
Abstract
A 57-year-old with a 9-year history of increased abdominal girth, presented with increased abdominal pain, anemia, and acute renal failure. His past medical history was only remarkable for a previous lung cancer 21 years ago that was treated with a right upper lung lobectomy. A computed tomography (CT) scan of the patient's abdomen showed a solitary 20×20×25cm cystic splenic mass. The patient underwent an urgent splenectomy. Intra-operatively a large splenic cystic cavity was found with a solid inferior splenic mass. An exhaustive histological analysis of the splenic mass confirmed a clear cell carcinoma with low malignant potential that likely represented a metastatic lesion from the patient's previous distant lung cancer. Postoperatively the patient recovered well and at 1-year followup the patient demonstrated no further evidence of metastatic disease. This case is extremely unique and provides a very rare example of a metastatic solitary clear cell carcinoma to the spleen, with a presumed latency period of more than 20 years.
Introduction
Clear cell carcinoma is a rare tumor cell type that differentiates from epithelial cells and originates from various organs, including the ovaries, endometrieum, kidneys, or lungs.1–4 It is characterized by pale appearing cells that are either fluid or glycogen filled, and in most cases it is considered to be a malignant lesion. Metastatic clear cells to the spleen are extremely rare, with only one case of this previously reported in the English literature to the best of our knowledge. 5
Although the majority of splenic tumors are discovered incidentally or on post-mortem autopsies,6,7 they can uncommonly illicit abdominal pain, abnormal blood cell counts, or acute hemorrhagic shock resulting from splenic rupture. 8 Notably, metastatic tumors to the spleen are rare, and solitary metastatic tumors are also exceedingly rare.9–12 We report here a unique case of metastatic clear cell carcinoma to the spleen with a long latency period of over 20 years.
Case Report
A 57-year-old man with a distant history of a right upper lobe clear cell carcinoma 21 years ago developed an insidious slow-growing left upper quadrant mass associated with intermittent left upper quadrant pain over 9 years. In August 2009, after two weeks of frequent, intermittent, severe, sharp left subcostal and flank pain he sought out a Chinese herbalist. He was provided with a ginseng-based remedy and was urged to seek further professional evaluation.
He presented to medical attention approximately 1 month later in the hospital emergency department. He was hemodynamically stable but his physical examination was significant for a large protuberant abdomen with moderate-to-severe pain to palpation in the left upper quadrant. A complete blood count revealed anemia with a hematocrit of 18.2%, and an electrolyte panel revealed renal failure with a serum creatinine of 3.3 mg/dL. A non-contrast computed tomography (CT) of the chest, abdomen, and pelvis revealed a 20×20×25cm cystic splenic mass (Figure 1). There was no evidence of other primary or secondary tumors outside of the spleen. The right upper lung lobe was not present, which was consistent with the patient's previous surgical history.
Large intra-peritoneal splenic mass. A representative cross-sectional axial CT image demonstrates a large 20 × 20 cm cystic splenic mass in the left upper quadrant of the abdomen. Compared to cystic main body of the splenic mass, the inferio-lateral border appears more solid. There is associated mass effect with lateral displacement of the mesentery and posterior displacement of the left renal complex.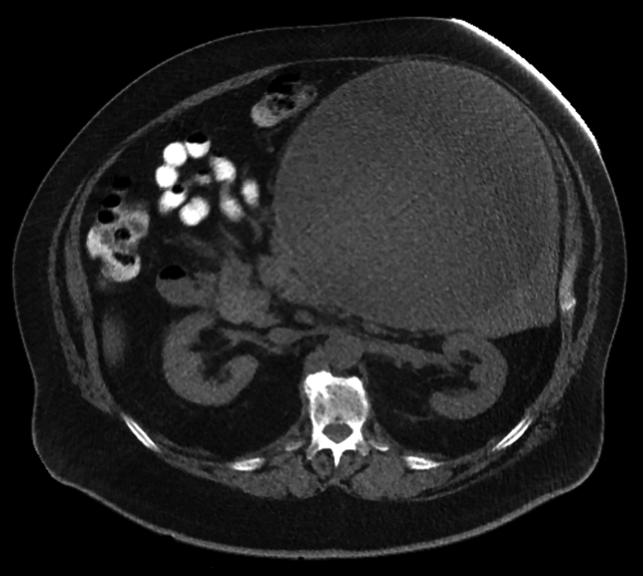
Upon admission the patient was transfused with packed red blood cells and his hematocrit responded appropriately. He remained hemodynamically stable. Based on the patient's symptoms and CT scan findings he was taken urgently to the operating room for an exploratory laparotomy and a splenectomy. Intraoperatively, a very large encapsulated spleen was encountered, and was removed in its entirety (Figure 2A). Variable size small splenules were noted in the peri-splenic fat pad, as well as attached to the gastro-splenic ligament. The abdominal cavity was otherwise normal with no other suspicious findings or masses. There were no palpable lymph nodes.
