
Abstract
Small cell carcinoma of the uterine cervix is a rare form of cervical cancer characterized by extreme aggressiveness and poor prognosis because of its rapid growth, frequent distant metastases, and resistance to conventional treatment modalities. We report here a case of advanced-stage small cell carcinoma of the uterine cervix treated by neoadjuvant chemotherapy, followed by radical surgery, resulting in locoregional disease control. A 39-year-old Japanese woman was diagnosed as having stage IIIb small cell carcinoma of the uterine cervix. She was treated by neoadjuvant chemotherapy with irinotecan/cisplatin, followed by extended radical hysterectomy with pelvic and paraaortic lymphadenectomy. The patient was further treated by adjuvant chemotherapy with irinotecan/cisplatin. Intrapelvic recurrence has not been detected throughout the postoperative course. However, the patient died with distant metastases of the disease, 27 months following the initial treatment. It has been suggested that neoadjuvant chemotherapy therapy followed by radical surgery is a treatment option for advanced-stage small cell carcinoma of the uterine cervix for the locoregional disease control. Further studies are necessary to obtain information regarding multimodal treatment including sequence, duration, frequency, and type of effective chemotherapy agents to be used in the treatment of small cell carcinoma of the uterine cervix.
Introduction
Small cell carcinoma is the most common neuroendocrine tumor of the uterine cervix. It has been estimated that it may account for approximately 0.3–3% of all cervical carcinomas.1–12 The clinical behavior of small cell carcinoma of the uterine cervix is similar to that of small cell carcinoma of the lung,5,6 and differs from the more commonly seen squamous cell or adenocarcinoma of the cervix. Small cell carcinoma of the uterine cervix is usually not confined to the cervix at the time of diagnosis, as it tends to spread to bone, brain, lung, and liver tissues.2,11,12
It is extremely aggressive and has an unfavorable outcome, due to the early development of lymph node and distant organ metastases and vascular invasion.1–3, 5,7,10,11 An optimal initial therapeutic approach to this rare disease, especially at an advanced stage, has not yet been clearly defined. However, it has been generally accepted that small cell carcinoma of the uterine cervix should be treated by multidisciplinary therapy, including surgery, chemotherapy, and radiotherapy.2–4,6,12,13 In this report, a case of advanced-stage small cell carcinoma of the uterine cervix treated with neoadjuvant chemotherapy, followed by radical surgery and adjuvant chemotherapy is described. Current strategies for the multimodal treatment of this rare tumor type are also discussed.
Case Report
A 39-year-old Japanese woman (gravida 3, para 1) was admitted complaining of lower abdominal pain. Gynecological and rectal examinations showed macroscopic cervical cancer (6 cm in diameter), which had infiltrated to the pelvic wall. Bilateral inguinal and femoral lymph nodes were not evident. The pathological diagnosis of a punch biopsy taken from the uterine cervix was primary small cell carcinoma (Figure 1). No distant metastasis was detected by chest X-ray, intravenous pyelogram, cystoscopy, or colon fiberscopy. Computed tomography (CT) and magnetic resonance imaging (MRI) revealed an enlarged uterine cervix (64×58×64 mm) and paraaortic and pelvic lymph node metastases (Figure 2A). Serum level of tumor markers were as follows: neuron-specific enolase (NSE), 12.9 ng/mL (<10 ng/mL); pro gastrin-releasing peptide (GRP), 398 pg/mL (<46.0 pg/mL); squamous cell carcinoma antigen, 1.3 ng/mL (<1.5 ng/mL); and Cyfra 21-1, 1.4 ng/mL (<2.3 ng/mL). The patient was diagnosed with stage IIIb uterine cervical cancer, according to the International Federation of Gynecologists and Obstetricians (FIGO) classification system (1994). The patient had also previously been diagnosed with type 2 diabetes mellitus.
