
Abstract
Capillary hemangiomas are benign vascular neoplasms. When associated with the spine, these growths frequently involve the vertebral body, but rarely have they been reported to occur as intradural lesions, while even more rarely occurring in a true intramedullary location. We report a rare case of an intramedullary capillary hemangioma of the thoracic spinal cord and a review of the literature.
Introduction
Capillary hemangiomas are benign vascular neoplasms typically encountered in the skin. They occur most frequently in childhood as cutaneous or subcutaneous lesions characterized histologically by nodules of capillary-sized vessels lined by flattened endothelium. 1 As the most common primary tumor of the spine, capillary hemangiomas are frequently encountered as interosseous lesions. The occurrence of these tumors in the central nervous system, however, is exceedingly rare and they are even less frequently encountered as intramedullary lesions. 2 Despite the high prevalence of vertebral body hemangiomas, extraosseous extension causing neurological impingement remains uncommon.
In the present case, we report an intramedullary capillary hemangioma of the thoracic spinal cord, an exceedingly rare presentation with few previously reported cases existing in the literature.2–6
Case report
The patient is a 47-year old right-handed man with several months of non-specific mid-back pain, lower extremity hyperesthesia, and a more recent two week history of gait difficulties. His past medical history is significant for a prior left-sided intracerebral hemorrhage with consequent hemiparesis three years ago.
The patient's baseline deficits associated with his prior left hemisphere stroke included dysarthria, right facial weakness, and a dense right hemiparesis. New deficits included 3-4/5 strength of the left lower extremity and a sensory level just above the nipples consistent with approximately a T3 spinal level. Reflexes were 3+ in the bilateral lower extremities. Babinski reflex was present bilaterally.
MRI of the thoracic spine both before and after the administration of intravenous Gadolinium demonstrated what initially appeared to be a homogenously enhancing intradural, extramedullary lesion displacing the cord anteriorly with significant cord deformation (Figure 1). Our differential diagnosis included: nerve sheath tumor, meningioma, and ependymoma.
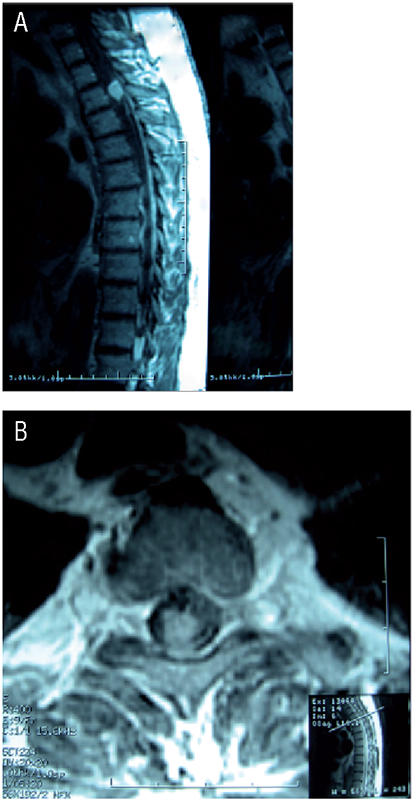
(A) Sagittal T1-weighted MR image with Gadolinium revealing a homogeneously hyperintense mass involving the upper thoracic spine. (B) Axial T1-weighted MR image with Gadolinium demonstrating a centrally located lesion.
The patient was offered an excisional biopsy of the lesion. T2 and T3 laminectomies were performed, and the lesion location was confirmed using intra-operative ultrasound. Intradural exploration revealed a highly vascular, partially encapsulated cherry-red lesion that appeared to arise from the dorsal aspect of the spinal cord. In contrast to MRI findings, the tumor was found to be intramedullary in location. Overlying the tumor was a region of thickened arachnoid, but no demonstratable dural attachment. Several involved nerve roots were coagulated and divided. Further dissection revealed an extremely friable exophytic tumor arising from the region of the dorsal root entry zone of T3. Intra-operative frozen section was consistent with a possible hemangiopericytoma. Post-operative MRI showed no evidence of residual tumor.
On histopathology, the tumor grossly consisted of a partially circumscribed lesion with a brownish-tan appearance. H&E staining demonstrated a hypercellular, vascular neoplasm composed of cytologically bland spindled cells with minimal cytoplasm. These cells were arranged in vague lobules of short irregular spindle cells and dilated vascular spaces. Immunohistochemical findings are explained in Figure 2. Further evaluation demonstrated dilated, compressed vascular channels and focal extramedullary hematopoiesis. In total, the findings were consistent with capillary hemangioma.

(A) Photomicrograph of H&E stain shows a hypervascular tumor composed of thin and irregular capillary vessels and minimal cytoplasm. Magnification X 200. (B) Immunohisto-chemical staining revealed the tumor cells to be strongly and diffusely immunoreactive for CD31, CD34, and CD99. Scattered S-100 protein and BCL-2 positive cells were present. Epithelial membrane antigen (EMA) and inhibin stains were negative and MIB-1 labeling was brisk, but with rare mitoses. Magnification X 200.
Post-operatively the patient had good functional recovery. At three months follow-up the patient had only minor residual lower extremity dysesthesia with return of baseline motor function. The patient has remained stable 36 months post resection.
Discussion
Capillary hemangiomas involving the spinal cord are extremely rare, and are most frequently extramedullary in location.1–3 We are aware of only a handful of previously reported cases of intramedullary spinal cord capillary hemangiomas (Table 1). Notably, all but one previously reported case involved the thoracic spine or the conus.

Although several patients had imaging studies suggesting “extramedullary” lesions, they were ultimately found to have intramedullary capillary hemangiomas. h/o = history of; UMN = upper motor neuron; LMN = lower motor neuron; LBP = lower back pain; DTR = deep tendon reflexes; R = right; L = left.
MRI is the gold standard imaging modality for intramedullary lesions.13–16 Many such lesions can be safely removed with proper imaging, surgical planning and technique. In the case of intramedullary capillary hemangiomas, however, on MRI the lesion can be interpreted as extramedullary,5,8,10 and the original differential diagnosis often fails to include capillary hemangioma,2,8,11 as was the case with our patient. As previously discussed by Roncaroli et al. and Nowak et al., the treating surgeon must be cognizant of intramedullary capillary hemangiomas to avoid misdiagnosis and potential excessive treatment.1,2 Although extremely rare, capillary hemangiomas of the spinal cord have a benign clinical course. Glial based tumors, such as ependymomas and astrocytomas, account for over 90% of intramedullary tumors. 17 The distinctive gross appearance of capillary hemangiomas intraoperatively often eliminates the more common glial based lesions from the differential diagnosis. The remaining possibilities include lesions ranging from: hemangiopericytoma, hemangioblastoma, cavernous angioma, hemangioendothelioma, arteriovenous malformations, venous angiomas, and capillary telangiectasias. Fortunately, histopathological analysis reliably distinguishes these lesions for diagnosis.
Although related most closely to the category of vascular malformations, capillary hemangiomas that appear within the spinal cord parenchyma may have their origins elsewhere. Similar to intramedullary lipomas (which account for 1% of intramedullary lesions), capillary hemangiomas of the spinal cord may represent a form of dysembryogenesis. Rather than being a true neoplasm, these lesions more likely arise from inclusion of mesenchymal tissue into the neural tube during primary neurulation.18–20 The available literature clearly demonstrates the benign nature of intramedullary capillary hemangiomas, and gross total resection appears to be curative with good outcomes and no reported recurrences (Table 1). Given the rarity of this lesion, its benign course and straightforward therapy, surgeon familiarity is important to ensure patients receive appropriate diagnosis and treatment.