
Abstract
Primary pancreatic small cell carcinoma (SCC) is rare, with just over 30 cases reported in the literature. Only 7 of these patients underwent surgical resection with a median survival of 6 months. Prognosis of SCC is therefore considered to be poor, and the role of adjuvant therapy is uncertain. Here we report two institutions’ experience with resectable pancreatic SCC. Six patients with pancreatic SCC treated at the Johns Hopkins Hospital (4 patients) and the Mayo Clinic (2 patients) were identified from prospectively collected pancreatic cancer databases and re-reviewed by pathology. All six patients underwent a pancreaticoduodenectomy. Clinicopathologic data were analyzed, and the literature on pancreatic SCC was reviewed. Median age at diagnosis was 50 years (range 27–60). All six tumors arose in the head of the pancreas. Median tumor size was 3 cm, and all cases had positive lymph nodes except for one patient who only had five nodes sampled. There were no perioperative deaths and three patients had at least one postoperative complication. All six patients received adjuvant therapy, five of whom were given combined modality treatment with radiation, cisplatin, and etoposide. Median survival was 20 months with a range of 9–173 months. The patient who lived for 9 months received chemotherapy only, while the patient who lived for 173 months was given chemoradiation with cisplatin and etoposide and represents the longest reported survival time from pancreatic SCC to date. Pancreatic SCC is an extremely rare form of cancer with a poor prognosis. Patients in this surgical series showed favorable survival rates when compared to prior reports of both resected and unresectable SCC. Cisplatin and etoposide appears to be the preferred chemotherapy regimen, although its efficacy remains uncertain, as does the role of combined modality treatment with radiation.
Introduction
More than 42,000 cases of pancreatic cancer occur in the United States each year. The most common forms of pancreatic cancer in descending order of frequency are ductal adenocarcinoma, intraductal papillary mucinous neoplasms with invasive cancer, and well-differentiated neuroendocrine tumors. However, more than a dozen other rarer types have been described, 1 many of which are biologically aggressive and present at an advanced stage. As imaging technology, chemotherapy, and access to health care improve, surgery will likely take on a more important role in the management of these rarer pancreatic cancer subtypes. Institutional series, reviews, and meta-analyses of these cancers are necessary so that surgeons and pathologists can identify them when encountered and render the appropriate diagnosis, prognosis, and treatment.
Small cell carcinoma (SCC) of the pancreas is an example of a rare pancreatic cancer, with just over 30 cases described in the literature. Most of the SCC literature to date focuses on small cell lung carcinoma (SCLC), which comprises 25% of all lung cancers. 2 While 96% of small cell carcinomas originate in the lung, 2 small cell carcinomas can arise from multiple sites in the body, including the gastrointestinal system, larynx, pharynx, paranasal sinuses, uterus, cervix, ovaries, bladder, and prostate. Furthermore periampullary small cell carcinomas have been described in the duodenum, 3 bile duct,4–6 ampulla of Vater, 7 and pancreas. 2 Historically considered an exocrine tumor, pancreatic SCC is now classified as a neuroendocrine carcinoma that can be distinguished from more common lower-grade pancreatic neuroendocrine tumors by its high mitotic rate (>20 mitoses per 10 high power fields), infiltrative pattern of growth, minimal cytoplasm, finely granular cytoplasm, and nuclear molding.2,8 We present the experience of two institutions, the Johns Hopkins Hospital and the Mayo Clinic, with resectable small cell carcinoma of the pancreas and provide an updated review of the literature, with a particular emphasis on resected pancreatic SCC.
Materials and Methods
This study was approved by the Institutional Review Boards of the Johns Hopkins Hospital, Baltimore and the Mayo Clinic, Rochester. At the Johns Hopkins Hospital, a prospectively collected pancreaticoduodenectomy database and the Department of Pathology patient database were queried for all surgical cases of pancreatic SCC. Between 1970 and 2007, of all patients undergoing a pancreaticoduodenectomy, four patients were identified with pancreatic SCC, representing 0.3% of all operable pancreatic cancer cases. At the Mayo Clinic, a prospectively collected database of all cases of pancreatic neoplasms was maintained from 1975 to 2005 through the Mayo Clinic Tumor Registry and updated through a retrospective chart review. There were 3,694 patients with ductal adenocarcinoma during this period, and 64 patients with other rare tumor types. Only two patients with resected pancreatic SCC were identified, representing 0.0005% of all pancreatic cancer cases seen at the Mayo Clinic. Baseline demographic, clinicopathologic, treatment, and long-term survival data were reviewed for each patient.
