
Abstract
Pineal parenchymal tumors are rare. Of the three types of pineal parenchymal tumors, pineocytomas are the least aggressive and are not known to diffusely disseminate. In this paper, we report the successful treatment of a case of pineocytoma with diffuse leptomeningeal relapse following initial stereotactic radiotherapy. A 39-year-old female presented with headaches, balance impairment, urinary incontinence, and blunted affect. A pineal mass was discovered on magnetic resonance imaging (MRI). A diagnosis of pineocytoma was established with an endoscopic pineal gland biopsy, and the patient received stereotactic radiotherapy. Ten years later, she developed diffuse leptomeningeal dissemination. The patient was then successfully treated with craniospinal radiation therapy. Leptomeningeal spread may develop as late as 10 years after initial presentation of pineocytoma. Our case demonstrates the importance of long-term follow-up of patients with pineal parenchymal tumors following radiation therapy, and the efficacy of craniospinal radiation in the treatment of leptomeningeal dissemination.
Introduction
Pineal parenchymal tumors are rare, accounting for 0.4–1% of all intracranial tumors in the United States and Europe and 2.2–8% of those in Northeast Asia.1,2 Pineal parenchymal tumors (PPT) include pineocytomas, pineal parenchymal tumors of intermediate differentiation (PPTID), and pineoblastomas. Pineocytomas typically remain localized, and the reported 5-year survival rate is 86%.3,4 There have been sparse reports of pineocytomas associated with leptomeningeal progression, but to our knowledge none have described in detail the extent, time course, and management of diffuse leptomeningeal dissemination.5,6 In this paper, we report a case of pineocytoma with leptomeningeal relapse following radiotherapy.
Case Report
Presentation
In June 1999, a 39-year-old female presented with a two year history of worsening headaches, balance impairment, urinary incontinence, and blunted affect, with a loss of interest in her usual activities. She had no visual complaints. On physical exam, pupils were equal, round and reactive to light, and extraocular movements were intact, including upward gaze, with no evidence of Parinaud's syndrome. Magnetic resonance imaging (MRI) demonstrated a heterogeneously enhancing pineal mass causing hydrocephalus (Figure 1).
T1-weighted post-contrast sagittal magnetic resonance image showing an enhancing mass in the region of the pineal gland.
Operation and diagnosis
An endoscopic pineal gland biopsy and third ventriculostomy were performed. The biopsy revealed a primary pineal neoplasm with uniform cells, round nuclei, and focal clusters of cells consistent with pineocytomatous rosettes. The final pathologic diagnosis was pineocytoma. The patient continued to experience symptoms following the third ventriculostomy, requiring placement of a ventriculoperitonal shunt. Following shunt placement, her symptoms dramatically improved.
Treatment
In October 1999, the patient underwent stereotactic radiotherapy to a total dose of 5040 cGy in 28 fractions of 180 cGy. The prescribed 90% isodose line encompassed the multi-loculated contrast-enhancing volume of the tumor with minimal additional margin. At the time of treatment planning, the target volume was 1.68 cc and measured approximately 13×15×20 mm. Daily treatment was delivered by a dedicated 6-MV linear accelerator with micromultileaf collimators (Novalis, Heimstetten, Germany). The patient was immobilized by a custom-fitted thermoplastic face mask. Treatment was performed using a single isocenter and 17 noncoplanar beams, each of which was conformed to the beam's eye view of the target by the collimator. The patient tolerated daily immobilization and treatment without acute complications.
Post-treatment course
The patient was followed with MR imaging. The enhancing region of the tumor disappeared by June 2001. By June 2007, complete resolution of the pineal mass was noted along with diffuse pachymeningeal thickening. Given the non-specific nature of this finding in an otherwise asymptomatic patient, regular follow-up was scheduled in two years.
