
Abstract
Tumefactive fibroinflammatory lesion (TFIL) is a rare benign tumor in the head and neck region. We present a case of a 40-year-old female with a benign but progressive lesion of the infratemporal fossa, which was diagnosed as TFIL. Patient responded briefly to a course of steroid treatment but eventually showed progression and was unresponsive to further steroids. She was then treated with external beam radiation to a dose of 60 Gy in 30 fractions. After radiation a slow, gradual decrease in tumor size was noted over the course of years and she is free of disease after more than 11 years of follow-up. The major long-term side effect this patient developed was an expected unilateral radiation-induced retinopathy, due to the close proximity of the lesion to the orbit. The dilemma of treatment of benign disease with radiation with potential long-term complications is discussed and a review of the literature on TFIL is presented.
Introduction
Clinicians are sometimes confronted with a patient presenting with a malignant-appearing mass as based on clinical characteristics (size, location and nature of growth, e.g. infiltrative or destructive) and details from the medical history (fashion of appearance and rate of progression). Despite this presentation however, the nature of this mass may be related to a condition with a benign histological appearance.
In the medical literature, these lesions have often been described as inflammatory pseudotumors (IPT), 1 however multiple other terms have been used to describe these, depending on the site of occurrence, the organ of origin or the predominant pathologicafeatures, e.g. plasma cell granuloma of the lung, 2 xanthogranuloma, 3 or histiocytoma. 4 Overall, these tumors are rare and difficult to classify because of the lack of clear diagnostic criteria, leading to the use of multiple synonyms. In general, they can be categorized as non-neoplastic, fibroinflammatory proliferations.
Within the broad spectrum of IPT's, a condition named tumefactive fibroinflammatory lesion (TFIL) is a rare idiopathic fibrosclerosing disorder occurring in the head and neck region, which has a locally destructive nature but is characterized by a benign histological appearance. As this is not a malignancy, there is no tendency for metastases. However, the clinical behavior with locally aggressive growth and the surgical findings of infiltration resemble those of an invasive malignancy. Because of the discrepancy between the aggressive clinical manifestation and the benign histological features, these lesions often pose a dilemma in terms of diagnosing and treatment. Rice et al. 5 first described the abnormality in 1975 as sclerosing cervicitis. It was first named tumefactive fibroinflammatory lesion by Wold et al. 6 in 1983. The lesions usually develop in the head and neck region, although they rarely arise in other areas like the extremities.7;8 Treatment strategies for this benign lesion are not well defined and are based on individual reports, including the use of high-dose steroids, surgery and radiation treatment, all with varying results. Little information is available on the results of radiation treatment as this has only been the treatment of choice in a few cases in literature.5;9;10
In this paper we present a case with an infiltrative lesion in the infratemporal fossa diagnosed as TFIL, which appeared to be refractory to and progressive on steroids and was treated with definitive radiotherapy. The extent of surgery that would have been required to resect it was regarded as unacceptable to the treatment team and the patient, without first considering other options. The issues of difficulties in establishing a pathological diagnosis will be described and we will present a review of the available literature on TFIL.
Case Report
Clinical presentation
A previously healthy 40-year-old female presented in 1997 at the Princess Margaret Hospital with a 3–4 months history of an increased swelling in her right temporal area. She underwent initial investigations elsewhere including plain skull film x-rays and a bone scan, which did not show any abnormality. She then developed progressive sensations of pressure with pulsatile aching in the temple region and also in her right eye and upper teeth on the right side. There were no complaints suggestive of diplopia, facial nerve paralysis, hearing loss, tinnitus or vertigo. The lesion did not change dramatically in size since the first presentation. She did not present any constitutional symptoms, or any weight loss. She was a non-smoker and reported no alcohol abuse. There was no history of radiation exposure. She had a previous history of tubal pregnancy and a tubal ligation in 1994. Her family history was positive for a brother who died at age of 5 secondary to a brain tumor of indeterminate histology.
On physical examination, an 8×6 cm hard, non-tender, fixed mass in the right infratemporal fossa was noted, which extended deep to the zygoma bone into the infratemporal fossa. The overlying skin was mobile without any skin involvement. There were no signs of trismus or proptosis, and cranial nerve examination was normal. The reported symptoms of one episode of paraesthesia over her right face in the V2 and V3 distribution could not be correlated with obvious signs of trigeminal nerve involvement.
