
Abstract
Clear cell variants of transitional cell carcinomas (TCC) of the bladder are extremely rare tumors. Only 6 cases have been reported until now. We report of a 67 year old man who presented with fast growing tumor disease. While initial diagnosis showed localized bladder tumor, final histopathology revealed pT4, G3, L1 urothelial carcinoma with clear cell differentiation. No more than 14 weeks after initial diagnosis the patient died from multi-organ failure after unsuccessful salvage laparotomy which showed massive tumor burden within the pelvis and peritoneal carcinosis. This case demonstrated an extremely fast tumor growth. Therefore, patients with clear cell urothelial carcinoma should be treated vigorously and without time delay. We present a case of clear cell variant of TCC which exhibited an extremely aggressive behavior. To our knowledge this is the fifth report of this rare disease.
Introduction
Approximately 15% of carcinomas of the bladder account for variants other than the most common urothelial carcinoma. The four major categories are squamous cell carcinoma, adenocarcinoma, undifferentiated carcinoma and variants of urothelial carcinoma. 1 Within the latter category, squamous, trophoblastic, glandular, micropapillary, nested and small cell differentiation are well described. However, little is known about urothelial carcinoma of the bladder with clear cell differentiation.
Case Report
A 65-year-old white male presented with progressive lower urinary tract symptoms and worsening of general condition. His past medical history was unremarkable. Laboratory investigation revealed elevated serum creatinine levels (139 µmol/L). Ultrasonography showed III pyelocaliectasia on both kidneys, thickening of the urinary bladder wall as well as residual urine of appr. 500 mL. Blood prostate specific antigen (PSA) level: 2.5 µg/L. After insertion of an indwelling urinary catheter creatinine levels did not decrease and the pyelocaliectasia remained. The patient underwent cystoscopy. Distal ureteral stenoses on both sides were recognized and ureteral stents were inserted. Non-papillary, solid tumor masses were found on the vesical trigonum and were removed by transurethral resection (TURBt). The pathohistological examination revealed poorly differentiated urothelial carcinoma of the clear cell variant with detrusor muscle infiltration (pT2a, G3). Computed tomography (CT) scan demonstrated 14 mm bladder wall thickening, no tumor invasion in perivesical tissue and no evidence of metastasis (Figure 1). Shortly after diagnosis, the patient was scheduled for radical cystectomy and ileal conduit. Final pathohistological examination confirmed the diagnosis of urothelial carcinoma clear cell variant, infiltrating the perivesical tissue, prostate and seminal vesicles (pT4, L1, G3, R1). Microscopic examination of the specimen exhibited diffuse glycogen-rich, clear cytoplasm and severe nuclear atypia in an alveolar growth pattern (Figure 2). Glandular differentiation was not observed. Immunohistochemical staining showed positivity for cytokeratin 7 (CK 7), cytokeratin 20 (CK 20) and cytokeratin 8/18 (CK 8/18) (Figure 2). Negative immunochistochemical staining results were observed for PSA, vimentin, HMB-45, S-100, cancer antigen 125 (CA 125), Melan-A and CD-10.
Computed tomography demonstrating bladder wall thickening (red arrow) but no evidence of perivesical tissue involvement and no evidence of metastasis.
Immunohistochemical staining reaction. Positivity for CK7, CK20 and CK8/18. Haematoxylin and Eosin (H&E) showing diffuse glycogen-rich, clear cytoplasm and severe nuclear atypia in an alveolar growth pattern.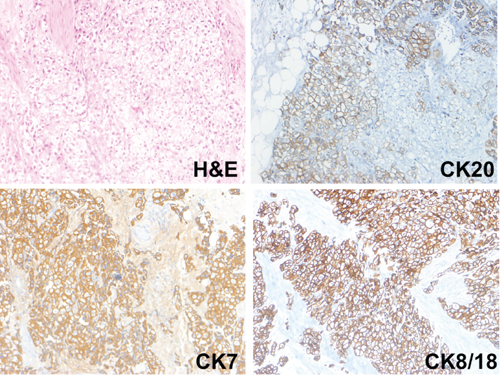
Approximately 9 weeks after cystectomy the patient presented with acute worsening of general condition and symptoms of ileus. Diagnostic CT scan demonstrated mechanical ileus due to local recurrence and indicated bowel infiltration (Figure 3). The patient was then scheduled for open laparotomy which revealed massive tumor burden within the pelvis infiltrating the small intestine and colon as well as a widespread peritoneal carcinosis making a complete resection impossible. Shortly after, the patient died from multi-organ failure.
