
Abstract
Background
Thailand has a higher global non-communicable disease (NCD) mortality rate in comparison to the rest of the world, accounting for 75% and 71% of all deaths. WHO focused increasingly on health literacy (HL) in order to decrease NCDs. This study aimed to assess the effectiveness of an HL intervention utilizing transformative learning and positive psychology with mindfulness training in terms of changing levels of HL, health behavior (HB), and health outcomes.
Design and methods
The study was a randomized control trial from May to September 2019. The participants were a rural Thai population with low levels of HL, living in an area with high levels of NCDs. The 200 participants were cluster randomly allocated to an eight-week intervention, and the control group. The data were collected by Likert questionnaires and physical exams, and analyzed via ANOVA.
Results
The intervention group mean scores for HL, psychological capital, HB, and family well-being increased from baseline to post-intervention, but decreased during the follow-up but were still significantly higher than the control group and baseline scores. The increases in HL and HB were matched by improvements in physiological measurement. The BMI scores of the intervention group decreased in each phase, while the control group scores remained largely unchanged. An intervention group had significantly lower fasting blood sugar than the controls at the intervention and in the follow-up. There was no interaction between social support and any other variables.
Conclusions
This program demonstrated improvements in HL, HB and the well- being of Thai families at risk of NCDs in rural communities.
Introduction
Improving self-efficacy and health literacy (HL) is consistently associated with developing healthier behavior and reducing the rate of non-communicable diseases (NCDs).1–3 Thailand has a high rate of NCDs, accounting for 75% of all deaths. 4 Poor HL correlates with NCD rates and in a Thai national survey, only 5.5% had high HL, with half the population at a low level. 5 Rates of obesity are also high, with 33% of men and 42% of women were obese and one in three adults had hypertension and one in ten are diabetics. 4 Accordingly, the researchers were interested in reducing obesity, diabetes and hypertension by improving HL via a social and cognitive skills educational development program and introducing healthier behaviors in line with the Thai health promotion aim of decreasing NCDs. The health education program incorporating transformation learning, behavior modification, a positive psychology mindfulness intervention designed to encourage positive thinking, appreciation and gratitude was designed with the aim of improving HL and health behaviors (HB). The psychological character strengths of individuals were also assessed to explore whether or not the intervention resulted in increases in psychological capital (PsyCap). 6
Significance for public health
The WHO highlighted concerns about the rise of NCDs worldwide and tried to establish healthy populations to promote well-being and quality of life. Global conferences on health promotion in Shanghai prioritized increasing health literacy and well-being to decrease NCDs globally as part of a sustainable development agenda. Hence, the improvement in health literacy, family well-being and the good health outcomes of NCD risks were challenge for public health providers as changing health behaviors of individuals and communities. This study confirmed that the most often used health literacy and mindfulness-based intervention via the transformative learning process can provide effective alternative therapies and controlling BMI, blood pressure, and blood sugar for NCD risks worldwide, especially Asian people in endemic areas of hypertension and diabetes. This health literacy intervention can contribute to all health providers for their effective health care services.
Based on the previous research, three elements of HL were addressed in the design of the intervention: i) functional literacy consisting of access to and understanding of health information; ii) interactive literacy, consisting of communication and self-management skills; and iii) critical literacy, consisting of media literacy and decision-making skills.7–10 Transformative Learning Theory 11 provided a framework for developing HL and behavior change with its aim of encouraging a rational analytic approach to problematic HBs. 12 Homework was agreed on between sessions and the behavior modification principles to reward and reinforce behavior were incorporated to encourage compliance. 13 The group setting also provided social support for members.