Imaging was performed using magnetic resonance imaging (MRI). On these a large ill-defined swelling in the right temporal fossa was noted, superficially extending over the right parotid region, and involving the scalp, superficial subcutaneous tissues and the temporalis muscle. The mass was in close proximity to lateral aspect of the right orbit. On T2-weighted images, increased signal intensity was noted in the lesion and area of the involved temporal muscle. The lesion had an intermediate high signal on T1 and showed clear enhancement after gadolinium administration. The mass was measured as 6.0×2.0×4.0 cm in the anterior-posterior, transverse and cranio-caudal directions, respectively.
Based on the clinical presentation a differential diagnosis of rhabdomyosarcoma, fibrosarcoma or fibromatosis was made. To obtain a histological diagnosis, an incisional open biopsy was performed. During this procedure, the lesion appeared as an extremely hard, white, firm mass enveloping the temporal muscle and it was noted to have become confluent with the muscles.
Pathology
The mass consisted of a hypocellular lesion composed of bland fibroblasts and myofibroblasts surrounded by dense eosinophilic collagen extending into striated muscle and adipose tissue. The mass showed a striking perivascular infiltrate of small lymphocytes and plasma cells. Scattered plasma cells, small lymphocytes, and mast cells were present in the collagenous tissue. No cellular atypia, necrosis, or mitoses were seen (Figure 1A and 1B). Immunohistochemical stainings were performed on the tumor sample and showed that many of the spindle cells were positive for smooth muscle actin (SMA) and muscle specific actin (MSA) and negative for desmin. Based on this, at that time the diagnosis of tumefactive fibroinflammatory lesion (TFIL) was made. For the purpose of this case report, the original tumor block was retrieved for additional immunohistochemical stainings. These studies showed that the spindle cells were negative for CD30, CD34, Alk-1, β-catenin, and epithelial membrane antigen (EMA) (Figure 1C). These results confirmed the fibroblastic and myofibroblastic phenotype of the spindle cells, consistent with the original diagnosis of TFIL.
Hypocellular mass composed of bland fibroblasts and myofibroblasts surrounded by abundant collagen (A). Perivascular aggregate of small lymphocytes and plasma cells (B). Scattered spindle cells positive for actin consistent with myofibroblasts (C).
Treatment and clinical outcome
In multidisciplinary setting, the treatment approach was established. A complete thoracic and abdominal imaging work-up was done to rule out other manifestations of idiopathic fibrosing conditions such as retroperitoneal fibrosis, and this revealed no abnormalities. Given the extent of disease it was decided to start with steroid treatment, and reserve radiation treatment for any failure. Based upon the extent and location of the disease, surgical management would be associated with cosmetic and functional disabilities, and therefore considered only if no other options would be available. She was started on prednisone 80 mg daily for about 1 month and was then slowly tapered to 60 mg daily, partly due to side effects, especially insomnia. On re-assessment about 3 months after the start of steroids, the tumor had responded to steroid treatment as it was measured on physical examination as 3.5×4 cm in size. The prednisone dose was subsequently tapered to 50 mg over the course of 1 month. At that time, progression in tumor size was noted clinically, now measuring approximately 7×5 cm, which was confirmed by repeat MRI.
Because of the progression during steroid treatment, it was decided to treat the patient with radiation therapy. It was anticipated that this could potentially have a high likelihood of late toxicity in terms of radiation-induced retinopathy, given the close proximity of the tumor to the right orbit and right optical structures. The patient was informed of this risk before RT was commenced. In the period of May-June 1998, a dose of 50 Gy in 25 fractions was delivered with 6 MV photons using a wedged right anterior-oblique and apical field. This was followed by another 10 Gy in 5 fractions with modified shielding in order to protect the right eye, using the same field setup, resulting in a total dose of 60 Gy in 30 fractions.
Following radiation treatment, the patient was followed regularly to assess the treatment response. After treatment, repeat imaging was performed on multiple occasions. The first post-treatment MRI scan also depicted the pre-treatment tumor extent since on this scan no reduction in size of the abnormality compared to pre-radiotherapy had occurred yet (Figure 2, 1998 October). Regression of the size of the lesion following radiation treatment was very slow with little change over the course of the first 2 years and a gradual decrease in size over the next years. At the latest imaging performed in February 2007, residual soft tissue changes were still present in the infratemporal fossa, but stable compared to 2003 (Figure 2).