Recurrence
In February 2009, the patient returned to clinic complaining of bilateral resting tremors and left hand numbness over the previous year, progressive low back pain and sciatica-like pain running down her left leg into her left foot for the past six months and constipation, nausea, vomiting, fatigue and saddle anesthesia increasing over the previous three weeks. She had additionally experienced a twenty-pound weight loss over the past three years. An MRI was performed which revealed mass-like enhancement of the fifth cranial nerve, widespread leptomeningeal enhancement involving the cervical, thoracic, and lumbar spine, as well as enhancement throughout the perimesencephalic cistern, interpeducular cistern, and cisterna magna (Figures 2 and 3). The imaging revealed no evidence of local relapse.
T1-weighted post-contrast axial magnetic resonance image showing leptomeningeal enhancement around the brainstem at the cervicomedullary junction.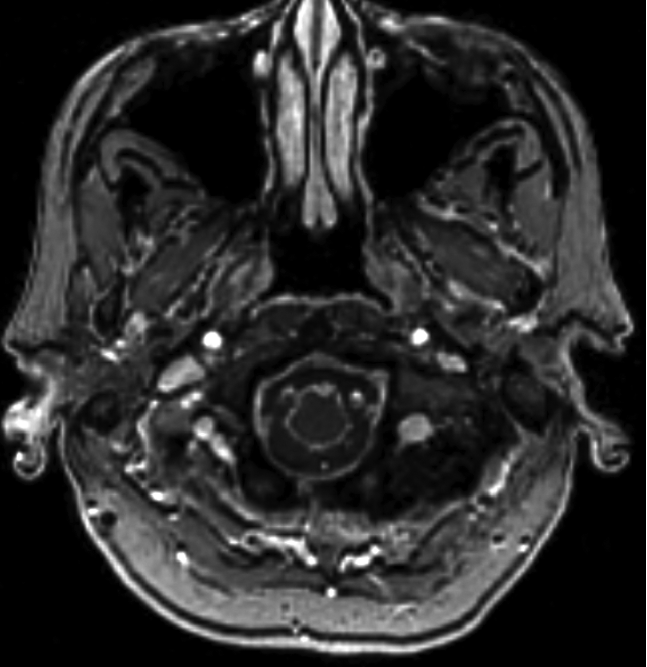
T1-weighted post-contrast axial magnetic resonance image showing nodular enlargement and enhancement of the trigeminal nerves bilaterally.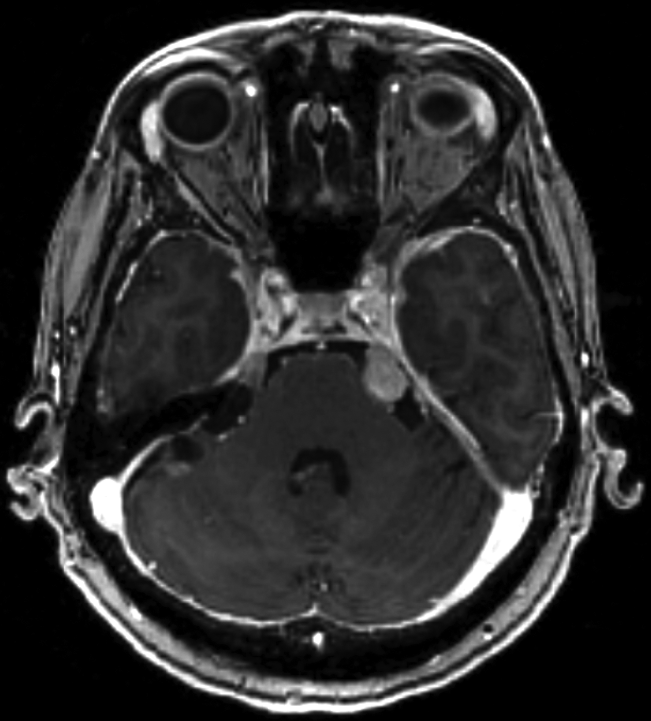
Diagnosis and treatment
Cerebrospinal fluid studies revealed atypical cells consistent with pineocytoma. There was no evidence of infection, with negligible leukocytes and negative tests for syphilis, cryptococcus, tuberculosis and other infectious etiologies. In March 2009, a left frontal craniotomy and dural biopsy were performed. The biopsy was described as pineocytoma and pineal parenchymal tumor of intermediate differentiation, WHO grade II-III. The sample did not have the histopathologic features of a pineoblastoma, according to the WHO Classification of Tumors affecting the Central Nervous System. The tumor was graded as WHO II-III in view of histologic characteristics consistent with a pineocytoma and a high Ki-67 index (10–15%). By the time the pathology from the dural biopsy was reviewed, the slides from the original biopsy were no longer available for comparison or additional staining. The patient began craniospinal radiation therapy in April 2009, receiving 24 Gy in 16 fractions to the whole brain and spine, with a boost of 26 Gy to the sacral spine.
