
Abstract
Kaposi's sarcoma (KS) most often affect the skin but occasionally affect the mucosa of different anatomic sites. The management of mucosal KS is seldom described in the literature. Data from 15 eligible patients with mucosal KS treated between 1994 and 2008 in five institutions within three countries of the Rare Cancer Network group were collected. The inclusion criteria were as follows: age >16 years, confirmed pathological diagnosis, mucosal stages I and II, and a minimum of 6 months’ follow-up after treatment. Head and neck sites were the most common (66%). Eleven cases were HIV-positive. CD4 counts correlated with disease stage. Twelve patients had biopsy only while three patients underwent local resection. Radiotherapy (RT) was delivered whatever their CD4 status was. Median total radiation dose was 16.2 Gy (0–45) delivered in median 17 days (0–40) with four patients receiving no RT. Six patients underwent chemotherapy and received from 1 to 11 cycles of various regimens namely vinblastin, caelyx, bleomycine, or interferon, whatever their CD4 counts was. Five-year disease free survival were 81.6% and 75.0% in patients undergoing RT or not, respectively. Median survival was 66.9 months. Radiation-induced toxicity was at worse grade 1–2 and was manageable whatever patients’ HIV status. This small series of mucosal KSs revealed that relatively low-dose RT is overall safe and efficient in HIV-positive and negative patients. Since there are distant relapses either in multicentric cutaneous or visceral forms in head and neck cases, the role of systemic treatments may be worth investigations in addition to RT of localized disease. Surgery may be used for symptomatic lesions, with caution given the risk of bleeding.
Introduction
Kaposi sarcoma (KS) was first described in 1872 by Moritz Kaposi, a Hungarian dermatologist as brownish red-to-bluish red cutaneous or mucosal neoplasms of the larynx, trachea, stomach, liver, and colon. Until the HIV epidemics in the 1980's, KS was viewed as an indolent slowly growing cancer and patients were expected to die with, rather than of KS. KS was later seen in 30–40% of patients with AIDS but fell markedly starting in the 1995's with more efficient anti-retroviral therapies. A breakthrough came in 1994, when the Kaposi sarcoma-associated herpes virus [human herpesvirus type 8 (HHV-8)] was identified and linked with all four types of KS, namely classic (traditional), endemic (African), epidemic (AIDS related), and iatrogenic (related to immunosuppression). Since then, much research has shown that HHV-8 appears to be necessary to, but not sufficient for, the development of KS. The HHV8 is ubiquitous among human populations. It is generally shed in the oral cavity, and is primarily transmitted via the salivary route. 1 However, the seroprevalence within the general population is low, suggesting that HHV8 is not ubiquitous among healthy human populations. The question also remains whether KS is multicentric or metastatic and whether mucosal and cutaneous forms are different entities.1,2 The current mainstay of cutaneous Kaposi's sarcoma therapy includes systemic and localized treatments.3,4 The knowledge base directing treatment for mucosal KS, however, is much less and understood. We aimed at assessing the management practices, including the role of radiation therapy, in patients with localized mucosal KS.
Materials and Methods
Patients
We collected the data from 15 eligible patients with mucosal KS treated between 1994 and 2008 in five institutions within three countries of the Rare Cancer Network group (RCN). The RCN is a cooperative, international consortium of investigators studying tumors too rare to be the focus of prospective trials. 5 The inclusion criteria were as follows: age >16 years, confirmed pathological diagnosis, stages I and II, and a minimum of 6 months’ follow-up after treatment. All medical records were reviewed for age, gender, symptoms, physical examination, laboratory examination, imaging, pathological diagnosis, involved sites, stage, treatment modality, response, time and site of relapse, treatment-related complications, time to death, and date of last follow-up. In this study, all investigators obtained their own Institutional Review Board approval for patients’ data collection. All original pathology reports were reviewed using the World Health Organization (WHO) classification of KS. The workup of all individual patients included medical history, physical examination, complete blood count, lactate dehydrogenase and complete metabolic profile. Computed tomography, magnetic resonance imaging, positron-emission tomography, or whole body computed tomography scan were performed according to each institutions’ policy. Patients were treated according to each hospital's local policy. The modality of treatment included chemotherapy, radiotherapy (RT), surgical resection, or a combination of these. Early and late treatment toxicities were evaluated according to the Common Terminology Criteria for Adverse Events V3.0.
Statistical methods
Overall survival was calculated from the date of diagnosis to the date of last follow-up or death from any cause. Disease free survival (DFS) was calculated from the date of diagnosis to the date of relapse from KS. Local control was calculated from the date of diagnosis to the date of local recurrence. Survival curves were constructed using the Kaplan-Meier method and differences were considered significant if the P value was <0.05 (two-tailed log rank test).