Computed tomography (CT) diagnostic demonstrating signs of ileus. Open surgery revealed tumor infiltration causing a mechanical ileus. The latter was not identified by CT-scan.
Discussion
The World Health Organization (WHO) distinguishes several morphological subtypes of tumors of the urinary tract: urothelial carcinomas, squamous neoplasms, glandular neoplasms, neuroendocrine tumors, melanocytic tumors, mesenchymal tumors, haematopoietic and lymphoid tumors as well as miscellaneous tumors (WHO: histological classification of tumours of the urinary tract 2004, data not shown). Clear cell variant of urothelial cancer is a very rare subtype of glandular neoplasms to which also adenocarcinoma must be mentioned. A limited number of cases have been reported up to date;2–5 this is the fifth report of this rare variant of transitional cell carcinomas (Table 1). The problematic feature of clear cell variant urothelial carcinoma can be approached from two directions: histopathologically and clinically. Clear cell carcinoma can arise in almost any site including prostate, kidneys, uterus, ovary, vagina, lung and breast.6–9 Therefore it might be difficult to diagnose the primary site. Based on the urinary tract, clear cell features within the bladder have been mostly associated with adenocarcinomas that have been reported to be more frequent than clear cell variant urothelial carcinomas. The histopathology in our patient revealed multiple layers and severe nuclear atypia in an alveolar growth pattern (Table 2, Figure 2). Typical pattern of adenocarcinomas of the bladder such as glandular differentiation, tubulocystic or papillary morphological patterns as well as hobnail cells were not observed. Although not being a clear feature for differentiation immunohistochemical positivity for CK7 might suggest an urothelial origin making adenocarcinoma less likely.1,10 To rule out metastasis, although CT-scans did not indicate primary sites other than the bladder, we performed immunohistochemical stains for PSA (prostate cancer), vimentin (kidney cancer), CA 15-3 (colorectal cancer), HMB-45/S-100/Melan-A (melanoma) and CD-10 (clear cell renal carcinoma).
Reports of clear cell variant transitional carcinoma. Seven cases, including ours, have been published until now.

RC, radical cystectomy; TURBt, transurethral resection; LUTS, lower urinary tract symptoms.
Microscopic evaluation of each case. Common findings are glycogen-rich cytoplasm and nuclear atypia. In contrast to adenocarcinomas of the bladder glandular differentiation and hobnail cells are not found.

TCC, transitional cell carcinoma.
The clinical course of clear cell variant urothelial carcinomas of the bladder is currently unknown due to the lack of larger case series. Only five cases with clinical information have been published (Table 1).2–5 Our patient showed aggressive behavior with rapid local recurrence and development of peritoneal carcinosis to which he succumbed only 14 weeks after initial diagnosis at which an advanced tumor stage had been not assumed. A similar clinical course has been described by Kotliar and colleagues. 4 They reported of a 71-year old male who underwent radical cystoprostatectomy with ileal conduit due to muscle-invasive urothelial carcinoma clear-cell variant. Although computed tomography revealed no evidence of pelvic lymphadenopathy, nor metastatic disease, two pelvic lymph nodes were diagnosed carcinoma-positive. In spite of adjuvant chemotherapy the patient died after 20 months. In contrast a less aggressive course has been reported in two patients with urothelial clear cell carcinoma who were treated with TURBt, even though one patient had detrusor muscle invasion.3,5 Both patients were free from recurrence after 7 and 20 months (Table 1).
In conclusion, clear-cell variant urothelial carcinoma is a rare pathologic finding with a variable clinical course. Adenocarcinoma of the bladder, the major differential diagnosis, can be discriminated by conventional histology and immunohistochemistry. Clear-cell variant urothelial carcinoma shows a glycogen-rich cytoplasm and may be either circumscribed or extensive whereas adenocarcinoma is characterized by glandular differentiation and hobnail cells. Up to date immunohistochemical staining does not help to differentiate both variants (Table 3). Therefore, the pathologist is urged to make a decision based on microscopic findings. Future attempts should strive for strict diagnostic criteria as a prerequisite to define the underlying biology/genetic defects. Lager series are needed to classify prognostic groups and to choose the best therapeutic options for this rare tumor entity.
Immunohistochemical evaluation of each case. Distinct staining features of clear-cell variant transitional cell carcinomas have yet not been identified. A distinction to prostate cancer and renal cell cancer can be made.
