
Abstract
Selection of an optimal donor pancreas is the first key task for successful islet isolation. We conducted a retrospective multicenter study in 11 centers in North America to develop an islet donor scoring system using donor variables. The data set consisting of 1,056 deceased donors was used for development of a scoring system to predict islet isolation success (defined as postpurification islet yield >400,000 islet equivalents). With the aid of univariate logistic regression analyses, we developed the North American Islet Donor Score (NAIDS) ranging from 0 to 100 points. The c index in the development cohort was 0.73 (95% confidence interval 0.70–0.76). The success rate increased proportionally as the NAIDS increased, from 6.8% success in the NAIDS < 50 points to 53.7% success in the NAIDS ≥ 80 points. We further validated the NAIDS using a separate set of data consisting of 179 islet isolations. A comparable outcome of the NAIDS was observed in the validation cohort. The NAIDS may be a useful tool for donor pancreas selection in clinical practice. Apart from its utility in clinical decision making, the NAIDS may also be used in a research setting as a standardized measurement of pancreas quality.
Introduction
Allogeneic islet transplantation (AIT), a β-cell replacement therapy, is used in a highly select group of patients with type 1 diabetes. These patients suffer from recurrent severe hypoglycemic episodes and extensive glycemic liability. AIT is a minimally invasive therapeutic procedure compared to whole pancreas transplantation, restoring physiological glycemic control without severe complications. Since the Edmonton Protocol was published in 2000 1 , AIT has been applied in many institutions worldwide. Improved islet processing techniques as well as clinical immunosuppressive regimens implemented in the following years allowed for enhanced short- and long-term metabolic control, comparable to results after whole pancreas transplantation2,3. The routine transition of islets collected and transplanted from two to four donors down to one donor per recipient has become critical for advancement of the field from logistic, medical, and financial points of view 4 . This would also limit a recipient's exposure to multiple donor human leukocyte antigens (HLA) and immunological sensitization. Based on current experiences, the minimal islet mass required for the initial transplantation, in order to produce a substantial metabolic effect, has been set for 5,000 islet equivalents (IEQ) per kilogram of the recipient's body weight 4 . Therefore, islet processing centers have focused on improving isolation results in order to consistently obtain higher islet yields. Islet isolation results depend on two major factors—characteristics of the donor/pancreas and islet processing technique. Now, after more than a decade of technical efforts, islet processing techniques appear to have reached a mature and stable stage. The selection of an optimal donor pancreas remains an initial key task prior to islet isolation. It is inarguable that despite the best islet processing technique, islet isolation fails when a poor quality donor pancreas is chosen.
There are two categories of donor variables that are correlated with islet isolation outcomes: variables predicting pancreas weight and variables related to pancreas quality. Pancreas weight predictors are donor age, gender, body surface area (BSA), body mass index (BMI), body weight (BW), and body height5–22. The pancreas quality predictors are cold ischemia time (CIT), donor age, blood chemistry indicating function of pancreas, liver, and kidneys, medical history, cause of death, duration of hospital stay, vasopressor usage, and organ procurement team8,13,14,16,18,20,22–28. To standardize the pancreatic donors using a combined donor variable approach, O'Gorman et al. published the first study with an islet donor score resulting from variables of 326 donors between 1999 and 2004 in a single center 28 . As islet mass required for transplant remains >5,000 IEQ per kg of recipient BW, in our analysis we defined successful islet isolation as those with a postpurification islet yield greater than 400,000 IEQ, which is the highest cutoff value among those defined in the previous studies6,8,9,26. With this rigorous definition, transplant can be accomplished in most of the patients (those with weight ≤80 kg). Herein we report our findings from a multicenter study, wherein donor variables were assessed to produce a new donor scoring system, which can be used as a routine objective tool for pancreas selection prior to islet isolation in clinical practice.
