
Abstract
Synchronous endometrial and cervical cancer is a very rare condition. This report describes a case of a 46-year-old woman who presented with a cervical mass that measured 5.6 cm along its longest diameter, whose biopsy analysis revealed an endocervical mucinous adenocarcinoma. She was classified as having an IB2 cervical carcinoma and treated with concurrent chemoradiation plus hysterectomy. Pathological and immunohistochemical analysis of the surgical specimens revealed a synchronous endometrioid grade 2 adenocarcinoma in the endometrium, and a well-differentiated mucinous adenocarcinoma in the cervix. Magnetic resonance imaging (MRI) studies performed prior to treatment were reviewed and apparent diffusion coefficient (ADC) maps were generated. The ADC values demonstrated distinct signal intensity differences between the endometrial and endocervical tumors. In conclusion, diffusion-weighted MRI and ADC maps can help to distinguish the site of origin of synchronous tumors.
Keywords
Introduction
Synchronous endometrial and cervical cancer is a very rare condition, which generally presents as an adenocarcinoma in the endometrium and a squamous cell carcinoma in the cervix.1–4 Even rarer is the occurrence of adenocarcinoma of the uterine cervix associated with an endometrial adenocarcinoma.5,6 The distinction between cervical and endometrial adenocarcinomas can be very difficult because of overlapping morphological features.7–9
Diffusion-weighted imaging (DWI) is a technique used to show tissue characteristics based on the diffusion motion of water molecules that is known as Brownian motion. 10 DW imaging can also provide quantitative measurement of apparent diffusion coefficient (ADC) value, which is considered to be influenced by cellular density in solid tissues. 11 The ADC is an indicator of the movement of water within the tissue. Decreased ADC values in malignant tumors compared with normal tissues or benign lesions have been previously reported in various organs. 12
DWI for uterine cervical cancer and ADC values of cervical cancer differ from those of the normal cervix, and could be used to indicate the histological type and the pathological grade of tumor. 13 Furthermore, it could distinguish between most uterine adenocarcinomas originating from the cervix and endometrium. 14 To the best of our knowledge, this is the first report of a synchronous endometrial and endocervical adenocarcinoma analyzed by DWI and ADC values.
Case Report
A 46-year-old woman presented with a 3-month history of vaginal bleeding during intercourse. A gynecological examination revealed a cervical mass measuring 5.6 cm along its longest diameter. Biopsy analysis revealed an endocervical adenocarcinoma, histological grade 1 (Figure 1A). It was staged as IB2, according to guidelines of the International Federation of Gynecology and Obstetrics (FIGO). 15
A) Adenocarcinoma seen in the cervical biopsy prior to treatment. Neoplasia with villoglandular architecture with low grade nuclei and signs of mucin secretion (hematoxylin-eosin; original magnification ×100); B) Endometrial adenocarcinoma after treatment showing glandular and cribriform architecture and intraglandular foci of necrosis (hematoxylin-eosin; original magnification ×100).
The patient underwent concurrent chemoradiation followed by a simple hysterectomy. Pathological analysis of the surgical specimen revealed residual tumor involving only the body of the uterus. The residual tumor was classified as a grade 2 endometrioid adenocarcinoma, which was positive for estrogen and progesterone receptors and vimentin (Figure 1B). The endometrial tumor infiltrated less than 50% of the myometrium. These findings were consistent with a diagnosis of synchronous endometrial and endocervical adenocarcinoma.
Magnetic resonance imaging (MRI) studies performed prior to the treatment were reviewed. The ADC maps prior to treatment were also generated. In these maps, neoplastic tissue was associated with heterogeneous, hypointense areas. Regions of interest were identified by MRI and indicated with white boxes within the ADC maps, and ADC values associated with these regions were 0.72±0.18×10−3 mm2/s (Figure 2C) for the endometrial tumor and 0.59±0.12×10−3 mm2/s for the cervical tumor (Figure 2C). Figures 2A and 2B, representing the sagittal and coronal T2-weighted images that demonstrate both masses, were present in both the endometrial cavity and the endocervical canal. Each was associated with distinct signal intensities.
