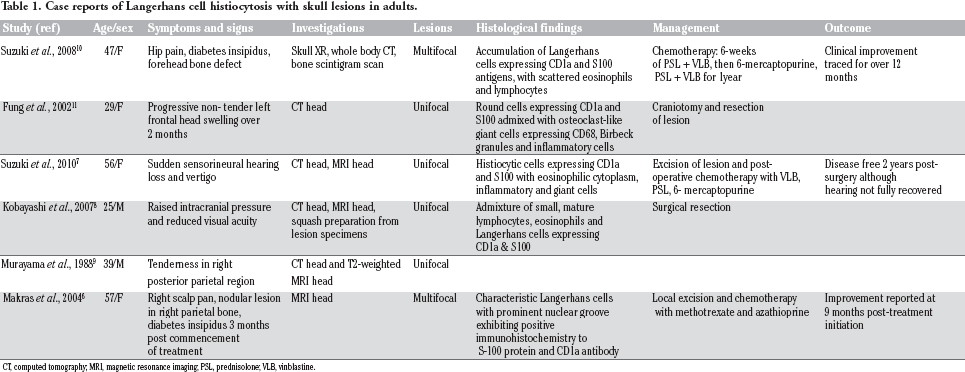
CT, computed tomography; MRI, magnetic resonance imaging; PSL, prednisolone; VLB, vinblastine.
Footnotes
Acknowledgements
We would like to thank Mr Peter Paton of the Anatomical Pathology Department and Mr Chris Henwood of the Audiovisual Department, Nepean Hospital for their assistance with the X-ray.