Results
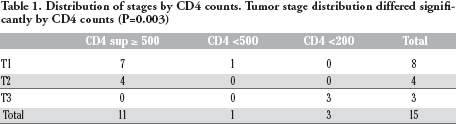
Localized mucosal presentations of KS were found to be rare compared to cutaneous forms of KS, accounting for only 5% of all cases reviewed at the Mayo Clinic for this study. Patient data were collected from five institutions in France, Switzerland and the USA from the Rare Cancer Network. Median age at diagnosis was 40.6 years old (28–81). There were 12 males and 3 females. Patients originated from Eastern Europe, Mediterranean, Africa, Asia, other including Caucasian in 2, 5, 3, 1 and 4 cases, respectively. Eight, six and one were heterosexual, homosexual and bisexual, respectively. KS were diagnosed between 1994 and 2007, three being diagnosed after 2000. There were 11 HIV positive Kaposi sarcoma cases. Median tumor diameter was 3 cm (2–6). T stage was significantly more advanced in HIV patients with CD4 counts lower than 200. The three T3 patients had all less than 200 CD4/mm3 (Table 1). Three patients had node-positive disease, including one bulky nodal disease in a patient with a CD4 count of less than 200.
Distribution of stages by CD4 counts. Tumor stage distribution differed significantly by CD4 counts (P=0.003)
A majority of tumors (66%) occurred in the head and neck region, including 4, 2, 1 and 1 in the oropharynx, oral cavity (Figure 1), larynx and sinus, respectively. Two cases occurred in the male genitalia and one case of each in the stomach, anal canal and vagina. An association with cutaneous involvement was noted in two cases at diagnosis, namely two patients with respectively less than 200 CD4 and oral cavity disease or stomach and normal CD4 counts (Table 2).
Isolated Kaposi sarcoma lesion of the left tonsil in a 69 year-old Caucasian HIV-negative human herpesvirus type 8 positive male.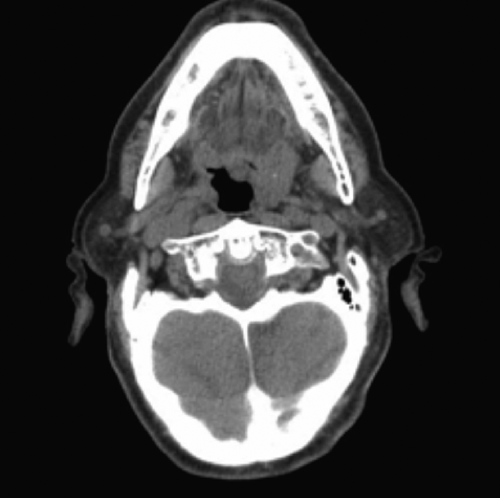
Patient, tumor characteristics and outcomes.

G, grade; skin +, cutaneous involvement; fu, follow-up; awod, alive without disease; awd, alive with disease.
Twelve patients had no surgery. All three operated patients had normal CD4 counts, only one patient had complete resection. RT was delivered whatever their CD4 status was. Median total radiation dose was 16.2 Gy (0–45) delivered in median 17 days (0–40) with four patients receiving no RT.
Six patients underwent chemotherapy and received from 1 to 11 cycles of various regimens namely vinblastin, caelyx, bleomycine, or interferon, whatever their CD4 counts was.
Acute mucosal G1–2 toxicity was present in all cases whatever CD4 counts. Grade 1–2 dysphagia was present in three cases including two cases with low CD4 counts (P=0.037). Grade 1–2 dermatitis was present in two patients with normal CD4 counts. There were no grade >3 toxicities. Toxicity and severity was not different between HIV patients and patients with different CD4 counts. There was one case with other type of toxicity in the low CD4 count.
Median follow-up was 67 months (6–119). Two local relapses were noted in one patient with normal CD4 counts and one with low CD4 counts. These relapses did not occur in the RT field: one patient had a T3 disease of the oral cavity and received only intralesional vinblastin, while the other one had undergone upfront surgery for T1 oropharyngeal, was reoperated for early relapse (6 months), again relapsed and was successfully salvaged with RT. The latter failed in the skin of the foot four years following irradiation. There were no regional relapses included in the patient treated with RT for bulky nodal disease and laryngeal KS. There were three distant failures: one in the lung and skin and two in the skin. All patients are alive at last follow-up including four without disease. Two- and five-year DFS were 81.6% and 75.0% in patients undergoing RT or not, respectively. Median survival was 66.9 months (23–119)(Figure 2).
Disease free survival.
Discussion
The disease was more common in men. The median age (41 years old) was younger than those for HIV-negative patients with cutaneous disease. The number of HIV-positive patients may explain this difference. Noteworthy, all HIV-positive patients were under antiretroviral therapy, which in itself is recognized an efficient therapeutics for KS. For HIV-positive patients with limited or advanced KS, treatments should include highly active antiretroviral therapy (HAART) whenever possible. AIDS-related KS may clinically regress with the use of HAART alone as CD4 count improves. A recent South Africa-based randomized trial with 59 patients showed that HAART with chemotherapy produced a higher rate of treatment response, while the HAART alone arm was not inferior in overall survival. 6 The prognosis of AIDS-related conditions including KS has dramatically improved after HAART was introduced for clinical use. If immune reconstitution inflammatory syndrome occurs, such as rapid progression of KS within weeks of starting HAART, chemotherapy will become necessary. For a pediatric population with HIV-1-infected KS, an intense combination of anti-retroviral and chemotherapeutic agents was proven effective. 7 Survival was overall good in the series whatever the treatment modalities, which were highly heterogeneous.