Postoperative gross appearance of the extracted splenic mass. A) Well encapsulated splenic mass with associated overlying adventitial and adipose tissue. B) Opened cystic cavity of splenic mass reveals an inner surface with course trabecule with fibrinous exudates. A longitudinal section through the inferior pole splenic mass demonstrates a pale appearing solid mass with surrounding red splenic tissue.
On the operating room back table, the splenic mass was found to have a large cystic cavity that contained 4 liters of brownish serous fluid. A large stellate yellow mass measuring 7.1×6.6×3.0cm was found attached to the inferior inner wall of the splenic cystic cavity (Figure 2B). The remaining wall of the splenic cyst was thinned, and its inner surface was covered with coarse trabeculae and adherent fibrinous exudates (Figure 2B). Surrounding the large cyst cavity was beefy red splenic tissue, measuring 3.9 cm in diameter in its extension beyond the cyst.
Postoperatively the patient's hospital course was uncomplicated and he recovered well. His creatinine level remained elevated at 3.1 mg/dL, and a renal ultrasound during the patient's hospitalization demonstrated increased bilateral kidney echogenicity but no masses or hydronephrosis. On postoperative day 5 the patient was discharged from the hospital after receiving post-splenectomy vaccinations.
The splenic tissue and associated mass underwent an exhaustive histological analysis (Table 1) by the Veterans Affairs Palo Alto pathology department, and were also reviewed by colleagues at the Stanford University Medical Center, and the Mayo Clinic at Scottsdale. The specimen showed sheets and clusters of cohesive cells with abundant clear cytoplasm, mildly irregular nuclei and prominent nucleoli (Figure 3A and 3B). Foci of clear cells were found infiltrating surrounding normal splenic tissue as well as the lining of the large cyst wall (Figure 3C and 3D). The findings were most consistent with a low-grade metastatic clear cell carcinoma with squamous features. Investigation of the patient's past medical records suggested that the splenic carcinoma most likely resulted from a delayed metastasis from his prior lung carcinoma.
Histological analysis.

Histological examination reveals clear cells in splenic mass tissue. A) Low magnification image of hematoxylin and eosin (H&E) staining of the inferior pole splenic mass. Islets of interspersed clear cells are observed throughout fibrous sheets. B) High magnification image of H&E staining of splenic mass shows groups of cells with larger clear cytoplasms, with surrounding band of fibrous tissue. C) PAS staining avidly stains cytoplasm of clear cells. D) Pankeratin exclusively stains clear cell clusters.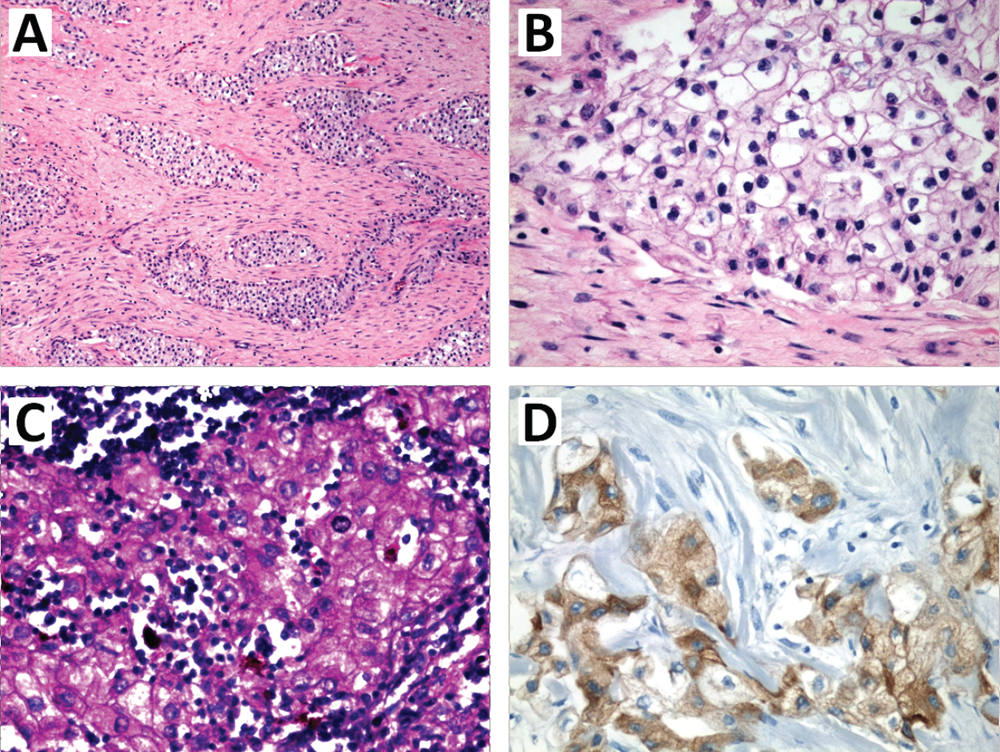
On subsequent 6 month followup, positron emission tomography (PET)-CT demonstrated no scintigraphic evidence of malignancy, once again confirming no other sites of disease. At 6-month followup the patient's anemia had resolved, however his serum creatinine continued to be elevated from baseline with nephritic range proteinuria from presumed glomerulonephritis. Microscopic polyangitis and membranous glomerulonephritis were the leading diagnostic considerations for this, but the patient declined a kidney biopsy to further clarify the diagnosis. At 1-year followup the patient was clinically stable, with no further evidence of malignancy.