Research in positive psychology 14 has consistently shown that individuals with higher levels of hope, optimism, self-efficacy, and resilience, sometimes labelled PsyCap, 15 experienced higher levels of well- being and mental health.6,16–18 For this reason, the levels of psychological strengths were assessed in both samples. The health intervention focused on encouraging positive emotions and self- efficacy, which if successful, would be reflected in the measures of hope, optimism, self- efficacy, and resilience, postintervention. The intention was to enhance well-being and strength development further by including an intervention on mindfulness which has been shown to foster well-being and help with weight and decreasing blood pressure (BP).19,20 The intervention was designed to be delivered to groups of participants as the presence of social support has been shown to increase the effectiveness of such interventions, 21 as well as being more cost effective. To summarize, the aim of this study was to examine the effectiveness of a HL program based on transformative learning, including positive psychology and incorporating behavior modification in changing behavior and improving health in a population at high risk of developing NCDs and to compare the outcomes with a normal treatment control group, who were receiving regular health care in their community, but no HL education. The aim was to address national goals of reducing obesity, diabetes and hypertension. The first hypothesis was that the intervention group postintervention and at one- month follow- up, would have higher levels of HL, HB, family well-being (FWB) and lower BMI, BP and fasting blood sugar (FBS) levels than the control group. Secondly, it was hypothesized that the intervention would increase levels of psychological strengths in the intervention group when compared with the control group.
Thirdly, it was hypothesized that there will be an interaction between levels of social support available to participants and health outcomes namely HL, FWB and HB, with higher levels of support associated with greater improvement.
Design and methods
This study was a randomized control trial of RCTs by repeated- measures design. The experimental study was conducted from May to September 2019.
Participants
The two hundred volunteers from rural communities in the area of Thailand that had the lowest levels of HL were recruited by local health workers. The permission for this was received from the Department of Public Health who also allowed access to relevant health data on all of the participants. All of the participants were randomly allocated to an either experimental or control group by cluster random sampling from eight villages. The demographics of both groups are similar, with the majority at 41-59 years of age, female, with an elementary level of education, and a marital status of living with a spouse.
Procedure
In the intervention condition, there were five groups of 20 participants who met in community centers in different areas for three hours over eight weeks, followed by a follow-up meeting for feedback and health monitoring in week 12. The participants were paid a small amount to cover their time. The control group was a treatment as normal group with access to the normal services provided locally, but no HL courses. The control group participated in the baseline assessment and the follow-up measures. Information about the study was provided to participants and they also gave consent for information for their health records to be accessed with reassurances that any information would remain anonymous.
Measures
The Thai Adult Health Questionnaire 22 is a culturally appropriate, comprehensive measure of HL, HB, family health and healthrelated social support, developed for use in Thailand. The PsyCap Questionnaire (PCQ), Luthans et al. 15 measures hope, self- efficacy, optimism and resilience. Health measures at baseline, postintervention and follow up were BMI, cholesterol, FBS levels, systolic and diastolic BP. The data were collected with a Likert questionnaire with a reliability of 0.79-0.93, and analyzed using ANOVA.
HL development program
The ten phases of transformational learning are as follows: i) presentation of a disorienting dilemma incorporating risk factors for NCDs that do not fit existing beliefs, ii) individual reflection on the dilemma; iii) critical assessment of their assumptions; v) recognizing mismatches and discussing it with others; v) explore new options; vi) plan changes; vii) acquire new knowledge to implement changes; viii) practice new behaviors; ix) build up confidence in new roles and actions; and to x) reintegrate necessary lifestyle changes, which were systematically worked through. 11 Different dilemmas were presented for each targeted unhealthy behavior with client involvement in topic selection. The group facilitator introduced behavior modification techniques, such as rewards for compliance and non- compliance with the homework set between sessions and this was discussed and debated within the groups. The techniques included providing educational materials, discussions, weekly mindfulness practice, telephone counselling between sessions to encourage compliance, encouraging selfmanagement and active learning methods such as brainstorming, role play, safe use of social media, exchanging experiences and supporting each other in their attempts to change.