In the literature, management modalities for cutaneous KS include surgery, conventional and megavoltage RT, chemotherapy, immunotherapy, antiviral drugs, and cessation of immunosuppressive therapy in iatrogenically immunosuppressed patients.
8
For systemic therapies, options exist for chemotherapy, immunotherapy, HAART for AIDS-related epidemic KS, and experimental biologic agents. Localized methods include intralesional chemotherapy, laser therapy, external beam radiotherapy and surgical excision. For chemotherapeutic agents, recent studies have established a strong role for pegylated liposomal doxorubicin, which is now generally accepted as first-line therapy.
9
Other agents such as taxane, bleomycin, vinblastine, vincristine, and etoposide have also been tested with certain success but are now considered to be older regimens.
10
For classical KS, immuno-modulators such as interferon alfa,
11
topical imiquimod and thalidomide were efficacious in small studies.4,12,13 Localized cutaneous nodular disease can be treated by surgery, RT, intralesional and outpatient low-dose vinblastine chemotherapy (Figure 3).
14
For local treatments, radiotherapy often produces excellent therapeutic and cosmetic outcome,15,16 while palliative in nature if KS becomes disseminated. These studies showed that radiation therapy was an effective form of treatment for most KS (response rate 60–90%), with a minimal toxicity profile. A variation of low to intermediate-dose radiotherapy fractionation schemes have been reported, ranging from single-fraction 6 Gy to 39 Gy in 13 fractions.17–21 The outcomes and survival after radiotherapy appeared similar for both classic and HIV-related KS in an Ugandan population.
22
The use of radiotherapy did not appear harmful in patients who were known to be immunocompromised. RT has been widely used in doses ranging between 6 and 30 Gy for localized mucosal disease in AIDS patients but may not be sufficient for HIV-negative patients for Jindal
Treatment algorithm for localized cutaneous and mucosal Kaposi sarcoma lesions. If lesion growth is slow or stable, observation is a reasonable option. For HIV-infected patients, initiation of HAART alone may induce regression of the lesions. Systemic chemotherapy should be discussed depending on the number of lesions (>20), involvement of internal organs, associated symptoms, speed of evolution, age, performance status, ulceration and/or presence of edema. Close monitoring during radiation treatments is important for immunosuppressed patients. Absence of immunodeficiency can include HHV-8 patients. *Strict oral hygiene protocol and antifungal treatment for 6 weeks (starting 1 week before the radiotherapy). LF-EBRT, localized field external beam radiotherapy; CT, chemotherapy.
Head and neck subsites were the most frequent anatomic site involved, which can be explained by HHV8 oral shedding.1,30–37 The hard palate and gingiva are the most frequent locations. Additional sites include the tongue, buccal mucosa, lips, submandibular duct area, parotid gland, and intra-parotid lymph nodes. A recent review identified over 200 non-AIDS KS cases, with the palate and oropharynx being the commonest sites, which is consistent with our series. 1 Oral classic KS lesions, single or multiple, are usually painless, well-demarcated, and brownish to red with violaceous macules/papules that eventually develop as nodules with or without ulceration. HIV-negative oral KSs only represent 5% of African endemic KS series while oral cases represent over 50% of AIDS related KS.35,38 Surgery may be performed but the disease may not always be well demarcated. For symptomatic lesions which cause bleeding and ulcerative dermatitis, surgical excision may be considered. Limited excision alone can be curative in selected immunocompetent individuals. 30 Laser therapies may improve the pigmentary impact of KS plaques and nodules on skin. 39 Intralesional chemotherapy (vinblastine, bleomycin) or topic alitretinoin (9-cis-retinoic acid) gel can also be used, which were American FDA-approved. For experimental biological agents, an mTOR (mammalian target of rapamycin) inhibitor caused KS regression and sustained response in a HIV-negative patient. 40 Therapies such as intratumoral elec-trochemotherapy, 41 antiangiogenic and anti-HHV-8 agents are currently under investigation.
One patient had interferon for stomach KS. For these anatomic sites, RT may not be appropriate owing to large set-up uncertainties and systemic treatment should be preferred. Two patients had involvement of their male genitalia and underwent successful low dose RT (15.2 and 19.8 respectively) and are alive without disease at 47 and 78 months. One patient had vaginal involvement, was treated with irradiation (16.2 Gy) and is disease free after 37 months follow-up. As also recommended by Kirova
Conclusions
This small series of mucosal KSs revealed that relatively low-dose RT is overall safe and efficient in HIV-positive and negative patients. Since there are distant relapses either in multicentric cutaneous or visceral forms in head and neck cases, the role of systemic treatments may be worth investigations in addition to RT of localized disease. RT has its own place in the management of mucosa KS as an efficient treatment. Surgery may be used with caution, given the risk of bleeding, for symptomatic lesions.