Coronal T2 Fatsat magnetic resonance imaging during follow-up of patient after radiation treatment. Note the slow regression of the large lesion in the right infratemporal fossa. The 1998 October scan (post-radiation scan) also depicts the pre-treatment tumor extent, since no regression of tumor size was present yet at that time.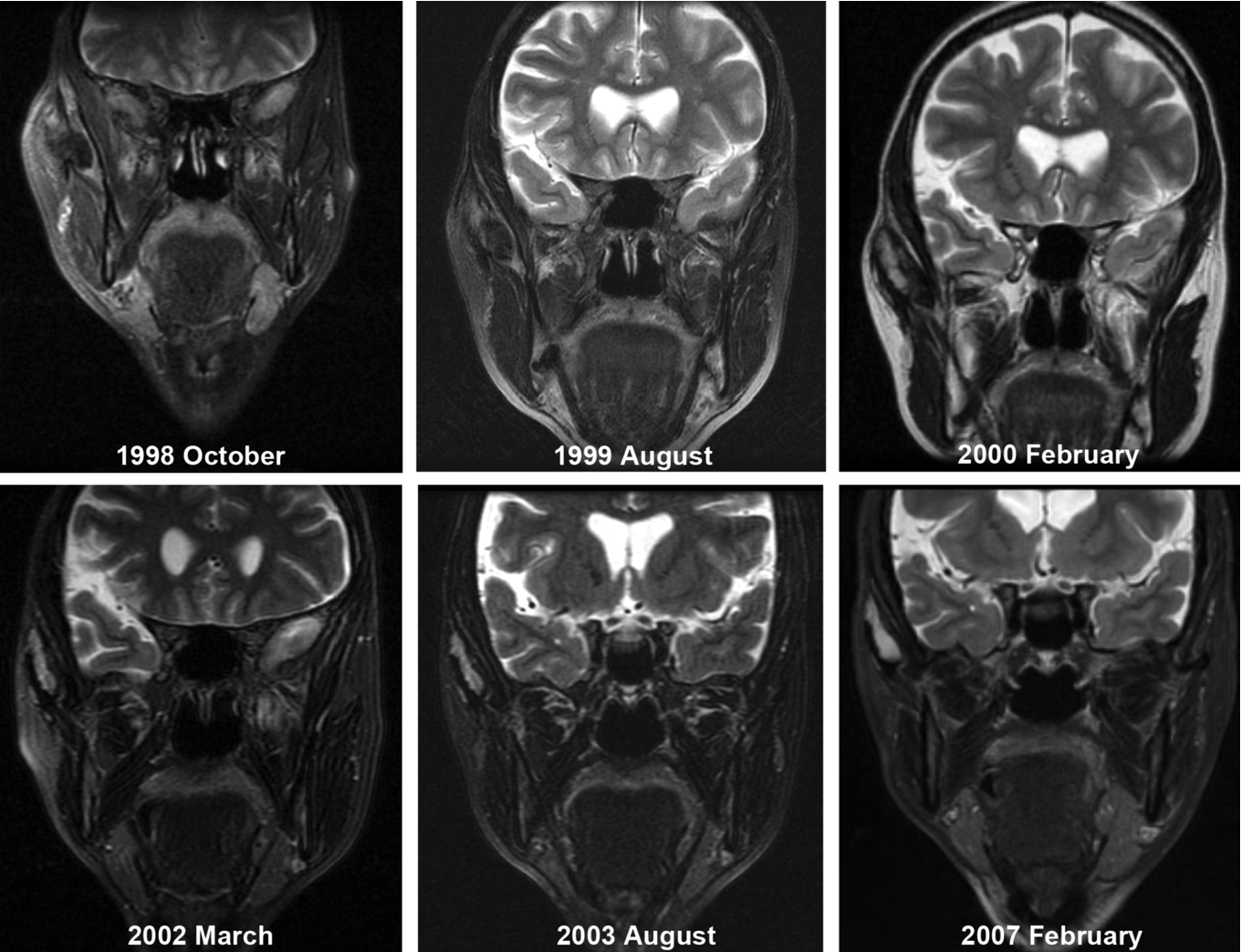
Because of the close proximity of the optical structures in relation to the radiation fields, the patient was followed by an ophthalmologist because of concerns for late optical radiation toxicity. At her first visit, shortly after the end of radiation, minimal asymptomatic cataract in her right eye was seen, which did not require any intervention. After 2 years of follow-up, one cotton wool spot in the macular area was described, which would be consistent with radiation-induced early retinopathy changes. This remained stable without any visual disturbances and without any treatment until 8 years after treatment. At that time she presented with blurring and clouding of vision. Fundoscopy of the right eye showed a macular hole, and fluorescein angiography subsequently demonstrated cystoid macular edema with a few dot reddish lesions suggestive of either blood or macular aneurysms. The diagnosis of radiation-induced retinopathy was made and she was then treated with intravitreal injections of the anti-VEGF (Vascular Endothelial Growth Factor) agent bevacizumab at six-weekly intervals. This resulted in an improved vision. However, at the end of the six weeks periods, the patient would develop recurrent blurred visions, which again would improve upon receiving the next bevacizumab injection. This treatment is being continued until present.
