
Abstract
Neurofibromatosis type 1, also called von Recklinghausen’s disease, is a hereditary congenital disorder that affects tissues of neuroectodermal or mesodermal origin. This disease has various manifestations, including pigmented skin lesions, cutaneous neurofibromas, skeletal abnormalities, and tumors of the central/peripheral nervous and gastrointestinal systems, and vascular abnormalities. Because of vasculopathy, part of the vessel wall may be replaced by neurofibromatosis tissue. Involvement of the internal thoracic artery is, however, extremely rare. Off-pump coronary artery bypass grafting using the left internal thoracic artery was performed for coronary arterial disease in a patient with neurofibromatosis, and the residual left internal thoracic artery vessel pathology was investigated. The left internal thoracic artery vessel showed intimal proliferation, medial thinning, and fragmentation of elastic tissue. However, these findings were not typical for von Recklinghausen’s neurofibromatosis. Internal thoracic artery graft selection was feasible for coronary artery bypass grafting in a patient with neurofibromatosis type 1.
Keywords
Introduction
Abnormal growth of neuroectodermal tumors in the peripheral nervous system is a hallmark of neurofibromatosis type 1 (NF-1), also called von Recklinghausen’s disease, an autosomal dominant disorder with variable penetrance. 1 Pigmented skin lesions, cutaneous neurofibromas, skeletal abnormalities, and tumors of the central/peripheral nervous and gastrointestinal systems, and vascular abnormalities are the predominant clinical manifestations of this disease. Vasculopathy can occur in NF-1 patients involving the aorta, carotid arteries, vertebral arteries, thyrocervical trunk, and celiac and mesenteric arteries. 2 As a result of this vasculopathy, neurofibromatosis tissue may replace part of the vessel wall. However, the internal thoracic artery is extremely rarely involved. In the present case, an NF-1 patient underwent off-pump coronary artery bypass grafting for coronary arterial disease using the left internal thoracic artery (LITA), and pathological examination was performed to determine whether the residual LITA vessel can be used for off-pump coronary artery bypass grafting (CABG) in NF-1 patients.
Case report
A 45-year-old woman who had been diagnosed with NF-1 several years earlier presented with exertional chest discomfort. On examination, multiple café au lait skin macules and subcutaneous neurofibromas were seen (Figure 1).

The patient has multiple cutaneous neurofibromas on the trunk.
Her past history included insulin-dependent diabetes mellitus, hyperlipidemia, hypertension, cerebral infarction, and Cushing’s syndrome. There were no significant abnormalities on chest X-ray, and the laboratory examinations were within normal limits. A negative T pattern was seen in leads V1 to V6 on electrocardiography, while echocardiography showed inferior wall hypokinesis, a decreased left ventricular ejection fraction (67%), and no valvular pathology.
On coronary angiography, there was 90% stenosis of the right coronary artery (RCA) 2, in addition to 99% stenosis of the left anterior descending artery (LAD) 7 and left circumflex artery (LCx) 14. All lesions showed no aneurysmal changes, only stenosis. Surgical revascularization (off-pump CABG) was performed. Under general anesthesia, the LITA was harvested via a median sternotomy in a completely skeletonized fashion using a harmonic scalpel (Ethicon Endo-Surgery, Cincinnati, OH, USA). The LITA was anastomosed to the LAD. Subsequently, a saphenous vein graft (SVG) was anastomosed sequentially from the ascending aorta to the LCx 14 and the RCA 4AV. All arterial vessels were very fragile, including the LITA, so careful attention was needed to avoid surgical injury. The patient had an uneventful postoperative course. On follow-up coronary computed tomography performed 1 month after CABG, the grafts were patent, and the native coronary artery or LITA graft and SVG showed no suspicious changes (Figure 2).

Image of 3D computed tomography demonstrating the LITA and SVG.