Results
There were six patients identified with SCC of the pancreas. Three of the six patients were male, and three of the patients were known smokers. Median age at diagnosis was 50 years (range 27–60 years). The most common presenting symptoms were abdominal pain (67%) and jaundice (67%). None of the patients died perioperatively, although three patients suffered postoperative complications, including two patients with wound infections, one of whom also experienced delayed gastric emptying, and a third patient with an intra-abdominal abscess requiring percutaneous drainage. Overall, the median length of hospital stay was 12 days (range 10–23). These data are summarized in Table 1. All six carcinomas originated in the head of the pancreas. One of the carcinomas directly extended into the duodenum, and another involved the portal vein. Median tumor diameter was 3 cm (range 3–4.5 cm). Lymph node metastases were indentified in five patients, while the sixth patient only had five lymph nodes sampled and therefore may have been understaged. This patient was also the only one of the series to have positive resection margins. Three patients had microscopic vascular or perineural invasion. The pathology data are presented in Table 2.
Postoperative data.

NR, no record.
Pathologic data.

NR, no record.
All six patients are deceased. Median survival was 20 months (range 9–173 months). All six patients received adjuvant therapy, although the precise postoperative regimen is known only for the single patient treated adjuvantly at the Johns Hopkins Hospital. As first-line therapy, this individual received combined modality chemoradiation (50 Gy/2 Gy fractions) with concurrent cisplatin and etoposide. This patient's cancer recurred in the liver seven months after surgery, and experimental palliative chemotherapy with a BCL-2 antagonist (obatoclax) and topotecan was given. Single-agent paclitaxel was used after the previous regimen was discontinued due to side effects, but disease progression continued in the liver, peritoneal cavity, and lungs. Of the remaining five patients, four received combined modality treatment with cisplatin, etoposide, and radiation therapy at other institutions. The remaining patient received neoadjuvant chemotherapy with 5-fluorouracil, adriamycin, and mitomycin, after the cancer was initially deemed locally unresectable. While this patient was found to have positive resection margins, adjuvant radiation was not given, and it is unknown whether the patient received further adjuvant chemotherapy.
Discussion
Pancreatic SCC is now widely accepted as a high grade neuroendocrine carcinoma. 9 Preoperatively, it is difficult to distinguish SCC from more common types of pancreatic cancers, because the lesions share similar clinical symptoms and features on imaging studies. Resectable pancreatic small cell carcinomas typically measure about 3 cm. On CT imaging, they are homogeneous, well-defined, hypoattenuated with minimal enhancement after intravenous contrast injection, and may be hypo- or hyperechoic on ultrasound (Figure 1).10,11 Macroscopically, lesions appear grey-white in color and often contain areas of necrosis and hemorrhage. 2 Microscopically, pancreatic SCC is indistinguishable from SCLC, consisting of sheets of discohesive, pleomorphic cells with scant cytoplasm and high mitotic activity (>20 mitoses per 10 high power fields). Apoptotic bodies and necrotic foci are usually widespread. The nuclei have hyperchromatic, finely granular chromatin and either absent or small nucleoli (Figure 2). 12 Nuclear molding is often prominent.
(A) Small cell carcinoma of the pancreas, Gross. (B) Computed tomography scan, arterial phase.