The patient was last seen in the Head and Neck Clinic in March 2010 with more than 11 years of follow-up after the end of radiation treatment and there were no signs of disease progression and no changes in her physical examination, compared to previous visits. Because the clinical situation has remained unchanged for several years with no suspicious findings in physical examination, no radiological evaluation has been performed after 2007. She was still receiving the intravitreal injections with bevacizumab and had a stable vision of the affected eye. The vision in the contralateral eye remained unaffected.
Discussion
This case report describes a patient presenting with a locally infiltrating but histological benign lesion that progressed after initial medical treatment using steroids. The confirmation of the benign nature of this lesion, yet with a locally progressive behavior posed a dilemma in terms of clinical management, especially given the risk of long-term toxicity associated with radiation to a target in close proximity of important normal structures like the visual system. However, radiation was chosen over surgery because of functional and cosmetic concerns following an extensive resection in this anatomical area.
The lesion was diagnosed and treated as TFIL, which is a rare benign disorder that mimics a locally aggressive malignancy. It usually presents clinically as a stony hard lesion and multiple sites in the head and neck area may be present at diagnosis. Outside the head and neck area, TFIL is reported with no more than 2 case reports available in the literature.7;8 Microscopically, fibrous tissue with the presence of collagen is seen with an associated infiltration of lymphocytes, plasma cells, neutrophils and eosinophils. TFIL can invade vascular structures and muscle 10 and cause extensive bony destruction,5;10 as well as invasion of the meninges and brain involvement. 11
Lesions diagnosed as TFIL in the head and neck region are believed to be part of the broader fibrosclerosing syndrome that includes pseudotumour of the orbit or base of skull, 12 Riedel's thyroiditis, sclerosing cholangitis, 13 lacrimal gland fibrosis, fibrous parotitis and mediastinal or retroperitoneal fibrosis. In fact, in some patients manifestations of the same disease may occur in multiple organs. Cheng et al. 14 reported on a case of TFIL in the nasal cavity, who developed Riedel's thyroiditis subsequently.
To the best of our knowledge, only 33 cases of TFIL involving the head and neck region have been reported in literature so far, including the present case (Table 1).5;9–11;14–25 In TFIL, medical treatment with steroids has been suggested as first line of management in cases with TFIL. 21 Treatment with surgery is used to relieve symptoms of compression. Radiation therapy is reserved for failures. Information on the use of radiaton is limited for TFIL5;9;10 in terms of total dose and fractionation, with only 5 cases reported in literature. In 1 report on 3 cases, no details were provided on the prescribed radiation dose. 10 In two other cases, 50 Gy in 25 fractions was administered to disease located in the head and neck area.5;9 In IPT of the base of skull, low dose radiation (20 Gy) proved to be ineffective with poor disease control reported in 6 patients. 23 In our case, it was decided to deliver a total dose of 60 Gy. This was mainly because surgical salvage treatment after a potential failure following radiation was considered to be mutilating if surgery would have to involve resection of (part of) the orbit and contents.
Overview of reported cases of Tumefactive fibroinflammatory lesion of the head and neck in literature.