The residual LITA vessel pathology in this patient included intimal proliferation, medial thinning, and fragmentation of elastic tissue (Figure 3). However, immunohistochemical analysis of the proliferating cells was negative for antibodies against S-100 protein (immunostaining for neurofilaments; Figure 4). This vessel had no neurofibromatosis tissue. These findings demonstrated and confirmed that this patient’s internal thoracic artery was not typical for von Recklinghausen’s neurofibromatosis. Furthermore, no arteriosclerotic lesions (calcification, cholesterin deposition, lipid-engorged macrophages, and so on) were seen.
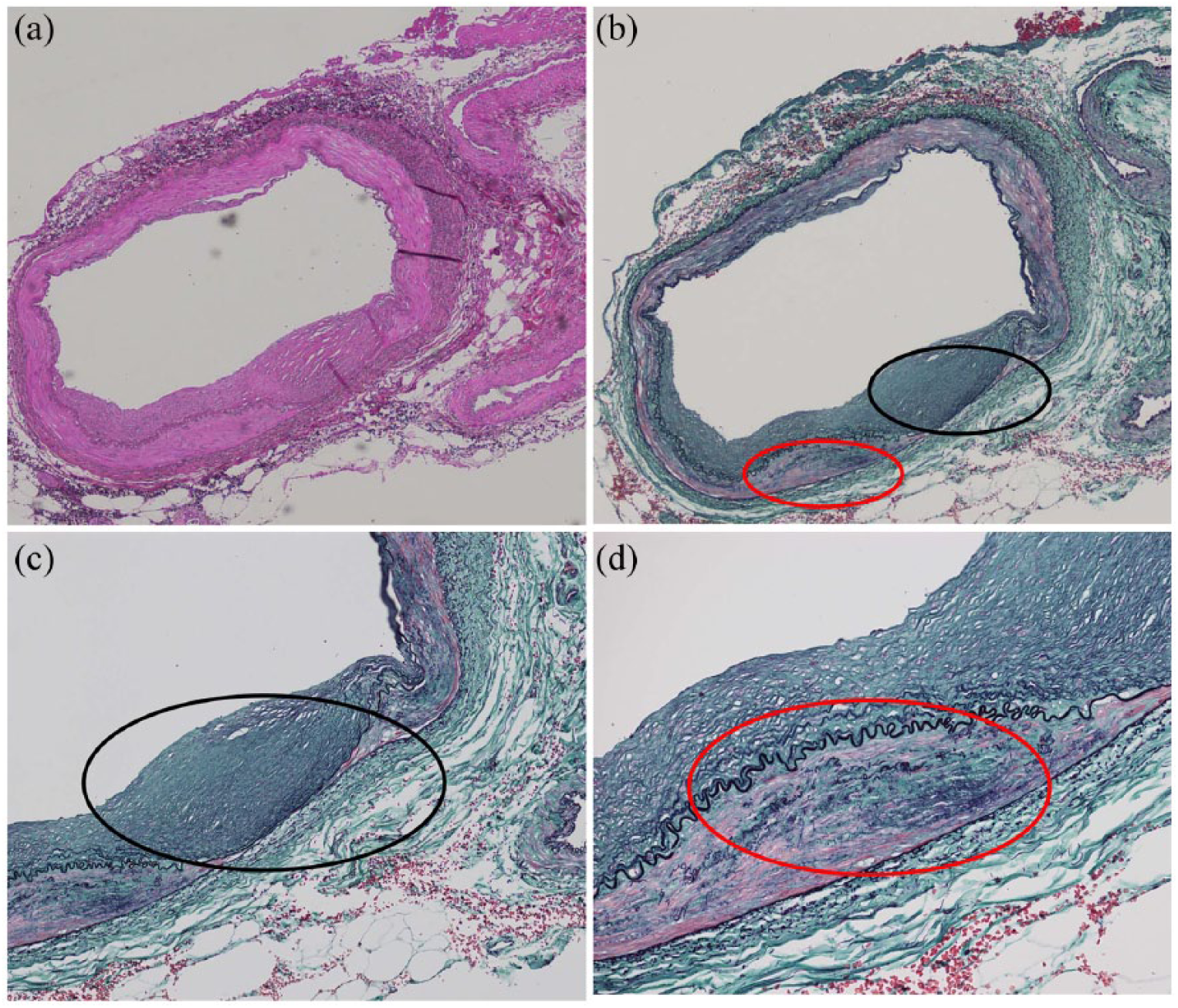
Pathological examination of the internal thoracic arterial wall showing (a) hematoxylin and eosin stain; (b) Elastica Masson stain; (c) extended image, showing thinning of media and proliferation of intima (black circle); and (d) extended image, showing fragmentation of elastic tissue (red circle).