Results
The presence of risk factors among the participants associated with developing NCDs measured at the baseline. There was no statistically significant difference between the groups for obesity, hypertension, high blood sugar, high cholesterol, and no exercise. Most of the participants had more than one risk factor. The means for the variables measured at each phase of the study are shown in Table 1. To test the first hypothesis, a repeated measures ANOVA tested the mean difference scores of the intervention and the control group at each intervention phase and the one-month follow-up. As shown in Table 2, the intervention group had statistically significant higher levels of HL, PsyCap, HB and FWB, compared to the control as predicted. To explore further the statistically significant interactions between HL, HB, FWB, BMI, FBS level and systolic BP at each intervention point, the differences between the mean scores for each variable at each phase were computed using the Bonferroni method. These are displayed in Table 3. The mean differences between the intervention and control group at each phase were statistically significant for all the variables apart from BMI and diastolic BP. From Table 4 it can be seen that PsyCap was significantly higher in the intervention group than the control group post-intervention and was maintained at the follow-up supporting the second hypothesis. In order to test the third hypothesis a two-way ANOVA was computed to compare the different levels of support in the intervention and the control group and their effects on HL, PsyCap, HB and FWB. The results in Table 4 show significant differences in the mean scores for HL, PsyCap, HB, and FWB between the intervention and control group. The statistically significant differences in social support between the groups were found for HL, HB, and FWB, but not PsyCap.
Description of HL, psychological capital, HB, FWB and health outcomes among the intervention group, the control group and phases of measurement.

Comparison of mean scores between the intervention and the control group by phase of intervention for HL, psychological capital, HB, FWB, BMI, FBS, BP.
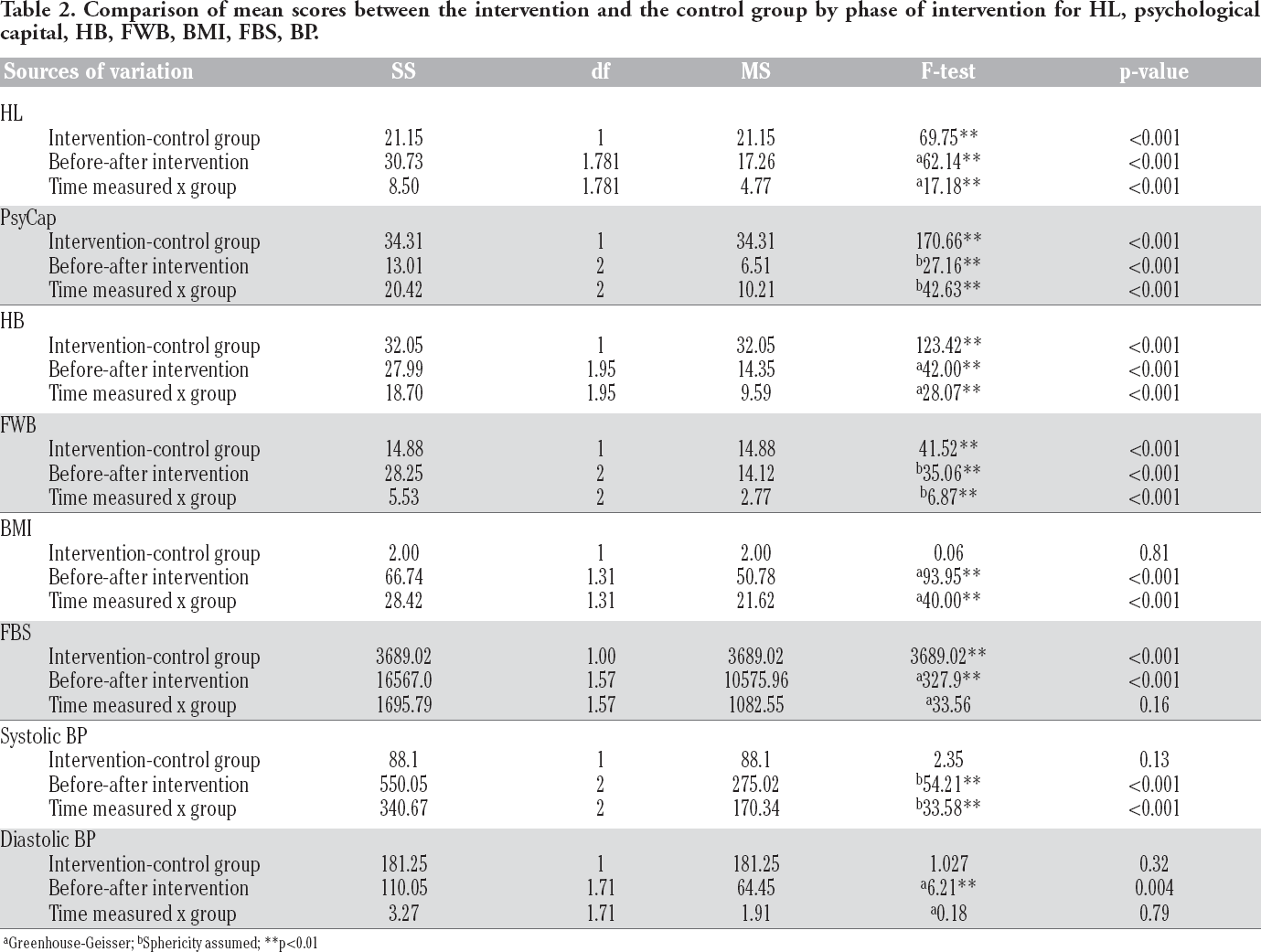
Greenhouse-Geisser
Sphericity assumed
p<0.01
The interaction between types of group and social support was statistically significant for HL but not for any of the other variables. Pairwise comparison using Bonferroni’ s method, were computed and this found only one pairwise difference among the participants in the control group; participants with lower levels of social support had a lower mean score of HL than those with high levels of social support supporting the hypothesis.
Discussion
The objective of this research was to assess the effectiveness of a HL program utilizing transformative learning, incorporating mindfulness training as an aspect of positive psychology, to encourage positive thinking, appreciation and gratitude in changing levels of HL, HB and family health when compared with health care as a normal control