Materials and Methods
Study Cohort
We conducted a retrospective multicenter study of 1,235 islet preparations obtained from deceased donors at 11 centers in North America (University of Alberta in Canada, Baylor University in Dallas, University of California San Francisco, University of Chicago, University of Illinois at Chicago, Massachusetts General Hospital, University of Miami, University of Minnesota, Allegheny Health Network Pittsburgh, University of Pennsylvania, and University of Wisconsin). The data set consisted of 1,056 islet isolation procedures performed between March 2007 and December 2013 and was used for the development of a scoring system using donor variables to predict islet isolation outcome (development cohort). For validation purposes, a separate cohort of islet preparations was analyzed. This validation cohort was derived from 179 consecutive islet isolations performed between February 2013 and January 2015 at the largest volume center among 11 centers. This study protocol was reviewed and approved by the Institutional Review Board (IRB) of the Division of Biological Sciences at the University of Chicago and was identified as nonhuman subject research, as determined by Federal Regulations. All donor data were entered in REDCap Project in the University of Chicago website before analysis. Based on communications with the IRB at the University of Chicago (IRB12-2187), the study did not require review by IRB of the other 10 centers.
Outcome
Our outcome measure of interest was postpurification islet yield as expressed in IEQ. Islet yield was determined by manual count of dithizone-stained samples, converting the different islet sizes into IEQ 29 . Successful islet isolation was defined as postpurification islet yield greater than 400,000 IEQ. Within the development cohort, there were 29 cases with missing postpurification IEQ data but postculture IEQ data was presented (mean ± standard deviation (SD) culture time was 47.8 ± 10.4 h). For those cases, we used postculture IEQ as the measure of islet isolation outcome. Cases other than successful islet isolation were labeled as failed islet isolation.
Donor Variables
Candidate predictor variables used in the analyses were age, gender, BW, height, BMI, and BSA calculated with the Mosteller formula 30 , CIT, cause of death, length of hospitalization, vasopressor requirement, procurement team, medical history, and blood test values including maximum and minimum glucose, peak levels of amylase, lipase, aspartate transaminase (AST), alanine transaminase (ALT), blood urea nitrogen (BUN), creatinine, sodium, and hemoglobin A1c (HbA1c). Cause of death was categorized into cerebrovascular accident, anoxia (including donation after cardiac death), head trauma with abdominal injury, head trauma without abdominal injury, and others. The procurement team was considered either “own” if the team was affiliated with the islet isolation center, or “distant” if not. Length of hospitalization was stratified into four categories: <2, 2–4, 5–7, and >7 days. Vasopressor requirement was stratified into five categories based on the number of different agent types used: none, single, double, triple, and more than three agents. Regarding medical history, the following information was collected: alcohol abuse, hypertension, and cardiac arrest.
Development and Validation of Scoring System
Using the development cohort, we conducted univariate logistic regression analyses to identify donor variables that predict islet isolation success. We then created donor scoring systems (points from 0 to 100) consisting mainly of several donor variables influencing the outcome. We plotted a receiver-operating characteristic (ROC) curve for each scoring system. We calculated an area under the curve (AUC) (also referred as c index) to assess the ability of the scoring system to predict successful islet isolation. We identified a scoring system having the highest AUC and named it the North American Islet Donor Score (NAIDS). Finally we tested the validity of the NAIDS on the validation cohort.
Statistical Analysis
Continuous variables are presented as mean ± SD. Categorical variables are shown as the percentage of the sample. A value of p < 0.05 was considered significant. Univariate logistic regression analyses and unpaired t-tests were conducted using SPSS version 19 (IBM, Armonk, NY, USA). The comparison of two uncorrelated ROCs was based on a form of a Z statistic that uses the difference in the area under the two curves and the standard error of each AUC.
Results
Donor Characteristics
The donor characteristics of 1,056 islet isolations are shown in Tables 1 and 2. The mean age of donors was 45.8 years and ranged from 5 to 77 years. The proportion of male donors was 55.5%. Cerebrovascular accidents accounted for the most frequent causes of death. The proportion of donors receiving zero, single, double, and triple vasopressor therapy during their hospital stay was 14.4%, 38.0%, 26.3%, and 14.5%, respectively. Mean CIT was 9.4 h, ranging from 0.67 to 23.8 h. The majority of donors stayed in the hospital for less than 5 days. Mean amylase and lipase peak levels were 136 and 78 U/L, respectively. Mean maximum and minimum blood glucose levels were 235 and 119 mg/dl, respectively. The mean HbA1c was 5.6%, but data were available in only 552 cases (52.3%).
Donor Characteristics in the Development Cohort: Continuous Variables

Donor Characteristics in the Development Cohort: Categorical Variables

115 cases have multiple events.
