
Abstract
Urothelial carcinomas have an established propensity for divergent differentiation. Most of these variant tumors are muscle invasive but not all. The response of non muscle invasive variant tumors to intravesical immunotherapy with BCG is not established in the literature, and is reported here. Between June 1995 and December 2007, 760 patients (mean age of 67.5 years) underwent transurethral resection of first time bladder tumors in our institution. Histologically variant tumors were found in 79 patients (10.4%). Of these 57 patients (72%) of them had muscle-invasive disease or extensive non-muscle invasive tumors and remaining 22 patients (28%) were treated with BCG immunotherapy. These included 7 patients with squamous differentiation, 4 with glandular, 6 with nested, 4 with micropapillary and 1 patient with sarcomatoid variant. The response of these patients to immunotherapy was compared with that of 144 patients having high-grade conventional urothelial carcinomas. Median follow-up was 46 months. The 2 and 5-year progression (muscle-invasion) free survival rates were 92% and 84.24% for patients with conventional carcinoma compared to 81.06% and 63.16% for patients with variant disease (P=0.02). The 2 and 5-year disease specific survival rates were 97% and 91.43% for patients with conventional carcinoma compared to 94.74 % and 82% for patients with variant disease (P=0.33). 5 patients (22.7%) of variant group and 13 patients (9.03%) of conventional group underwent cystectomy during follow-up (P=0.068).
Patients with non-muscle invasive variants of bladder cancers can be managed with intravesical immunotherapy if tumor is not bulky (>4 cm). Although progression to muscle invasive disease is more common than in conventional group and occurs in about 40% of the patients, life expectancy is similar to patients with conventional high-grade urothelial carcinomas provided that follow-up is meticulous.
Keywords
Introduction
Urothelial carcinomas have an established propensity for differentiation into several types of variant tumors. Most of these tumors are high-grade and muscle invasive. The morphological features of these tumors are well documented and they are often associated with poor prognosis. 1 It is still unclear however, if this is related to variant histology itself or to the high grade and stage typical to these tumors. 1 Several studies suggested that variant tumors also respond poorly to surgery, chemotherapy or radiation therapy.1–3
Although most of the variant tumors invade the muscularis propria or are very bulky (>4 cm), some of these tumors are limited to the lamina propria and can be fully resected transurethrally. Can these patients be managed with intravesical immunotherapy? In this study we compared the response to BCG immunotherapy of patients with variant tumor to patients with conventional high-grade urothelial carcinoma.
Materials and Methods
Patient population
An institutional database was retrospectively obtained from the hospital registry which contained information on 760 consecutive patients who underwent transurethral resection of bladder cancer for the first time between June 1995 and December 2007. All pathological material was reviewed by a single dedicated uro-pathologist. Pathologic staging was performed according to the TNM system and grading according to the 1973 WHO classification. 4 The study was approved by the IRB (number 207–31.10.08).
Treatment and follow-up protocol
Treatment protocol included second look resection in patients with either pT1 or G3 tumors. Patients with confirmed pT1, G3 or Tis were considered eligible for immunotherapy provided that all visible tumors were resected and second look biopsies confirmed pT0. Immunotherapy protocol included an induction course of 6 weekly (no less than 4) intravesical instillations of 81 mg Connaught BCG in 50 cc of normal saline, initiated 10–20 days following surgery. Maintenance therapy included 2–3 instillations every 3 months for one year and then every 6 months for additional 2 years. Radical cystectomy was offered to patients with disease progression to T2, to patients resistant to immunotherapy or in cases of recurrent T1G3 or Tis tumors.
Follow-up protocol included bladder biopsy after the induction course, and then cystoscopy and cytology every 3 months for 2 years and every 6 months for another 3 years. Upper tract surveillance (intravenous pyelography and more recently CT urography) was performed on initial diagnosis and then annually.
Statistical analysis
The outcome of patients with variant histology receiving BCG immunotherapy was compared to the outcome of patients with conventional high grade urothelial carcinoma treated with BCG immunotherapy. Continuous variables were compared using t-test and categorical variables with Fischer's exact test and chi square tests. Survival analysis was done using the Kaplan-Meier method. A p-value <0.05 was considered significant. Statistical analysis was done using the JMP software (SAS Cary, NC, USA).
