
Abstract
Plexiform neurofibroma of the submandibular gland is an extremely rare tumor. Herein, we report a case of plexiform neurofibroma in a patient with a von Recklinghausen's disease (NF-1) who presented with a submandibular mass mimicking a submandibular gland tumor. Complete surgical excision provides the best treatment and final diagnosis. A neurofibroma should be considered in the differential diagnosis for submandibular mass.
Introduction
Plexiform neurofibroma is a benign peripheral nerve sheath tumor that surrounds multiple nervous fascicles. 1 Neurofibromas may occur as part of the syndrome of neurofibromatosis (commonest), solitary neurofibromas, or multiple neurofibromas without von Recklinghausen's disease (NF-1).2,3 The plexiform neurofibromas of the submandibular gland are extremely rare.4–8 To date only five cases had been reported in the literature (Table 1) and only one case was not associated with NF-1. 5 Herein, we report a case of submandibular gland plexiform neurofibroma in a patient with NF-1.
Literature review of submandibular gland plexiform neurofibroma.

NA, Not available; −ve, negative; +ve: positive; Y, year; FNA, fine needle aspiration cytology; NF1, von Recklinghausen's disease.
A 17-year-old male presented with painless left submandibular mass of five years duration. The mass became enlarged and painful two years prior to his presentation. He had no other relevant symptoms. Both his twin and father have NF-1. A physical examination revealed a non-tender 4×5 cm mass in the left submandibular region, firm in consistency, not attached to the skin and without hypoglossal or lingual nerve involvement. On systemic examination showed, signs of NF-1, multiple cutaneous neurofibroma and cafè-au-lait spots over the body (Figure 1A, 1B and 1C). 9 An investigation of complete blood count and erythrocytes sedmentation rate (ESR) were within normal limits. The ultrasound of the left submandibular region showed submandibular complex mass with heterogeneous echogenicity ill defined border. The computer tomography (CT) scan of the neck revealed heterogeneous mass in the left submandibular gland (Figure 2). The MRI T2-weighted image with contrast showed a mass with diffuse heterogeneous enhancement in the left submandibular gland (Figure 3A and 3B). Fine needle aspiration cytology showed some clusters of acininc cells but no malignant cell. Preoperative diagnosis was benign submandibular gland tumor. The left submandibular gland excision was performed. The origin of this tumor was not obvious at surgery, though the hypoglossal and lingual nerves were intact. The tumor was thought to have originated from the secreting nerve. The patient had an uneventful postoperative period. Gross examination revealed a lobulated, convoluted firm in consistency lesion. It was heterogeneous, glistening, graywhite tumor. Histopathological examination showed elongated, spindly cells with wavy nuclei and normal glandular tissue at periphery (Figures 4A and 4B). Immunohistochernical studies showed positive staining of anti-S100 protein (Figure 4C), bordered by faintly epithelial membrane antigen (EMA). Six months follow up after the left submandibular gland excision was satisfactory with no local recurrence.