Univariate Logistic Regression Analyses
Of the 1,056 analyzed cases, 286 (27.0%) were successful islet isolations. Univariate logistic regression analyses revealed that the following donor variables were significantly associated with successful islet isolation: greater height, greater BW, greater BMI, larger BSA, male gender, shorter CIT, lower peak blood glucose, lower sodium level, pancreas procured by own team, fewer different vasopressor types, and the occurrence of cardiac arrest (Table 3).
Univariate Logistic Regression Analyses for Prediction of Successful Islet Isolation

Donor Score
Initially we employed a previously published method 31 to create a simplified scoring system based on a multivariate logistic regression model and estimated the score weights. However, we obtained an unsatisfactory scoring system with a ROC-AUC of 0.681, which has a poor discriminative ability. Therefore, we empirically created 87 different donor scoring systems with the aid of the results of univariate logistic regression analyses. Among 87 systems, a donor scoring system with the highest AUC value, hereafter referred to as the NAIDS, is presented in Table 4. The NAIDS is comprised of three main influential donor variables (BSA, number of different vasopressor types, and BMI) and two supplemental composite factors (unfavorable and favorable factors). Some of the variables in the NAIDS were not statistically significant in the univariate analyses, but by including nonsignificant variables as a composite factor, the NAIDS obtained an AUC of 0.730 (95% confidence interval 0.697–0.763) (Fig. 1). A brief explanation as to how we created the NAIDS should be provided. High amylase and lipase levels are both generally considered undesirable, but only the amylase level was included in the NAIDS because we found that including the lipase level did not increase the AUC. We found that the CIT of pancreases procured by the center's own team was significantly shorter than that of pancreases procured by an unaffiliated team (5.9 ± 2.6 vs. 10.5 ± 3.8 hours, p < 0.001, t-test). Thus, procurement team was highly associated with CIT. However, excluding one of those factors from the NAIDS resulted in a lower AUC value, leading us to include them both (CIT and procurement team) in the NAIDS. Finally, the threshold of the biochemical tests such as AST, ALT, BUN, and amylase was manually determined to obtain the highest possible AUC.
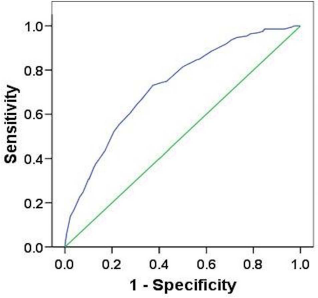
Receiver-operating characteristics (ROC) curve of the NAIDS in the development cohort. Blue line indicates ROC curve and green line indicates diagonal reference. Area under the curve was 0.730 (95% confidence interval, 0.697–0.763).
North American Islet Donor Score
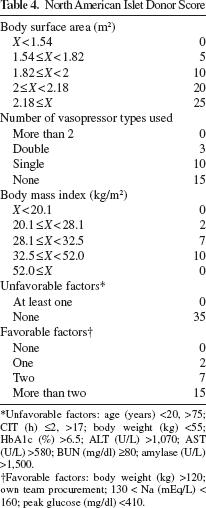
Unfavorable factors: age (years) <20, >75; CIT (h) ≤2, >17; body weight (kg) <55; HbA1c (%) >6.5; ALT (U/L) >1,070; AST (U/L) >580; BUN (mg/dl) ≥80; amylase (U/L) >1,500.
Favorable factors: body weight (kg) >120; own team procurement; 130 < Na (mEq/L) < 160; peak glucose (mg/dl) <410.
Success Rate Based on the NAIDS
We grouped the NAIDS into five strata to allow the application of the NAIDS stratification for comparisons of outcomes. The success rate increased proportionally as the NAIDS increased, from 6.8% (14/206) success in the NAIDS < 50 points to 53.7% (102/190) success in the NAIDS ≥ 80 points (Fig. 2).

Successful islet isolation rate by the NAIDS for both development and validation cohorts. The success rate increased proportionally as the NAIDS increased in both development and validation cohorts.
Validation of the NAIDS
For validation of the NAIDS, we plotted the ROC curve using the validation cohort data (n = 179). The ROC–AUC was 0.713 (95% confidence interval 0.637–0.788) (Fig. 3), which was not significantly different (p = 0.67) from that obtained from the development cohort. Furthermore, a similar proportional increase in a success rate was observed as the NAIDS increased in the validation cohort (Fig. 2).