Discussion
Clear cell carcinoma of the spleen is an exceedingly rare entity, and to our knowledge there is only one other reported case of this in the literature. 5 Metastatic tumors to the spleen are also rare, and are usually undetected except on post-mortem studies or in patients with advanced or disseminated disease.6,7,13,14 We report here a patient with a metastatic clear cell carcinoma to the spleen. This case is exceptionally unique in that the presumed primary site of the patient's metastatic clear cell carcinoma is from a prior lung cancer 21 years prior, demonstrating an extraordinary latency period that to our knowledge has never been described for metastatic clear cell tumors.
More commonly, clear cell pathology is known to arise in ovarian, endometrial, and renal tumors.3–5,15 In each of these tissues, clear cell tumors are typically associated with aggressive metastatic behavior and poor clinical outcomes. However, clear cell pathology of other tissue types has been described. Pulmonary clear cell carcinomas are a rare entity that are described in a few case reports.16–18 These tumors are not to be confused with benign pulmonary sugar cell tumors, which also have a large clear cytoplasm but are distinguished by perivascular epithelioid cell markers.19–21 Given the scarcity of reported pulmonary clear cell carcinoma cases, little is known about the malignant potential of these tumors and their prognosis.
Interestingly, the spleen is typically considered to be a hostile site for neoplastic implantation, explaining the reported low incidence of splenic metastatic lesions that are usually encountered and reported in the literature.6,16,22 This phenomenon is partially explained by the spleen's reservoir for cellular immunity, which may inherently infer significant anti-neoplastic properties. Anatomically, the spleen also lacks afferent lymphatics, has a tortuous splenic artery, and rhythmically contracts. These features may decrease the likelihood of neoplastic implantation to the splenic parenchyma.22,23
Despite these protective features, metastatic lesions to the spleen can occur and have been rarely reported in several case series.6,10,14 Earlier series suggested that primary gynecological tumors accounted for the majority of distant metastases to the spleen,10,24–27 but tumors from other tissue such as the breast, colon, and skin can also metastasis to the spleen at lower rates.9,10,28 More recent studies suggest that the majority of metastatic lesions to the spleen arise from the lungs. 29 In a summary of 713 clinical and post-mortem patient records, 21% of splenic metastasis were found to originate from primary lung tumors. 6 The discrepancy in metastatic lesions from primary tumor sites likely reflects the differences in clinical behavior and the treatment of different types of advanced metastatic cancer over time, the aggressiveness of the primary disease process, as well as possible sampling error associated with the examination of different study populations. Despite these differences, all studies similarly conclude that distant metastasis to the spleen occurs at a very low incidence ranging between 0.6–1.7%.6,10 Isolated splenic metastasis, as described in this case, is an even rarer finding with only approximately 50 reported cases of this in the literature.6,30–34
To confirm our pathological diagnosis ancillary and immunohistochemical analysis of the splenic mass specimen was vital (Table 1). Infiltrating clear cells within the inferior pole splenic mass were found to avidly stain with PAS (Figure 3C), which is consistent with extensive glycogen deposits in the clear cell tumor cytoplasms.21,35 Furthermore, consistent with previous reports, clear cells were found to be of epithelial origin (positive for Pankeratin, Figure 3D; and Cytokeratin 7), but negative for other cell type markers.36,37 Markers for other metastatic lesions, such as primary extrapulmonary sugar cell tumor (PEST), renal cell carcinoma (RCC), and mesothelioma were also negative (Table 1). Interestingly, Ki-67 staining demonstrated low tumor mitotic activity, which is consistent with the tumors presumed remarkably long latency period and indolent slow growth.
In summary, we present an exceedingly rare case of a solitary metastatic clear cell carcinoma to the spleen that likely originated from a previous lung cancer more than 20 years earlier. The case provides insights about the malignant potential of clear cell carcionoma, and their potential metastatic sites, including the spleen. For patients with solitary metastasis to the spleen, splenectomy and continued surveillance are excellent treatment options with a potentially good outcome.