Photograph showed left ankle cutaneous neurofibroma (A), right forearm cutaneous neurofibroma (B), and Cafè -au-lait spots found on the body of the patient (C).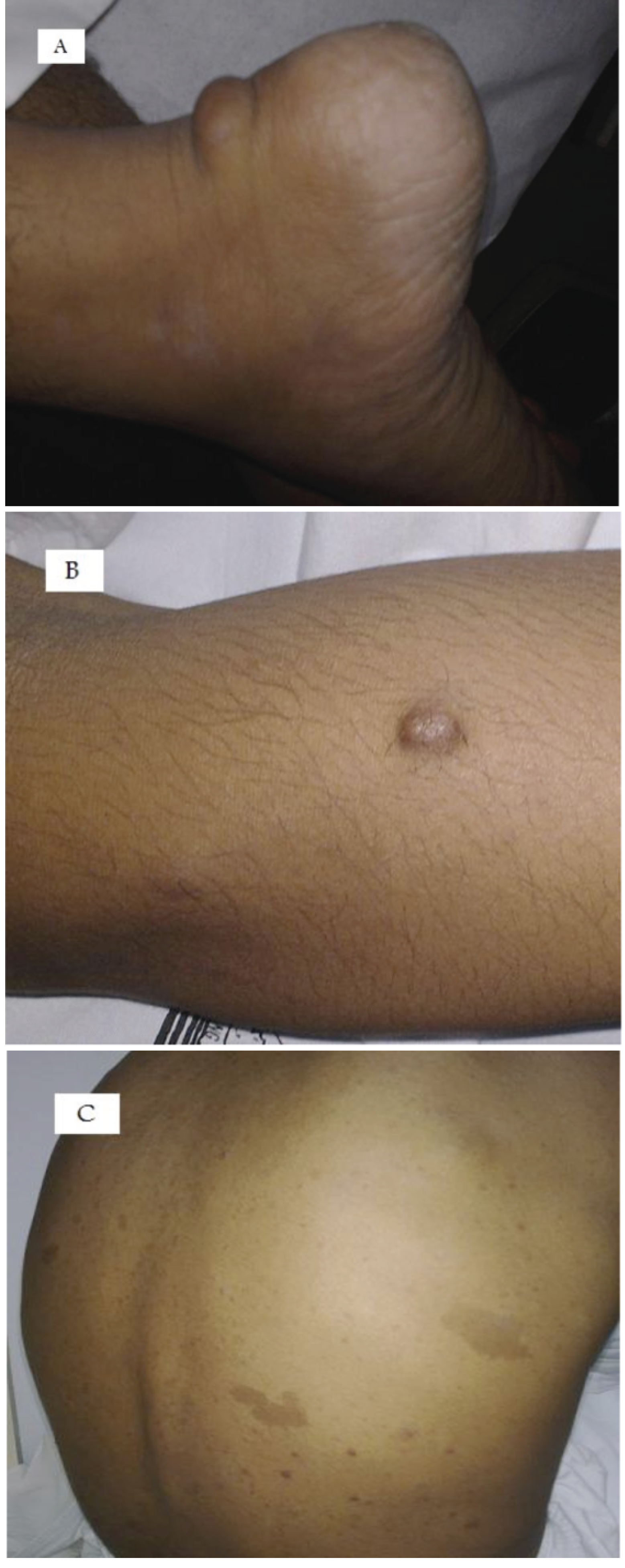
Axial contrast-enhanced computer tomography view demonstrating the heterogeneous mass of the left submandibular gland.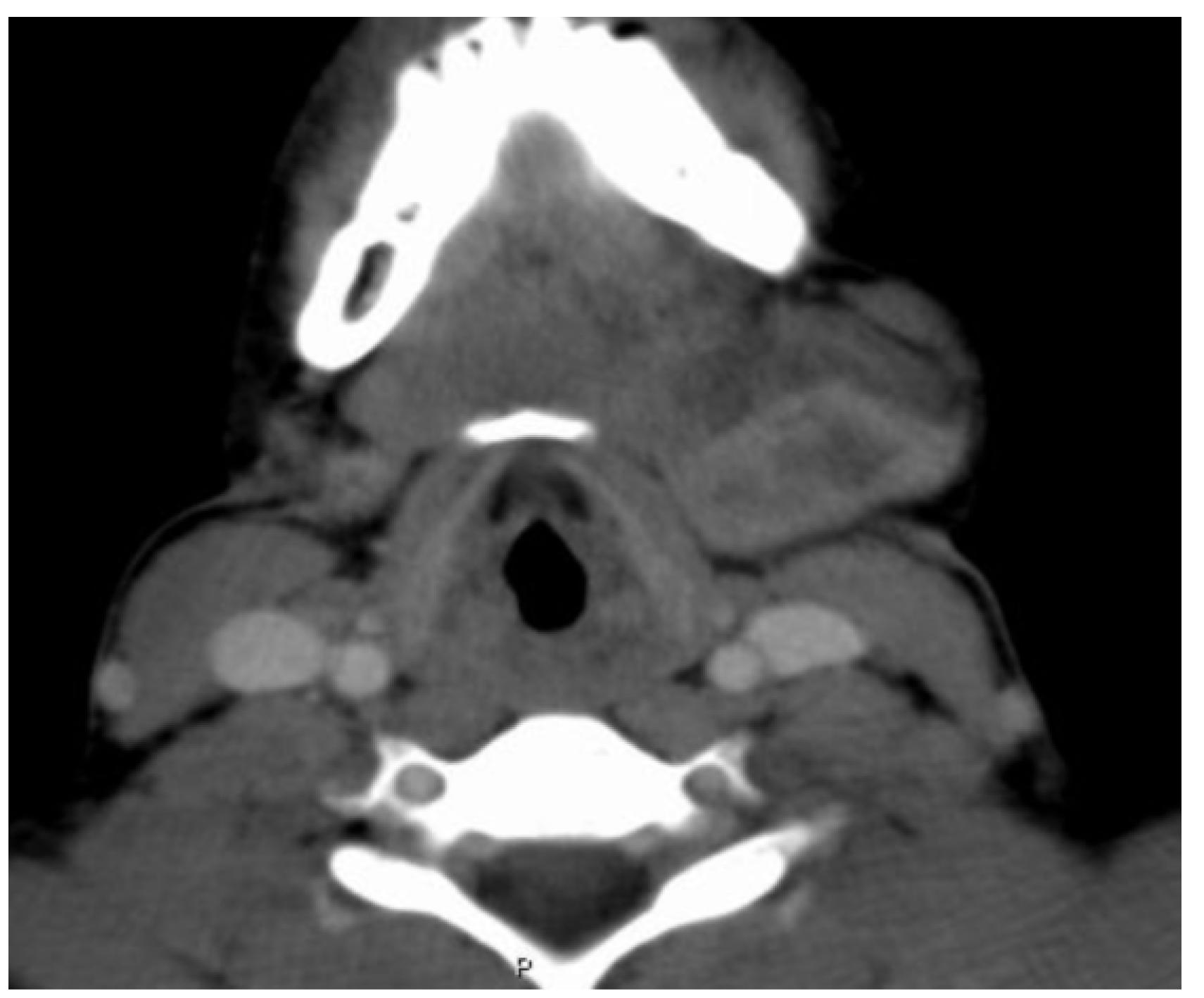
The MRI T-2 weighted image with contrast (A. Axial & B. Coronal view) showed a mass with diffuse heterogeneous enhancement in the left submandibular gland.
Photomicrograph of the plexiform neurofibroma, Histopathological image of the plexiform neurofibroma along with normal glandular tissue (Hematoxylin-Eosin stain) (A), Elongated, spindly cells with wavy nuclei (Hematoxylin-Eosin stain) (B), Immuno-positive staining for the S-100 protein (C).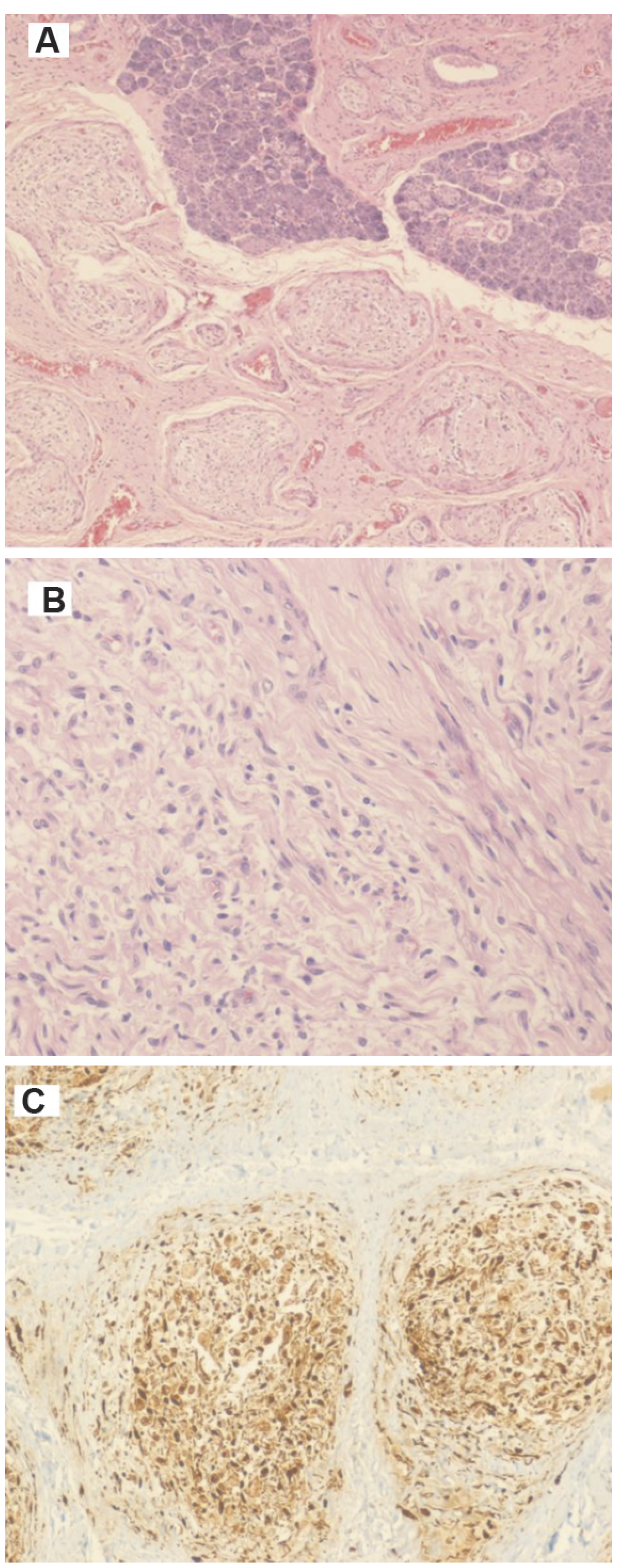
Discussion
The neurofibroma is a benign tumor of neural origin comprise all elements of the peripheral nerve (i.e. axons, Schwann cells and fibroblasts).10,11 Several forms had been described: cutaneous neurofibromas (both localized and diffuse types), intraneural neurofibromas (localized and plexiform), massive soft-tissue neurofibromas (diffuse and plexiform), and visceral neurofibromas (solitary or multiple) and sporadic or associated with NF-1.12,13 Plexiform neurofibromas are slow growing, painless and locally infiltrative tumors. 14 Although plexiform neurofibromas appear as benign, they have a 2–5% potential for malignant transformation.15,16 Most frequently occur as a component of neurofibromatosis, though they can also occur isolated without any neurofibromatosis symptoms but they are extremely rare.17,18 Mostly occur in the head and neck region because this area is richly innervated. 19 They are uncommon tumors of the salivary glands only 0.4% of salivary gland tumors. 20 They represent 14% of all benign mesenchymal tumors and 10% of non-epithelial salivary gland tumors.20,21 Most often had been described in the parotid gland. 8 The diagnosis of submandibular gland plexiform neurofibroma in all reported cases were based on histopathological examination.4–8 The diagnostic yield of FNAC appears to be rather low. Computer tomography scan and MR imaging of plexiform neurofibroma may show multilobulated masses that may appear as a bag of worm. 8 The computer tomography imaging features could be extremely helpful to the clinician in appropriately advising the patients, planning surgery and for follow-up. 8 Distinguishing between isolated neurofibroma and those associated with NF-1 is important because the treatment and prognosis different. Neurofibromas associated with NF-1 are likely to recur or undergo malignant transformation.10,22,23 The current treatment of plexiform neurofibroma involves surgery.22,24,25 These tumors are nonradiosensitive and limited benefit had been observed with chemotherapy. 26 The recurrence is seen in as many as 20% of the patients with a plexiform neurofibroma after complete resection and increases to 44% with subtotal resection.8,27
Conclusions
We have reported an extremely rare case of plexiform neurofibroma in submandibular gland. Although plexiform neurofibroma tumors have a neurogenic rather than a salivary gland origin, one must consider this kind of tumors and it is essential to monitor patients with NF-1 periodically for the possibility of recurrence and malignant transformations.
Footnotes
Acknowledgement:
we wish to express our thanks to Dr Amani Mohammed for her contribution and participation in the preparation of the manuscript.