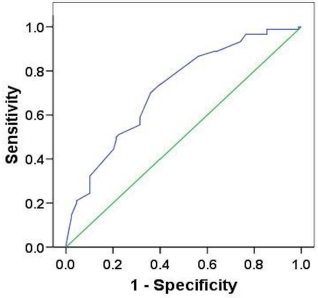
Receiver-operating characteristics (ROC) curve of the NAIDS in the validation cohort. Blue line indicates ROC curve and green line indicates diagonal reference. Area under the curve was 0.713 (95% confidence interval, 0.637–0.788).
Discussion
The NAIDS is a comprehensive scoring system. It consists of donor variables that predict pancreas weight and quality out of a total of 100 points. A higher NAIDS corresponds to a higher success rate with postpurification IEQ yielding over 400,000.
The NAIDS has three variables for pancreas weight estimation (i.e., BSA, BMI, and BW). BSA is given a maximum of 25 points, followed by BMI with 10 points. BW is allocated into the unfavorable and favorable factors. BMI as a measure for pancreas weight estimation has been used for many years in the islet field. However, it is not a completely accurate indicator. Although the BSA and BMI are both calculated from the body weight and height, the calculation formulas are different. Kin et al. reported that BW and BSA were more strongly correlated with pancreas weight 11 . The NAIDS stresses more on pancreas weight estimation using combined variables of BSA, BMI, and BW.
The NAIDS sets 65 points in the estimation of pancreas quality. The human pancreas is a more vulnerable abdominal organ compared to others such as the liver and kidneys. Islets as a tiny endocrine organ represent approximately 1% to 2% of the total pancreatic tissue and are surrounded by acinar cells containing protease. Most researchers believe that early activation of intracellular zymogen in the process of acute pancreatitis leads to a trypsin cascade that subsequently causes autodigestion of acinar cells 32 . It is clear that a pancreas with chronic pancreatitis is not a suitable donor organ. However, even in stable but brain dead conditions, a donor may suffer from impaired vascular autoregulation and decreased tissue perfusion pressure that subsequently cause declines in tissue perfusion and hypoxemia of the pancreas. It can evoke cellular damage and further result in autodigestion of pancreatic tissue. A study 12 in a rat model showed that exocrine tissue injury occurred with dynamic amylase release during pancreas preservation at 4°C. Furthermore islet injury was found to correlate with amylase release and led to a reduced number and viability of isolated islets. Loganathan et al. 33 reported that human isolated islet loss after culture was significantly higher in impure relative to pure preparations. Furthermore, lower islet purity was associated with many potential drawbacks including increased protease activity and decreased insulin levels in culture supernatants with reduced β-cell insulin granules and enhanced insulin degradation by proteases. Finally, islet transplantations in mice showed delayed islet graft function when acinar cells were transplanted adjacent to the islets under the kidney capsule. The above studies indicated that autodigested acinar cells in pancreatic injury might also contribute to the low yield and impaired function in isolated islets. We believe that even if the impaired tissue perfusion and present hypoxemia are corrected before procurement, the autodigested islets are less likely to recover before islet isolation.
The absence of vasopressor usage is awarded a maximum of 15 points in the NAIDS. When a dose of one type of vasopressor exceeds a certain level, the use of an additional vasopressor is generally required. The need for concomitant use of vasopressors indicates hemodynamic instability, leading to the poor blood microcirculation in the donor pancreas and progressive pancreatic injury. Therefore, the use of multiple types of vasopressors is likely to result in lower islet yield.
If there are no unfavorable factors, 35 points are given. Although islets obtained from younger donors are functionally superior to islets from older donors, the technical challenges in obtaining purified high-quality islets are not overcome with lower donor age, especially below 20 years. Conversely, donors >70 years old are not considered an ideal donor since insulin secretory capacities deteriorate with increasing age 7 . Longer CIT significantly decreases postpurification islet recovery. Many investigators have found that the CIT shorter than 2 h had a negative impact on islet yield, although the mechanism is not clear (personal communications). Abnormally high values of ALT, AST, BUN, and amylase can be a result of multiple organ failure, wherein the pancreas is often involved. HbA1c >6.5% suggests the donor suffered from diabetes. It has been reported that islets isolated from type 2 diabetic donor pancreases had impaired islet function and lower islet yield 34 .
