
Abstract
The nested variant of urothelial carcinoma (NVUC) is characterized by the presence of benign-appearing urothelial carcinoma cells in the lamina propria, sparing the surface urothelial involvement. NVUC shows aggressive clinical course despite of benign-looking histology. Herein reported are two cases of NVUC. One is 80-year-old woman, and another is 78-year-old man. In both cases, atypical cells forming nests and tubules were seen in the lamina propria without surface urothelial involvement. One case resembled nephrogenic metaplasia and another proliferated Brunn's nest or inverted papilloma. Immunohistochemically, both cases showed positive p53 and high Ki67 labeling, suggesting that both cases are malignant. Immunohistochemically, one case was characterized by positive cytokeratins, EMA, p53, Ki-67 (labeling=15%), α-methylacyl CoA racemase, CA19-9, and MUC1, and another case by positive cytokeratins, EMA, p63, p53, Ki-67 (lebeling=30%), CD10, CEA, and MUC1. Cyto keratin immunoprofiles were described and other antigens’ expressions were shown. The patients are now free of tumor 6 and 15 months after the resection of the bladder tumor.
Introduction
The nested variant of urothelial carcinoma (NVUC) of the urinary bladder is histologically characterized by bland, benign-looking urothelial carcinoma in lamina propria with nested and tubular patterns and without overlying urothelial carcinoma of the surface urothelial layer.1,2 The atypia of NVUC is relatively mild.1,2 NVUC resembles hyperplastic von-Brunn's nests, nephrogenic metaplasia, and inverted papilloma. High grade neoplasms with focal nests and tumors with overlying of carcinoma in situ should not be included in this variant. 2 NVUC should be differentiated from von-Brunn's nest, nephrogenic metaplasia, prostatic carcinoma, and inverted papilloma.1,2 Clinically, NVUC shows relatively aggressive course.
NVUC of the urinary bladder is very rare, and only less than 50 cases have been reported. 1 A PubMed search revealed only 8 reports of NVUC.3–10 Herein reported are two cases of NVUC with immunohistochemical findings.
Case Reports
Case #1
An 80-year-old woman consulted to our hospital because of dysuria. A blood laboratory test showed mild hyperlipidemia. Tumors markers were within normal ranges. Bladder endoscopy revealed a nodular tumor and transurethoral resection of bladder tumor (TUR-BT) was performed. Histologically, atypical cells were present in the lamina propria (Figure 1A and 1B). No tumor was seen in the surface urothelium (Figure 1A). The atypical cells formed small nests, and acinar formations were seen in a small number (Figure 1B). The cells had hyperchromatic nuclei and enlarged nuclei (Figure 1B). The histological features resembled nephrogenic metaplasia. Mucin stains were negative. An immunohistochemical study was performed with the use of Dako's envision method (Dako. Corp, Glustrup, Denmark), as previously described.10,11 The immunohistochemical results are shown in Table 1. Characteristic findings were positive cytokeratins, EMA, p53 (Figure 1C), Ki-67 (labeling=15%) (Figure 1D), α-methylacyl CoA racemase (AMACR), CA19-9, and MUC1 (Figure 1E) (Table 1). Since p53 was positive and Ki-67 was relatively high, benign conditions such as nephrogenic metaplasia and proliferated von Brunn's nest were denied. The final pathological diagnosis was NVUC of the urinary bladder. The patient is now free of tumor 6 months after TUR-BT, but is strictly followed up.
Case #1. A) Low power view of nested variant of urothelial carcinoma of the bladder. The atypical cells are present in the lamina propria. The surface epithelial cells are free of tumor. HE, x50. B) High power view of A. The atypical cells show mild atypia, and take a form of vague nested and tubular patterns. The features resemble nephrogenic metaplasia. HE, x 200. C) The atypical cells are positive for p53. Immunostaining, x200. D) The atypical cells show Ki-67 antigen. The Ki67-labeling is 15%. Immunostaining, x200. E) The atypical cells, particularly tubular cells, show positive reaction of MUC1. Immunostaining, x200.