Results
Study cohort comprised of 760 patients (mean age 67.5 years, S.D. 12.7 years), including 622 men and 138 women. Tumor staging according to specimens obtained at transurethral resection were: stage Ta in 478 patients (62.9%), stage T1 in 157 patients (20.6%), and muscle-invasive disease (stage >T2) in 112 patients (14.7%). Grading according to the WHO, 1973 system showed: grade 1 tumor in 166 patients (21.8%), grade 2 in 276 (36.3%) and grade 3 in 318 (41.8%). Bladder carcinoma in situ (either pure or concomitant) was found in 137 cases (18%). Histological variants of urothelial carcinoma were found in 79 patients (10.4%), and included: squamous differentiation in 22 patients (27.85%), nested in 20 patients (25.32%), micropapillary in 13 (16.45%), sarcomatoid in 15 patients (19%) and glandular in 9 patients (11.39%). Most of the patients with variant tumors had muscle invasive disease or a bulky tumor (>4 cm) that could not be entirely removed transurethrally. However, in 22 patients, tumor was non muscle-invasive and was fully resectable as confirmed on second look TURBT (Table 1). These patients received adjuvant intravesical BCG immunotherapy. Among these patients were: 7 patients with squamous differentiation, 6 with nested, 4 with glandular, 4 with micropapillary and 1 patient with sarcomatoid variant (Figure 1).
Demographics of the variant histology, prognosis and outcome.
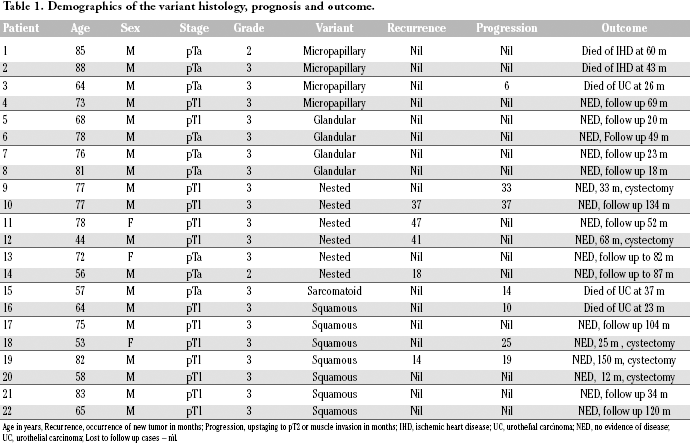
Age in years, Recurrence, occurrence of new tumor in months; Progression, upstaging to pT2 or muscle invasion in months; IHD, ischemic heart disease; UC, urothelial carcinoma; NED, no evidence of disease; UC, urothelial carcinoma; Lost to follow up cases – nil.