A,B) Sagittal and coronal T2-weighted images that demonstrate masses in both the endometrial cavity and the endocervical canal; each is associated with distinct signal intensities; C) apparent diffusion coefficient (ADC) maps generated prior to treatment.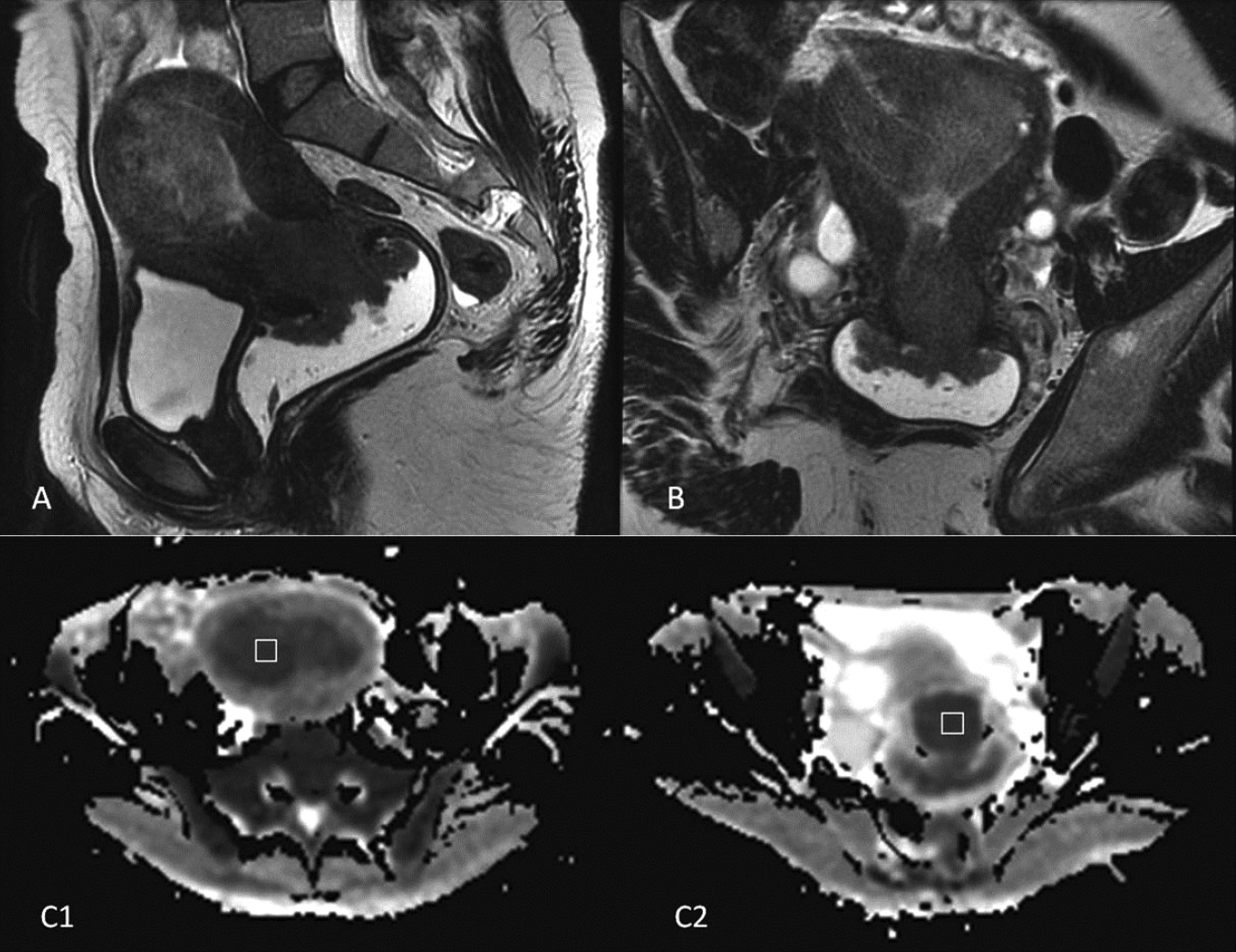
Discussion
Neoplastic involvement of the uterine body and cervix often raises important discussions about the primary site, as treatment options are quite different. Preoperative diagnosis of biopsy or curettage is frequently inconclusive. Determining the primary site of a uterine adenocarcinoma when both the uterine body and endocervix are involved can be problematic due to the overlapping morphology of endocervical adenocarcinomas and endometrial carcinomas. The hypothesis of synchronous tumors for these two adenocarcinomas has been rarely identified, although it is possible that this event is more common that currently estimated.
The majority of adenocarcinomas that involve the cervix and endometrium have a similar morphology. Despite many of these tumors being classified as primary endometrial cancers that involve the cervix, or primary cervical cancers that involve the endometrium, at least some of these cases may be a result of two different primary neoplasms.
To the best of our knowledge, this is the first report of the use of MRI and ADC to differentiate synchronous endometrial and endocervical adenocarcinomas. DWI has the potential ability to differentiate between normal and cancerous tissue in the uterine cervix, 13 but it appears to be useful for differentiating synchronous tumors arising from the endometrium and cervix.
The differential diagnosis between primary endometrial or endocervical cancer is very difficult with routine hematoxylin and eosin staining, and even with aid of immunohistochemistry (IHC). The common immunomarkers used to determine cell differentiation are vimentin, carcinoembryonic antigen, estrogen receptor, progesterone receptor and p16, but IHC studies are often unhelpful for differentiating between synchronous endometrial and endocervical tumors, especially those of the endometrioid type. 9
In our case the morphology of the two tumors was distinct in the cervix and endometrium, being, respectively, of the endocervical and endometrioid histological type, which suggested the diagnosis of synchronous endometrial and endocervical adenocarcinoma, although this was initially unsuspected. The patient was treated as a case of IB2 (FIGO) cervical cancer and received chemoradiation plus laparoscopic hysterectomy and bilateral salpingo-oophorectomy as this was a bulky tumor. After reviewing the MRI scan performed prior to treatment, we noted that the sagittal and coronal T2 weighted images showed concurrent masses in the endometrial cavity and the endocervical canal with a clear difference in signal intensity (Figure 1A and 1B). ADC maps (Figure 1C) showed neoplastic tissue as heterogeneous hypointense areas. Regions of interest placed into those areas and ADC values confirmed different patterns of ADC in the endometrial and cervical tumors.
Conclusion
Synchronous endometrial and endocervical adenocarcinomas are extremely rare conditions. As adenocarcinomas from the endometrium and the endocervix often present with a significant overlap of morphological and immunohistochemical features, the correct diagnosis can be very difficult. Moreover, when the adenocarcinomas are located in both the endometrial and endocervical canals, it is very difficult to determine the exact site of tumor origin using conventional imaging methods. DWI is a magnetic resonance technique that, at the microscopic level, can identify differences in water mobility in extracellular spaces. Correspondingly, in the present case, diffusion-weighted MRI and ADC maps helped to distinguish the origin of both tumors.