Case #2
A 78-year-old man complained of hematuria, and was admitted to our hospital. A blood laboratory test showed no significant changes. Tumors markers were within normal ranges. Bladder endoscopy revealed a nodular tumor and TUR-BT was performed. Histologically, carcinoma cells with hyperchromatic nuclei were seen in the lamina propria (Figure 2A and 2B). No tumor was seen in the surface urothelium (Figure 2A). The carcinoma cells formed small solid nests (Figure 1B). No tubular formations were seen. The histological features resembled proliferated von Brunn's nests. The carcinoma cells had hyperchromatic and enlarged nuclei (Figure 2B). Mucin stains were negative. Immunohistochemically, characteristic findings were positive cytokeratins, EMA, p63, p53 (Figure 2C), Ki-67 (labeling=30%) (Figure 2D), CD10, CEA, and MUC1 (Figure 2E) (Table 1). Since p53 was positive and Ki-67 was relatively high, benign conditions such as proliferated von Brunn's nest were denied.
Case #2. A) Low power view of nested variant of urothelial carcinoma of the bladder. The atypical cells are present in the lamina propria. The surface epithelial cells are free of tumor. HE, x50. B) High power view of A. The atypical cells show moderate atypia, and take a form of nested pattern. The features resemble hyperplastic von Brunn's nests. HE, x 200. C) The atypical cells are positive for p53. Immunostaining, x200. D) The atypical cells show Ki-67 antigen. The Ki67-labeling is 30%. Immunostaining, x200. E) The atypical cells show positive reaction for MUC1. Immunostaining, x200.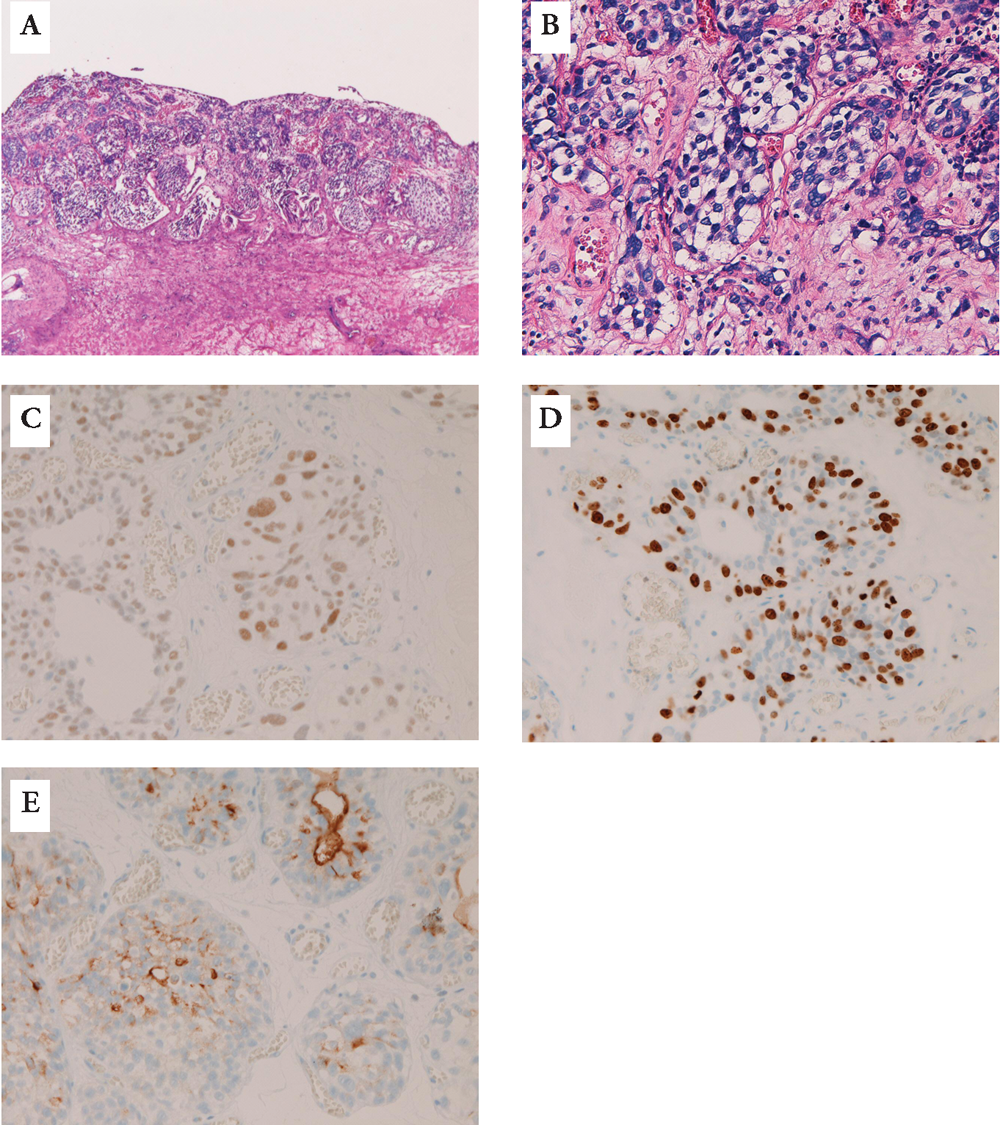
Immunohistochremical findings.