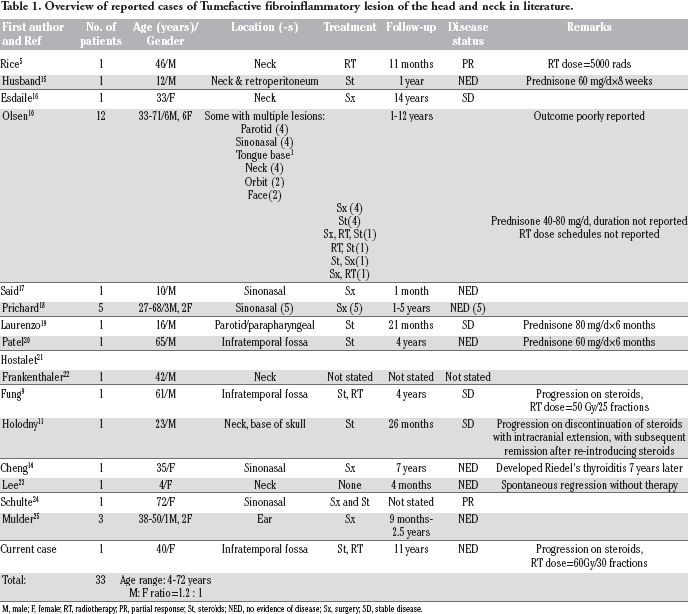
M, male; F, female; RT, radiotherapy; PR, partial response; St, steroids; NED, no evidence of disease; Sx, surgery; SD, stable disease.
As apparent from the experience reported in literature (Table 1), TFIL will in most cases only show a limited radiographic response after radiation treatment. In 3 cases treated with radiation therapy from the series of Olsen et al., 10 a complete regression was observed in 1 patient and stabilization in 2 after radiation. In a surgically unresectable case reported by Rice et al., 5 tumor size stabilization was reported as response to treatment. A similar response with stable disease following radiation treatment was seen in a case reported by Fung et al. 9 This pattern of response was confirmed in our patient as well. However, if left untreated or unresponsive to steroids, TFIL may progress to involve the base of skull, meninges, cavernous sinuses, brain and orbit. 11
Given the recent advances in characterization of benign soft tissue lesions, we performed additional (immuno-) histochemial analysis on this patient's archived specimen. A differential diagnosis of this lesion was the inflammatory myofibroblastic tumor (IMT), 26 which has been defined within the category of IPT with distinct clinical pathological and molecular features. 27 IMT is spindle cell proliferation with a variable inflammatory component, which mainly occurs in the lung, but has also been reported in extrapulmonary sites, including the mesentery, genitourinary system, retroperitoneum and pelvis, upper respiratory system, trunk and head and neck area. The frequency of occurrence in the head and neck varied from 0% to 29% accross different case series. 28 It involves mainly children and adolescents. 29 IMT often show distinct molecular features, consisting of rearrangements involving the ALK (anaplastic lymphoma kinase) locus on chromosome 2p23 30 and approximately 50% of IMTs are positive for ALK on immunohistochemistry. 27
However, based on the findings of the immunohistochemial analysis, we were unable to prove that this lesion was a case of IMT and concluded that the lesion was still to be classified as TFIL. The clinical characteristics of our patient were also in favor of this diagnosis: as opposed to IMT, tumefactive fibroinflammatory lesions tend to occur more often in older patients (not children and adolescents), often show a more ill-defined mass entrapping normal tissue and on pathology TFIL tend to have more sclerosis and a patchy, predominantly lymphocytic inflammatory infiltrate. 27
The etiology of the inflammatory pseudotumors is unknown and the pathophysiology remains poorly understood. An exaggerated response to (chronic) infection has been suggested to be a possible mechanism. 31 Others have suggested an autoimmune reaction linked to previous (viral) infection. 32 However, evidence for any of these theories is sparse and inconclusive.
In our patient, the late radiation toxicity in terms of retinopathy became apparent not until 8 years after treatment. This highlights the need for long-term follow-up of toxicity in patients at risk. In the case described, the retinopathy was due to radiation dose to the orbital structures, in an era in which conformal radiation or IMRT (Intensity Modulated Radiation Therapy) were not available. Nowadays, these types of toxicities may be prevented by means of dose sculpting around the normal structures. Radiation-induced retinopathy has long been recognized as an irreversible process leading to loss of vision. 33 Recently, the use of bevacizumab, a humanized anti-VEGF monoclonal antibody has been reported to result in clinical improvement of symptoms from radiation-induced retinopathy. 34 as was evident from our case.
In conclusion, tumefactive fibroinflammatory lesion of the head and neck is a rare benign diagnosis that can present as a locally progressive tumor. In case it is refractory to steroid therapy, radiation can be considered if surgery would be mutilating, but care has to be paid in order to prevent (late) radiation-induced toxicity.