Small cell carcinoma of the pancreas, Microscopic. At low magnification (100×, A), the diffuse architecture of the tumor on the left differs from the normal exocrine pancreas on the right. Mitotic figures and apoptotic bodies are abundant enough to be recognizable at this low magnification. Higher power views (400×, B) of the tumor cells demonstrate the disorganization, pleomorphism, high nuclear to cytoplasmic ratio, and finely granular cytoplasm. As in lower magnification fields, mitoses and apoptotic figures abound.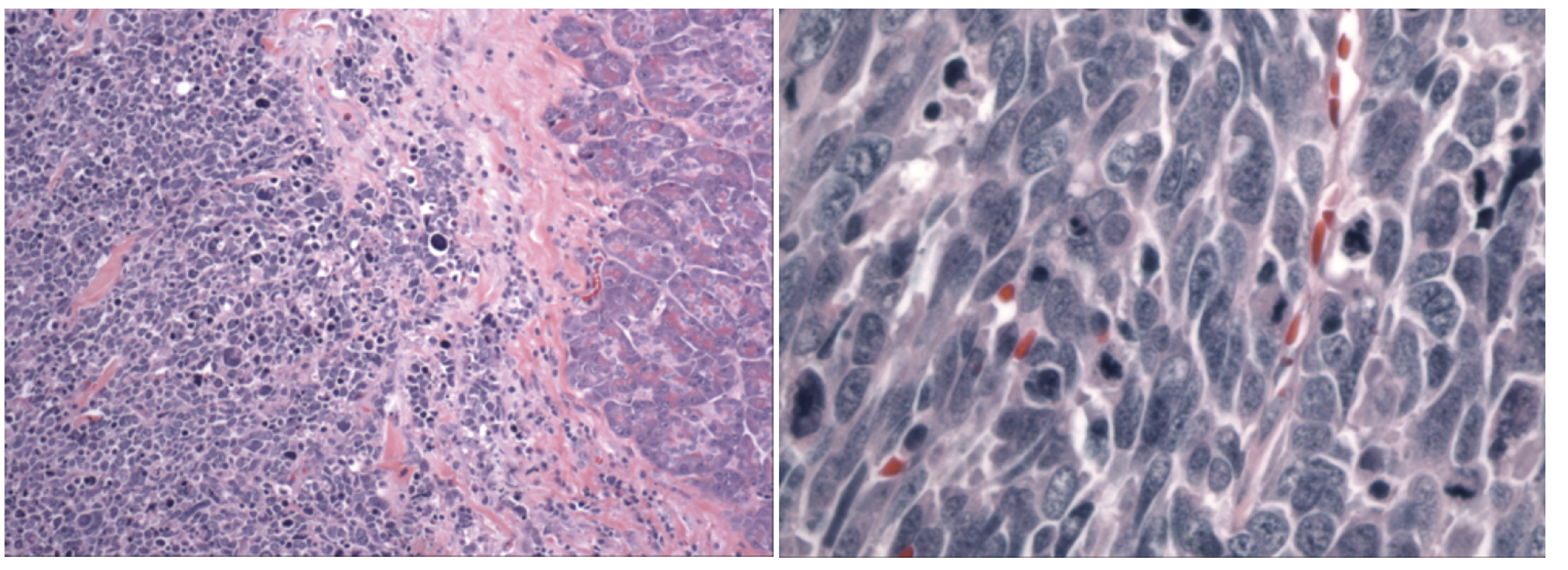
Neuroendocrine differentiation is supported by the presence of cytoplasmic membranebound granules on electron microscopy although in modern practice this workup is unnecessary as the neoplastic cells are also usually reactive to antibodies specific for neuroendocrine differentiation, such as synaptophysin, chromogranin A, and CD57.2,12 Occasionally, the neoplastic cells react with antibodies to neurofilaments. 13 Immunohisto - chemical labeling for neuron-specific enolase (NSE) has been used to characterize small cell carcinomas. Despite its high sensitivity, NSE lacks specificity as a neuroendocrine marker.13,14 In the practical work-up of SCC, immunohistochemistry is useful to discern SCC from high grade lymphoma; SCC labels with antibodies to high molecular weight cytokeratins but not with antibodies to leukocyte common antigen (CD45). Immunohistochemistry has not proven useful in distinguishing primary peri-ampullary SCC from metastatic SCLC. 15 Although a high percentage of lung primaries express thyroid transcription factor 1 (TTF-1), this marker has shown variable positivity in patients with extra-pulmonary small cell carcinoma.16–19 Furthermore, the expression of TTF-1 has not been well explored in pancreatic SCC, with only one reported negative case in the literature to date. 20 Recent studies have demonstrated that serum pro-gastrin releasing peptide (ProGRP) and serum neuron specific enolase (NSE) levels can be elevated in patients with pancreatic SCC, similar to the clinical experience with lung primaries.21,22 In fact, serum NSE levels were found to fluctuate with changes in disease burden in a at least one patient with pancreatic SCC. 22
Due to the rarity of pancreatic SCC, a pulmonary origin should be presumed in the setting of a suspicious pancreatic mass and a history of SCLC. Furthermore, any patient with a pancreatic mass that is suggestive of SCC on imaging or biopsy should be evaluated with a chest CT to rule out a lung primary. Somatostatin receptor scintigraphy (SRS) may also have a limited role in the workup of a patient with a pancreatic mass suggestive of SCC, although its value above a high quality CT scan is uncertain. The test has 90% sensitivity for detecting primary SCLC and has also been described for primary pancreatic SCC.2,23
In a 2004 comprehensive review of pancreatic SCC, Berkel et al. identified 23 cases in the literature, including one patient from the authors’ own experience. Since then, nine additional cases of pancreatic SCC have been described,21,22,24–27 wich are listed in Table 3 in a format consistent with the summary table presented in the review by Berkel et al. Missing data prevented significant analysis for several of the patients in Berkel's review, but a recent publication by Vos et al. examined a subset of the aforementioned 32 cases, focusing on patients for which adequate information was available. In this series of 23 patients, the median age was 62 years (range 37–75 years), and there was a male predominance (74%). The median tumor size was 4.2 cm, and the head of the pancreas was involved in 59% of