Follow-up
By June 2009, the patient's MRI revealed decreased leptomeningeal enhancement and a decrease in the size of the trigeminal nerves. All of the patient's symptoms had resolved except for minimal residual tremor. The patient refused adjuvant chemotherapy. The patient was last followed up more than 24 months after completion of craniospinal radiation. At that time, she remained tumor free and had a normal neurologic examination, except for minimal tremor. By 24 months post-treatment, we would expect any late neurologic side effects to have already emerged. These late side effects would likely consist of a vertical gaze palsy secondary to radiation necrosis and edema in the pineal region, which received the highest radiation dose 50.4+24 Gy. This patient is unlikely to develop any late neurologic side effects in the future.
Discussion
PPT are classified into three types: pineocytomas, PPTID, and pineoblastomas. Pineocytomas and pineoblastomas each account for approximately 45% of pineal parenchymal tumors. 3 PPTID are tumors that lie on the spectrum between pineocytomas and pineoblastomas, and account for approximately 10% of pineal parenchymal tumors. 3 The reported survival rates of these tumors vary from 86% 5-year-survival for pineocytomas to projected 1-year, 3-year, and 5-year survival rates of 88%, 78%, and 58%, respectively for all other pineal parenchymal tumors. 7
Diffuse leptomeningeal enhancement has been reported in association with disseminated malignancies as well as benign etiologies including cerebrospinal fluid pressure changes and autoimmune, infectious, inflammatory, and genetic disorders.8–13 In our case, diffuse leptomeningeal enhancement was initially thought to be due to infection, since pineocytoma has a low risk of dissemination to the leptomeninges and this type of diffuse dissemination had not yet been reported in the literature.
D'Andrea et al. reported leptomeningeal dissemination in three of six children with pineocytomas, although it is unclear whether the dissemination was focal or widespread. 6 Additionally, the authors did not use the designation PPTID. They classified pineal tumors only as pineocytoma or papillary pineocytoma. 6 It is, therefore, possible that some of their pineocytomas were actually PPTID, a potentially more aggressive tumor. Two retrospective studies of pineal tumors reported by Schild et al. found that of the PPT, spinal dissemination was associated with mixed PPT and PPTID but not pineocytomas.4,7 If D'Andrea et al. had classified their cases into pineocytomas and mixed PPT or PPTID, it is possible that they might have found leptomeningeal dissemination to be associated with mixed PPT and PPTID and not pure pineocytoma.
Leptomeningeal dissemination in our case could potentially be a result of dedifferentiation of an initial pineocytoma into a more aggressive PPTID. In our case, however, this scenario is less likely given that a dedifferentiated tumor would not have the histological characteristics of a pineocytoma.
It has been noted by Hasegawa et al. that an extensive amount of tissue is necessary to diagnose a PPTID, as opposed to a pineocytoma, and often stereotactic sampling or endoscopic sampling (as was used to obtain the first biopsy specimen in this case) are not sufficient. 5 In our case, subsequent dural biopsy revealed PPTID. It is possible that the original tumor had regions of PPTID which were missed in the biopsy, resulting in an unappreciated risk for leptomeningeal dissemination. A final possibility is that the endoscopic biopsy seeded the leptomeninges or served as a trigger for later dissemination.
Leptomeningeal spread, although rare, may develop as late as 10 years after initial presentation of pineocytoma. The natural history of our case demonstrates the importance of long-term follow-up of patients with pineal tumors following radiation therapy treatment. As is demonstrated by our case, a patient that develops leptomeningeal dissemination from a pineal parenchymal tumor can be effectively treated with whole brain and spine radiation therapy.