Photos of urothelial carcinoma histological variants not invading the detrusor muscle (H&E, ×100). (A) glandular variant (case 6), (B) micropapillary variant (case 3), (C) nested variant (case 13), (D) Squamous variant (case 17).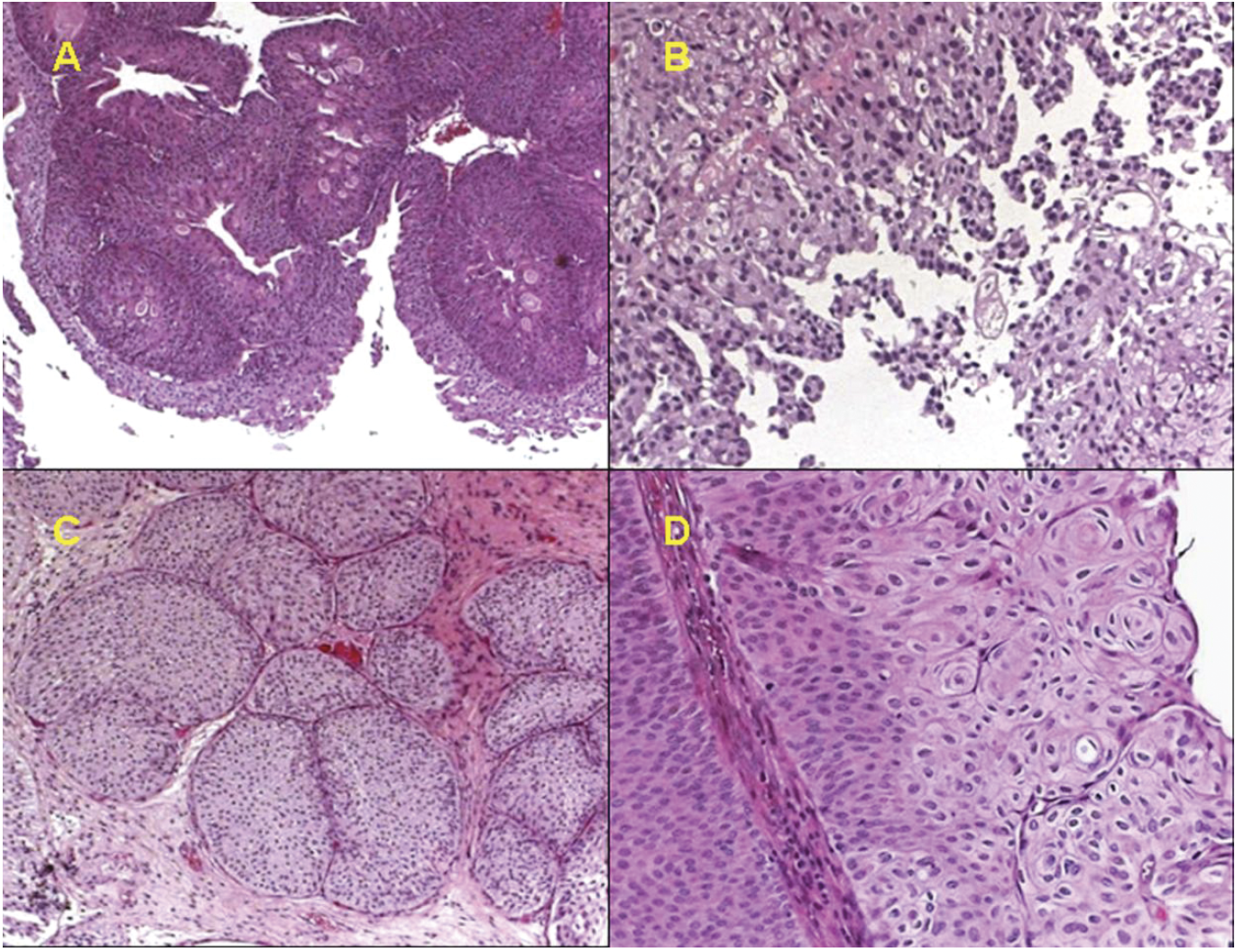
The outcome of patients with variant histology receiving BCG immunotherapy was compared to the outcome of 144 patients with conventional high grade urothelial carcinoma that were treated with BCG immunotherapy (Table 2 and Figure 2). The groups were similar in age, gender, stage distribution and follow-up length. The 2 and 5 year recurrence free survival rates were 79.56% and 71.74% with conventional carcinoma compared to 87.84% and 69.18% for the variant disease (P=0.68). The 2 and 5-year progression (muscle-invasion) free survival rates were 92% and 84.24% for patients with conventional carcinoma compared to 81.06% and 63.16% for patients with variant disease (P=0.02). Median time of progress to muscle-invasive disease was significantly shorter in the patients with variant disease (19.8 vs 56 months, P=0001). A total of 5/22 (22.7%) patients of the variant group and 13/144 (9.03%) of conventional group underwent cystectomy (P=0.068) during the course of disease follow-up. Among the variant group a total of 7 patients had progression of disease. Of these, 3 underwent cystectomy and all 3 are surviving. Of the remaining 4, two patients received chemoradiation and among these 4, only one is surviving and is under followup. In the conventional group, a total of 18 patients had progression of disease. Of these, 9 patients underwent cystectomy and 6 of them are surviving. Whereas in the non cystectomy group (9patients), two received chemoradiation and 3 patients are surviving.