Magnetic resonance imaging findings at initial diagnosis (A) and after 2 courses of neoadjuvant chemotherapy (B). (A) Magnetic resonance imaging at initial diagnosis revealed an enlarged uterine cervix (64×58 mm). (B) After 2 courses of neoadjuvant chemotherapy, a significant decrease in tumor size was achieved.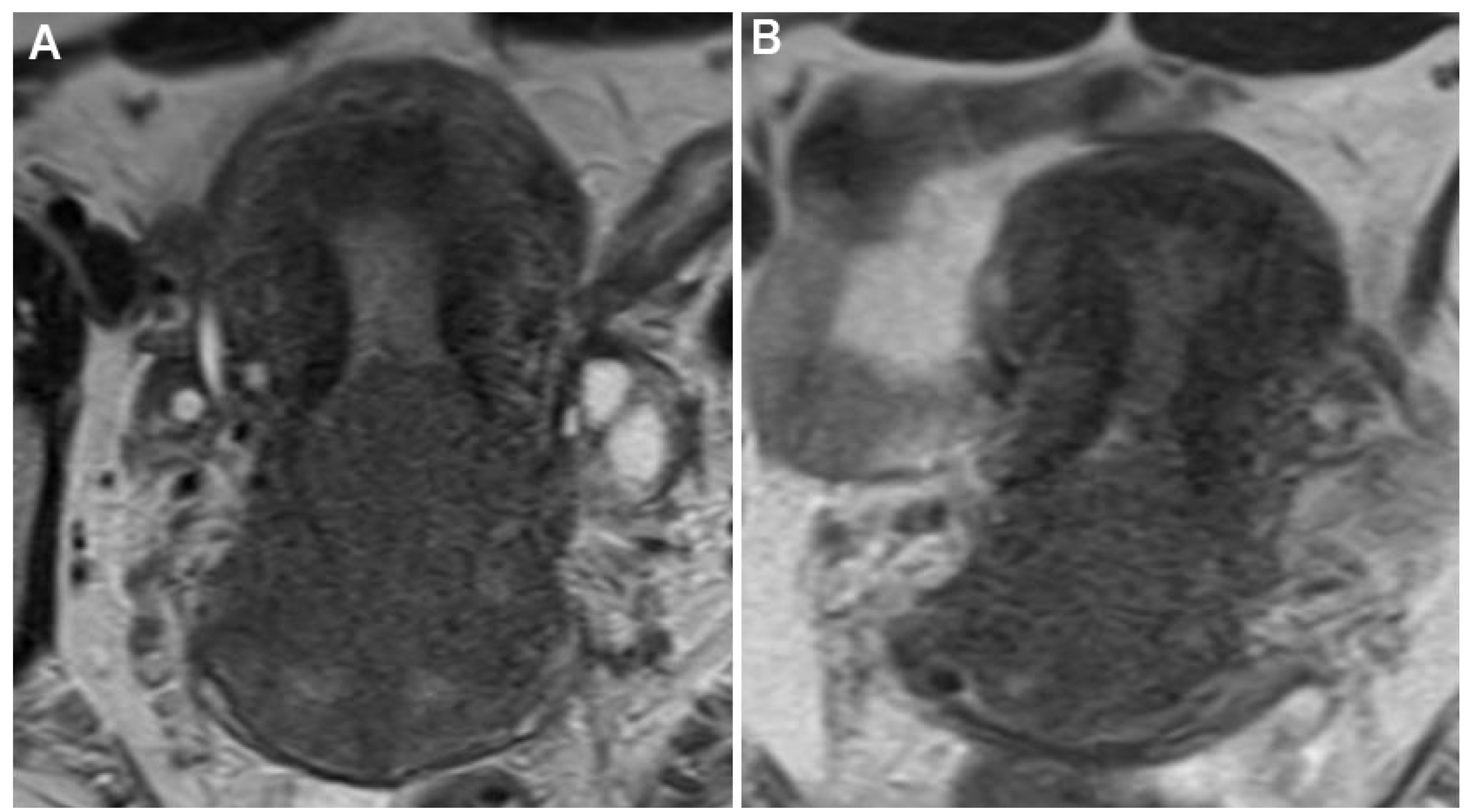
Immunohistological findings of the biopsied specimen. A, H&E; B, MNF116; C, chromogranin A; D, TTF-1 (original magnification ×400). The tumor showed typical features of small cell carcinoma. The tumor was densely cellular and showed trabecular nesting or a sheet-like pattern. The nuclei of the tumor cells were hyperchromatic. The cells had scant cytoplasm, round nuclei, an absence of nucleoli, and finely dispersed chromatin closely resembling the cells of oat cell carcinoma of the lung. Nuclear molding, single cell necrosis, and high mitotic activity were seen in all tumors. No areas of glandular or squamous differentiation were identified. Immunostaining revealed that the tumor cells were positive for MNF116 and chromogranin A and negative for TTF-1.