These increases in HL, HB and FWB provided further confirmation that transformative learning was an effective tool in acquiring knowledge and motivating change. In psychological terms, by challenging existing beliefs it created cognitive dissonance, produced the motivation of planning changes in behavior.11,12 It was acknowledged that behavior change was difficult and it was for this reason that behavior modification techniques were included to reinforce the practice of planned changes in behavior which were agreed by participants as homework to be completed between sessions. 13 Qualitative observations suggested that homework activities were ongoing completed and likely to have contributed to the successful outcomes specifically for HB and FWB.
The range of activities that focused on FWB emphasized taking care of family members with video clips of healthy lifestyles, role playing situations similar to actual experience related to family matters, their lifestyles and cultures to reflect how changes could impact positively on their families and themselves. All sessions were focused on activities that encouraged positive attitudes to increase levels of self- efficacy in the intervention group, which progress being regularly praised so participants came to be more optimistic than they can make changes for themselves and their families then they become hopeful of leading a healthier lifestyle in future. The support from the group members and the facilitators was so important here for increasing the confidence that participants had in implementing changes for themselves and their families. They moved from focusing on acquiring accurate health knowledge for themselves to engage their wider family in selfcare, with activities such as encouraging families to exercise together and prepare their own healthy foods with recipes that had been introduced at the sessions. Incorporating mindfulness practices into the sessions was culturally appropriate as meditation was a part of the practice of Buddhism and enhances wellbeing and more positive thinking as reported by Rogers et al. 19 that the intervention group participants’ scores on hope, self-efficacy, optimism and resilience increased throughout the intervention and were maintained at the one- month follow- up and were evidence of the success of positive psychology in the program. Previous research had shown that such activities enhanced confidence in their ability to undertake new activities, improve the quality of their lives and their families.14,23 This is supported in a survey of the health of families in a high-rise building in Bangkok, where self-efficacy and resilience together predicted 64% of the variance in Buddhist holistic health. 24 Similarly, Intarakamhang and Ekpanyaskul 25 exploring factors contributing to FWB in Thai urban communities, found that FWB was directly affected by the PsyCap levels. This suggested that incorporating positive psychology into HL interventions can directly enhance FWB.