Foot note. CK, cytokeratin. EMA, epithelial membrane antigen. PSA, prostate-specific antigen. AMACR, α-methylacyl CoA racemase ASMA, α-smooth muscle antigen. NSE, neuron-specific enolase. AFP, α-feto protein. ND, not done
The final pathological diagnosis was NVUC of the urinary bladder. The patient is now free of tumor 15 months after TUR-BT, but is strictly followed up.
Discussion
Usual urothelial carcinoma of the bladder may show a nested pattern of invasion. Such a tumor is not NVUC. 1 NVUC of the bladder is free from surface epithelial involvement.1–10 In the present cases, no surface involvements were seen. Therefore, the present cases are compatible with NVUC.
NVUC is characterized by the presence of tumor cells in the lamina propria; the tumor cells are bland and benign-looking.1–10 The NVUC shows mild atypia in the superficial part and relatively severe atypia in the deep areas. However, anaplasia is seen in some areas in the superficial parts. In the present case #1, the atypia was mild, and resembled nephrogenic metaplasia. In the present case #2, the atypia was mild to moderate. In the present two tumors, p53 was positive and Ki67 labeling was relatively high, suggesting that the present cases are malignant. Therefore, the present two cases are compatible with NVUC of the bladder.
NVUC must be differentiated from prominent von Brunn's nest, cystitis glandularis and cystica, nephrogenic metaplasia, inverted papilloma, carcinoid, prostatic carcinoma, paraganglion and paraganglioma. 1 The present tumors, particularly in case #2, are different from von proliferated Brunn's nests, because the present tumors showed mild atypia and immunohistochemical findings of positive p53 and relatively high Ki67 labeling. The present tumors are different from cystitis glandularis and cystica morphologically and immunohistochemically. The present cases, particularly in case #1, are different from nephrogenic metaplasia, because the present cases showed positive p53 and high Ki67 and negative CD10 in case #1. The present cases are different from inverted papilloma histologically and also because the present cases are thought to be malignant. The present cases are different from carcinoid tumor histologically and because the current cases were negative for neuroendocrine markers (chromogranin, synaptophysin, CD56 and NSE). The present cases are not prostatic carcinoma because of negative PSA. The current two cases are different from paraganglion and paraganglioma because of positive cytokeratins and negative neuroendocrine markers.
Immunohistochemical study of NVUC has been done in only one report. 3 Wasco et al., 3 who demonstrated 30 cases of NVUC of the bladder, demonstrated that NVUC was positive for CK7 in 93%, CK20 in 68%, and p63 in 92%. The present study is the first report of extensive immunohistochemical features of NVUC. In the present cases, CK7 was positive in 2/2, CK20 was negative in 2/2, and p63 was positive in 1/2. The present study demonstrated the CK immunoprofile; common findings were positive CDAE1/3, CK CAM5.2, CK7, CK8, CK18, and CK19. CK14, and CK20 was negative in the two cases. EMA was positive in both cases. p53 was positive in both cases and Ki67 labeling was relatively high in both cases. CD10 was positive in 1/2 case. AMACR was positive in 1/2 case. The positive reaction of CEA and CA19-9 implies glandular differentiation of NVUC. The positive MUC1 apomucin also implies glandular differentiation. The negative MUC2, MUC5AC and MUC6 suggest that these apomucin genes were not expressed in NVUC.
Clinically, the NVUC affect predominantly male patients.1–10 Wasco 3 showed that the male to female ratio was 2.3:1. In the present cases, one was male and another was female. The NVUC showed aggressive clinical course in spite of the deceptively benign-appearing histology.1–10 In the present two cases, the follow-up periods are short; 6 and 15 months. The present cases are now of free from tumor. Strict follow-up is needed in the present cases.