Comparison of demographics with important events between the variant and conventional histologies.

Kaplan-Meier curves for (A) Recurrence free survival (P=0.6762). (B) Progression (to stage =>T2) free survival (P=0.02). (C) Disease-specific survival (P=0.3378).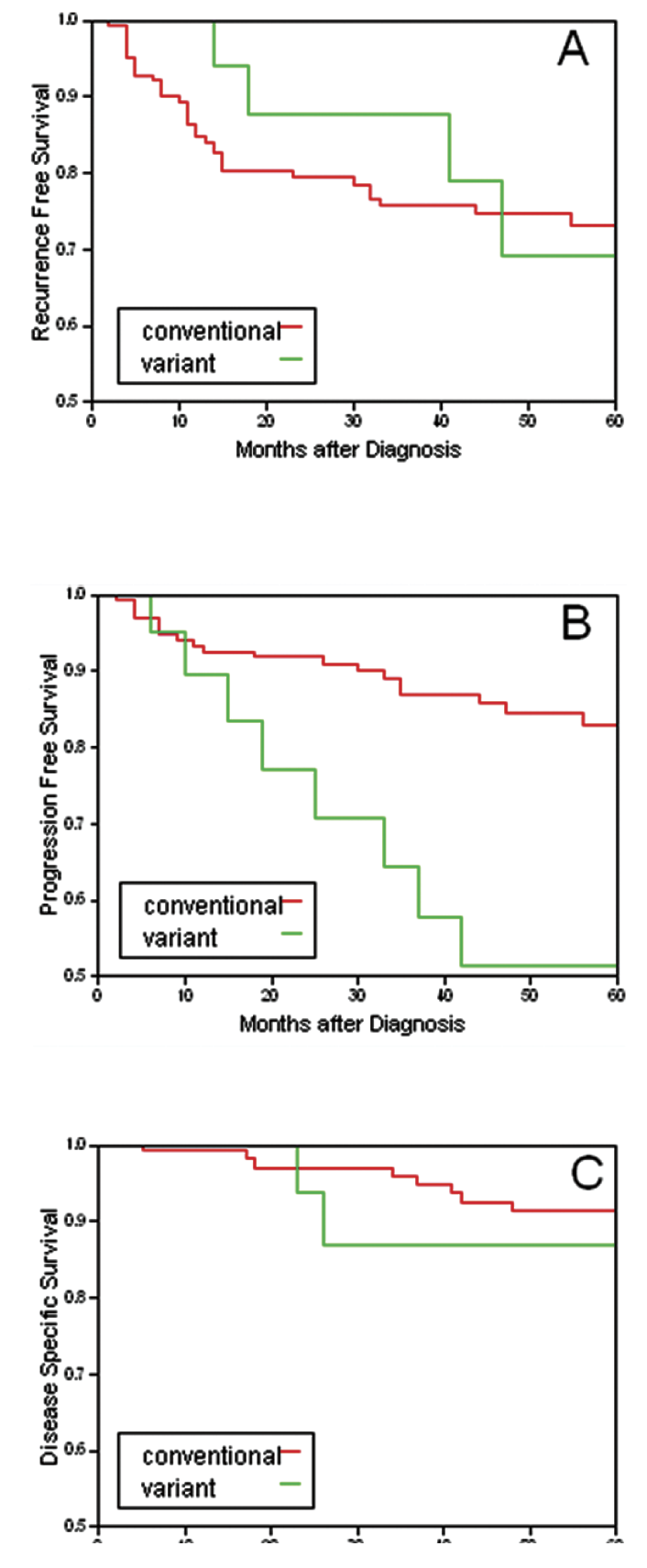
The 2 and 5-year disease specific survival rates however, were not significantly different (97% and 91.43% for patients with conventional carcinoma and 94.74 % and 82% for patients with variant disease, P=0.33).