Comparison of the mean scores between the intervention group and the control group by phases of measurement using Bonferroni's Pairwise comparison method.

Analysis of mean difference scores between the intervention group and the control group by phase of intervention for HL, psychological capital, HB and family well-being by levels of social support measured at follow-up.

p<0.01.
The HL and HB scores of the intervention group significantly increased from baseline to post- intervention and the differences were maintained at follow-up and were significantly higher than the control post- intervention and at follow-up. These results supported those of a survey exploring the relationship between HL and HB, specifically exercise, alcohol intake and fruit and vegetable consumption in older adults, 26 where higher levels of HL were associated with engaging in healthier behaviors. Singhasem, Krinara and Tiparat 27 explored the relationship between HL and HB that found that HL was positively correlated to a moderate degree with healthy levels of exercise, food consumption and better emotion management although the numbers in the study were relatively small. Nutbeam 28 suggested that it was the development of interactive and critical approaches to HL that promoted self-care management resulting in better healthcare practices in individuals and families. Transformational learning as used in this study certainly engenders critical interactive learning in a supportive social context that was also culturally appropriate.
The increases in HL and HB scores were matched by improvements in physiological measures of health, thereby providing objective evidence of improvements in health. While the mean BMI scores of the intervention group decreased at each phase, these differences did not reach statistical significance. The new behaviors regarding exercise and diet, were gradual weight loss, which is the desired outcome for long term changes so that weight loss is maintained long term. The control group scores remained largely unchanged. In terms of the FBS levels, there were no differences between the intervention and control group at baseline but the intervention group had significantly lower blood sugar level than the controls at the end of the intervention and at follow-up. Nitri and Stewart 29 in a study applying transformative learning to improve HL around diabetes to reduce sugar consumption in older adults with diabetes found similar reductions in FBS levels at the end of their study. Similarly, Chiangkhong et al. 30 delivered HL through transformative learning produced improvements in glycemic control behavior amongst adults with diabetes. For systolic BP, there were no differences between the groups at baseline and immediately post- intervention, but at follow- up the intervention group had significantly lower readings. There were no significant differences in terms of diastolic BP.
The current study was interested in whether or not that social support contributed to bringing about behavioral change
Limitations
This was a large-scale intervention with good levels of compliance. There may have been elements of social desirability responding with participants as relationships developed with the researchers and this could have inflated somewhat results in some areas. Future studies might want to consider incorporating measures to combat this. The intervention was delivered as a totally integrated program so evaluation of the individual components was impossible as this would have placed too much strain on the participants and possibly led to withdrawals from the program. Future studies could assess the impact of behavior modification as this was a relatively inexpensive way for providing the structure to support behavior change.
Conclusions
This random controlled trial demonstrated the efficacy a HL program based on transformative learning and incorporating positive psychology with groups in rural communities at risk of developing NCDs, who previously had low levels of HL.
Footnotes
The authors declare that they have no competing interests, and all authors confirm accuracy.
Acknowledgements
The authors would like to thank all of the participants, including who serve as health providers as research assistants, the gatekeepers of the target communities and sample groups. This study is a final part of a multi-phase project, under the Newton Funding. We would like to acknowledge the British Academy via the Newton Advanced Fellowship Grant No. AF170002/2017 and the Thailand Research Fund Grant No. DBG/612561.