Immediately after the cancer diagnosis, neoadjuvant chemotherapy with irinotecan (60 mg/m2, days 1, 8, and 15) and cisplatin (60 mg/m2, day 1). After 2 courses of irinotecan/cisplatin, the size of the cervical tumor had significantly decreased (54% decrease) (Figure 2B). Paraaortic and pelvic lymph nodal swelling had also decreased. Subsequently the patient underwent extended radical hysterectomy with pelvic and paraaortic (below the origin of the inferior mesenteric artery) lymphadenectomy. Pathologically, viable tumor cells were identified in the uterine cervix and in numerous paraaortic and pelvic lymph nodes.
Subsequently, adjuvant chemotherapy with irinotecan/cisplatin, which was effective in the neoadjuvant setting, was reintroduced. After 5 courses of postoperative chemotherapy with irinotecan/cisplatin, tumor recurrence was identified in the paraaortic lymph nodes. Second-line chemotherapy with amrubicin (45 mg/m2, day 1-3, 21 day-cycle) was started. The lymph node swelling disappeared after 2 courses of amrubicin. However, the tumor recurred again after a total of 7 courses of chemotherapy with amrubicin (13 months after initial treatment). Carboplatin/etoposide was used as third-line chemotherapy. No severe side effects associated with irinotecan/cisplatin, amrubicin, and carboplatin/ etoposide were observed. The patient died of disease progression 27 months following the initial treatment. No intrapelvic recurrence was detected by pelvic examination or by standard imaging modalities including transvaginal ultrasonography, CT, and MRI, throughout the postoperative course.
Discussion
Small cell carcinoma of the uterine cervix is associated with a poor prognosis even after the administration of multimodal therapy.8,9,11,12 This rare disease tends toward rapid extrapelvic distant metastasis to areas such as the lung, liver, brain, bone and lymph nodes, resulting in a shorter overall survival time than that seen in patients with other histopathological subtypes of cervical carcinoma.1,2,4,9,11,12 Hoskins
The treatment of small cell carcinoma of the uterine cervix is essentially extrapolated from that for small cell lung cancer. However, the optimal initial therapeutic approach to small cell carcinoma of the uterine cervix in particular has not yet been clearly defined. Locoregional treatment alone has been reported as insufficient, in most patients, to control both the local and distant aggressiveness of the disease.1,11,12 It has been suggested that small cell carcinoma of the uterine cervix should be treated by multidisciplinary therapy, including surgery, chemotherapy, and radiotherapy.2–4,6,11–13 Patients receiving initial concurrent chemoradiotherapy with surgery may fare better, although the evidence remains inconclusive.4,7,11,12 Locoregional recurrence outside irradiated fields is frequently observed in patients treated by radiotherapy. 8 Therefore, additional treatment strategy for locoregional disease control is necessary. Recently, neoadjuvant or postoperative chemotherapy has been used in an attempt to improve the survival of patients with small cell carcinoma of the uterine cervix.2,3,13,15
Some trials have revealed improved oncologic outcomes when patients are treated with similar regimens to those used for small cell cancers of the lung.
7
Hoskins
Several combination chemotherapy regimens have been demonstrated to achieve better survival for patients primarily treated with surgery for small cell carcinoma of the uterine cervix.1,3,6 Most frequently used regimens include etoposide/cisplatin,2–4 and, carboplatin/ paclitaxel. 7 However, the aggressiveness and poor prognosis of small cell carcinoma of the uterine cervix suggest the need for novel chemotherapy regimens. As demonstrated in the present report, irinotecan/cisplatin and amrubicin, which are currently used for the small cell lung cancer,16–18 are considered to be effective for small cell carcinoma of the uterine cervix. Favorable results have been reported in patients with small cell carcinoma of the uterine cervix who received concurrent chemoradiation followed by adjuvant chemotherapy,7,8, 11,12 while other studies have reported that radical surgery is an important component in the multimodal treatment of small cell carcinoma of the uterine cervix.5,14 In cases involving adjuvant chemotherapy following surgery, the delay in systemic treatment resulting from even a short postsurgical recovery period might place a patient at risk for metastatic spread. For this reason, Lewandowski and Copeland 13 proposed the use of neoadjuvant chemotherapy followed by surgery and or radiation therapy for the treatment of neuroendocrine tumors of the cervix. It has also been recommended neoadjuvant chemotherapy for patients with large-sized tumors, which is expected to enhance the resectability of the bulky tumors and thereby improve outcomes.5–7,14
In conclusion, we reported here a case of advanced-stage small cell carcinoma of the uterine cervix treated with neoadjuvant chemotherapy followed by radical surgery and adjuvant chemotherapy, which yielded successful locoregional disease control. Although to date there have been no randomized clinical trials to evaluate this approach, our multimodal treatment strategy is suggested to be an important component for this aggressive disease.