Discussion
Histological variants of urothelial carcinoma are not uncommon. In the current study variant tumors were found in 10.4% of the patients. The most common variants are the squamous, nested, micropapillary, sarcomatoid and the glandular types. These tumors are invariably high-grade and most commonly invade the detrusor muscle and are associated with poor prognosis. The presence of variant histology is considered an independent risk factor for extravesical disease but not for disease specific mortality. 5 Radical cystectomy, with or without neoadjuvant chemotherapy is advised to most patients with variant tumors and most of the literature on variant tumors reports on patients’ prognosis after radical cystectomy.2,5–7 There is however, a group of patients with variant tumors that do not invade the detrusor and that can be removed completely transurethrally. There is paucity in literature regarding the use of BCG in non-muscle invasive disease of variant histology.
In this study, patients with completely resectable variant tumors (confirmed by second look biopsies) were treated with BCG immunotherapy. Their outcome was compared to patients with conventional high-grade urothelial cancer treated with BCG. The groups were similar in age, gender distribution, stage and follow-up length. It was found that variant tumors are associated with higher progression rate but with similar disease specific survival.
Regarding the various variant tumors, squamous differentiation is one of the commonest histological variants of UC. After radical cystectomy, the finding of squamous differentiation increases the likelihood of local recurrence.6,8 Beside case reports, there are no studies of the response of these variant tumors to BCG. In our study, 7 patients with squamous differentiation were followed for median period of 34 months after BCG administration. Three had tumor progression, of which 2 patients had radical cystectomy and are under follow-up, where as 1 patient died from UC.
Nested carcinoma is another variant of the UC. About 70 cases have been reported mostly in the form of case reports. 1 Early cystectomy is recommended by most authorities. 9 In the current study, 6 patients with the nested variant did rather well. After a median follow-up of 75 months, 2 patients were found to have tumor progression, of which one patient underwent radical cystectomy and other underwent chemo radiation but none died from UC.
The micropapillary bladder cancer is an aggressive variant of UC. In the current series, 4 patients with micropapillary variant who received BCG were followed for a median period of 52 months. One patient developed progression, who received chemo radiation without cystectomy but died at 26 months. In the largest series of micropapillary bladder cancer, Kamat et al reported on 27 patients who received BCG for non-muscle invasive disease. Only 17% of them remained disease free after a median follow-up of 30 months 10 leading the investigators to the conclusion that BCG immunotherapy is ineffective against this disease. 11
The glandular variant of UC was found in only 4 patients in the current series. After a median follow-up of 22 months, none developed recurrence or progression. The largest series of noninvasive UC with glandular differentiation was reported by Miller and Epstein. 12 In that series, 7 patients were treated with BCG and follow-up was available in 6. None developed recurrence. The sarcomatoid carcinoma is typically locally or systemically advanced disease with poor prognosis compared to patients with conventional carcinoma in a similar stage. 1 A single patient with a sarcomatoid variant was given BCG in the current series. He developed tumor progression after 14 months and died of metastatic disease at 37 months. There are no reports in literature regarding the effectiveness of BCG in this variant. Aggressive multimodality treatment with neoadjuvant chemotherapy and radical surgery is probably the best therapy for this disease and not BCG immunotherapy. 2 To summarize, our study suggests that intravesical BCG has a role in treating selected patients with variant histology tumors that are non bulky (<4 cm) and completely resectable transurethrally. Patients with glandular, squamous and the nested variants respond reasonably well to this therapy, while the micropapillary variant tends to progress despite treatment. The study is limited by the small number of patients and by being single institutional and retrospective. The combined analysis of several variant tumors together, although a common methodology,5,7,13 is another limiting factor.
Conclusions Patients with non-muscle invasive variants of bladder cancers can be managed with intra-vesical immunotherapy with BCG provided the tumor is not bulky, can be completely removed transurethrally and this is confirmed by second look biopsies. Higher progression rate to muscle invasive disease is expected compared to conventional urothelial carcinoma. However, when follow-up is meticulous, life expectancy is similar to patients with high-grade conventional urothelial carcinomas treated with intravesical immunotherapy. A patient choosing this therapy must be aware of the high risk of progression and disease specific mortality, and should be highly motivated to comply with the follow-up protocol.