cases. At diagnosis, disease was confined to the pancreas in only two cases. Metastatic spread to the peripancreatic lymph nodes and the liver was noted in 62% and 38% of patients, respectively. Patients receiving either systemic or local therapy showed a significantly higher median survival compared to patients treated with symptomatic management alone (6 vs. 1 month, P≤0.0001). However, the authors found no significant difference in median survival between patients receiving chemotherapy alone and patients given local treatment in addition to chemotherapy, although it should be noted that the latter group contained only three patients. Overall, median survival was just 3 months (range 0.5–50 months). 28
Recent reported cases of small cell carcinoma of the pancreas.

RT, external beam radiation; Car, carboplatin; Cis, cisplatin; Et, etoposide; 5FU, 5-fluorouracil.
The majority of patients reported to date with pancreatic SCC did not have their tumors resected. Table 4 lists the seven previously reported patients who have had a pancreatic resection for SCC, along with the six patients from the present series.22,24,25,29–32. Three patients received adjuvant chemotherapy with cisplatin and etoposide, two received adjuvant radiation, and two were treated with surgery alone. No patient received combined adjuvant chemotherapy and radiation. The median survival was 6 months (range 1–56 months) for these patients. The present series of surgical patients almost doubles the reported experience of resected pancreatic SCC. Interestingly, all of the tumors originated in the head of the pancreas, supporting the observation that pancreatic SCC is more common in the head than in the body or tail. 33 Five patients in the present series received combined modality adjuvant therapy using cisplatin and etopside, in conjunction with radiation. To our knowledge, this represents the first report of tri-modality therapy for pancreatic SCC.
Surgical cases of small cell carcinoma of the pancreas.

IORT, intraoperative radiation; RT, external beam radiation; Cis, cisplatin; Et, etoposide; 5FU, 5-fluorouracil; NR, no record.
Surgical management remains the standard treatment for well differentiated neuroendocrine tumors. However, the benefit of surgery for high grade neuroendocrine carcinomas has not been established. Certainly, the poor survival after surgery reported to date (6 months median survival) might lead one to question the utility of pancreatectomy for high-grade neuroendocrine carcinoma. However, in the present series, three of six patients survived more than 2 years, and two patients survived over five years. The patient who lived for 173 months represents the longest reported survival for pancreatic SCC to date. The median survival was 20 months, which is comparable to patients with resected ductal adenocarcinoma of the pancreas.(33–36) Despite the small patient size in our study, we believe that combined local and systemic treatments, such as surgery and adjuvant chemoradiotherapy, should be considered in resectable pancreatic small cell carcinoma.
Conclusions
Pancreatic SCC is an extremely rare form of pancreatic cancer and occurs primarily in the head of the pancreas. Although these carcinomas are associated with an extremely poor prognosis, survival beyond a few years is possible, as was observed in three patients in the present surgical series and two previously reported cases of resectable disease. The regimen of cisplatin, etoposide, and radiation is generally the favored treatment for pancreatic SCC. Surgery and adjuvant chemoradiation should be considered in patients with resectable small cell carcinoma of the pancreas.