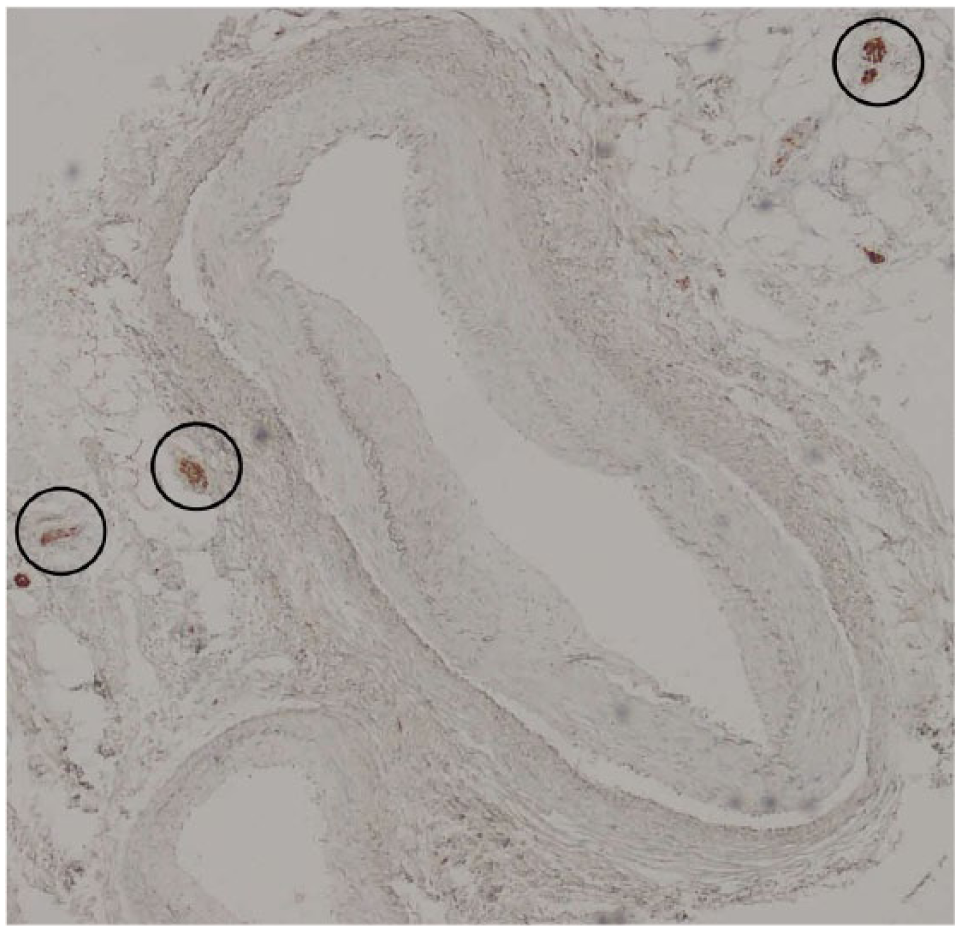
Immunohistochemical analysis for antibodies against S-100 protein (immunostaining for neurofilaments). Normal fibroma diffused in connective tissue becomes positive (black circle), but there are no positive cells in the internal thoracic arterial wall.