Favorable factors are given a maximum of 15 points. A procurement team at the same location as the isolation facility often provides higher quality organ recovery, which includes more efficient flush with preservation solution and cooling of donor pancreases after cross clamp, especially during multiorgan procurement. When the blood sodium level is elevated (>160 mEq/L) for a certain period of time, cell dehydration within the donor body occurs, and islets also become compromised. Even when the high blood sodium levels are corrected, the pancreatic injury may not be reversible. A study by Qi et al. 35 reported that hypernatremia is associated with reduced islet recovery postculture and diminished efficacy of islets when transplanted into diabetic mice. High blood glucose levels in the donor are indicative of islet dysfunction, and it is recognized as a negative factor in the scoring system.
Previous studies identified cardiac arrest as a negative variable, which was predictive of a low islet yield14,23. In contrast, our univariate logistic regression analysis resulted in a positive impact of the occurrence of cardiac arrest. It has been reported that the substantially increased risk of cardiovascular diseases is associated with patients being overweight or obese 36 . Therefore, a possible confounding relationship between the occurrence of cardiac arrest and high BMI might explain our unexpected finding. However, that was not the case. There was no statistical difference in BMI between cardiac arrest and the absence of cardiac arrest (29.4 ± 6.5 vs. 28.8 ± 6.5 kg/m2, p = 0.25, t-test). Our observation is most likely a statistical artifact created by the skewed distribution of frequency in cardiac arrest among the centers. In fact, the highest volume center (contributing 383 cases in the development cohort) exhibited 64% of cardiac arrest cases (122/190), and the center had the highest number of successful isolation cases (n = 131). This skewed distribution was also probably due to differences in interpretation of cardiac arrest across centers and may represent a reporting error. We recognize this as a limitation of our study.
Three additional limitations potentially existed in this multicenter study. First, we set the postpurification IEQ >400,000 as the target measurement for this study. After an optimal donor pancreas is received, there are several steps of the islet isolation procedure that may additionally affect the postpurification yield. Deviations or mistakes at any step can compromise the islet yield. We did not analyze the technical deviations in the isolation steps in participating centers. It is reasonable to assume that the rate of postpurification IEQ over 400,000 is higher in cases where the technical deviations or mistakes did not occur. Second, every islet center uses the same principle to count islets and to calculate the IEQ. However, technical deviations involved in IEQ counts may exist across participating teams. Deviations may occur during sample preparation, sampling methods, and the counting of islets. An overcounted IEQ may increase the successful islet isolation rate in the low NAIDS group. Conversely, an undercounted IEQ may decrease the successful islet isolation rate in the high NAIDS group. When all technical steps are better standardized and controlled, we would expect a better correlation between the NAIDS and postpurification IEQ >400,000. Finally, any deficiency in ice-cold protection of donor pancreases during procurement or transportation may result in warm ischemic injury. This kind of injury cannot be accounted for by the NAIDS since the injury is usually undetected or not recorded. In such cases, even donor pancreases with high NAIDS are highly susceptible to poor islet yield.
This study established the NAIDS based on data from 1,235 islet isolation cases in an international, multicenter database. The NAIDS shows the most important donor variables with quantitative scores. The application of the NAIDS will provide a useful point of reference for the selection of ideal pancreases for successful islet isolation and transplantation. In the current analyses, we did not analyze the predictive value of the NAIDS, as we did not want to set cutoff points for organ utilization. The NAIDS provides information of the chance of successful islet isolation based on the score and allows each individual center to set its own cutoff depending on the risk, logistic situation, funding available, and clinical scenario of the recipient. For example, centers with very limited funding or just starting the program may choose to focus on the best donor organs, for example, the NAIDS >80, and wait longer for availability of such optimal organs. After gaining the experience over time, they may choose to be more aggressive, lowering the threshold for the NAIDS, processing more organs, and transplanting more patients in a shorter period of time.
Apart from its utility in clinical decision making, the NAIDS may also be used in a research setting as a standardized measurement of pancreas quality.
Footnotes
Acknowledgments
The authors would like to thank Dr. Theodore Karrison (Director of Biostatistics Lab at the University of Chicago) for his advice on statistical analysis and Ms. Julissa Acevedo for her continued support in the establishment of the multicenter data entry in REDCap, University of Chicago. The authors also sincerely appreciate the database created by the REDCap project (grant support NIH CTSA UL1 TR000430), which is a reliable and user-friendly database. This study is supported in part by DRTC Grant No. P30 DK020595 to the University of Chicago. The authors declare no conflicts of interest.