Discussion
Dominguez et al. reported that the incidence of vascular lesions in patients with NF-1 was only 3.6%, the lesions were mostly vascular stenosis and aneurysms, and such patients had a high mortality. 3 Vascular lesions include stenosis, occlusions, aneurysms, arteriovenous malformations, and fistulae. 4 In a study by Lin et al., the prevalence of cardiovascular abnormalities among 2322 participants in the National Neurofibromatosis Foundation database was 2%, with peripheral artery abnormalities in only 16 patients (0.7%), including renal artery stenosis in 9 (0.4%). 5 The most commonly affected vessels in NF-1 patients are the renal arteries. 6 Involvement of the subclavian or intercostal arteries is listed among the vascular manifestations of neurofibromatosis. However, involvement of other arteries, including the phrenic artery, the thyrocervical trunk, and the left vertebral artery arising directly from the aorta, has also been reported. 7 Even though the internal thoracic artery is considered among the arteries that could be involved in NF-1, its involvement is extremely rare. 8
The mechanism of vasculopathy in NF-1 patients is unknown. Based on electron microscopic findings, Greene et al. suggested two types of vasculopathy. 9 First, intimal proliferation may be seen in large arteries, resulting in stenosis, medial thinning, and fragmentation of elastic tissue, which may cause aneurysm formation. In these vessels, neurofibromatosis tissue may be present.
Second, in small arteries, smooth muscle aggregates may be seen within the intima, causing luminal narrowing. In the present case, the LITA vessel pathology included intimal proliferation, medial thinning, and fragmentation of elastic tissue, but immunohistochemical analysis of the proliferating cells was negative for antibodies against S-100 protein and neurofilaments. This vessel had no neurofibromatosis tissue. Since it was not possible to examine the LITA graft pathologically, whether there was neurofibromatosis tissue in the vessel could not be ascertained. Furthermore, there were no arteriosclerotic lesions visible.
A previous report by Evrengul et al. 10 described conventional single-vessel CABG using the left internal mammary artery in a 17-year-old NF-1 patient. However, since tissue fragility and malignant transformation are common in this disease, Suematsu et al. 8 have strongly recommended the use of off-pump CABG, which maintains the patients’ immune function and avoids cardiopulmonary bypass-related mechanical injury. They also reported their use of off-pump bilateral internal thoracic arterial CABG in a patient with neurofibromatosis; computed tomography at 5-year follow-up showed good patency without any new aneurysmal change, stenosis, or occlusion in the coronary vasculature. 8 Though Suematsu et al.’s long-term results were good, 8 Conlon et al. 11 reported that a patient with neurofibromatosis developed spontaneous hemothorax caused by rupture of an internal thoracic artery pseudoaneurysm. Therefore, the present patient must be followed carefully to identify any possible aneurysmal change and stenosis or occlusion of the internal thoracic artery.
Conclusion
To the best of our knowledge, this is the first report of off-pump CABG using an LITA graft in a patient with neurofibromatosis in which LITA vessel pathology was investigated. Since pathological examination of the LITA graft was not possible, it is uncertain whether the vessel had neurofibromatosis tissue or atherosclerosis. The LITA was fragile, and histological changes of the remnant LITA were seen that are not usually seen in healthy LITAs, but the LITA was not typical for von Recklinghausen’s neurofibromatosis, and no arteriosclerotic lesions were observed. It is said that an ITA graft is more advantageous with respect to long-term patency than another graft. Internal thoracic artery graft selection was feasible for CABG in this patient with NF-1. We plan to follow this patient for the long term, and we believe that the information presented in this case report will benefit surgeons who may have difficulty with proper graft selection for CABG in NF-1.
Footnotes
Acknowledgements
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Our institution does not require ethical approval for reporting individual cases or case series.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written, informed consent was obtained from the patient(s) for their anonymized information to be published in this article.