
Abstract
We recently developed a promising regenerative method based on the xenotransplantation of human cartilage progenitor cells, demonstrating self-renewing elastic cartilage reconstruction with expected long-term tissue restoration. However, it remains unclear whether autotransplantation of cartilage progenitors may work by a similar principle in immunocompetent individuals. We used a nonhuman primate (monkey) model to assess the safety and efficacy of our regenerative approach because the model shares characteristics with humans in terms of biological functions, including anatomical features. First, we identified the expandable and multipotent progenitor population from monkey ear perichondrium and succeeded in inducing chondrocyte differentiation in vitro. Second, in vivo transplanted progenitor cells were capable of reconstructing elastic cartilage by xenotransplantation into an immunodeficient mouse. Finally, the autologous monkey progenitor cells were transplanted into the subcutaneous region of a craniofacial section and developed mature elastic cartilage of their own 3 months after transplantation. Furthermore, we attempted to develop a clinically relevant, noninvasive monitoring method using magnetic resonance imaging (MRI). Collectively, this report shows that the autologous transplantation of cartilage progenitors is potentially effective for reconstructing elastic cartilage. This principle will be invaluable for repairing craniofacial injuries and abnormalities in the context of plastic and reconstructive surgery.
Keywords
Introduction
Millions of patients are affected by craniofacial injuries and abnormalities, and conventional approaches to treat these defects rely on reconstructive materials, such as autocartilage, bone grafts, and synthetic materials (9,11,12,14,26). For autologous tissue grafting, limitations include the collectable volume, donor site morbidity, and tissue absorption; more importantly, the long-term clinical outcomes remain quite poordue to tissue maintenance failures (8,16,20). Furthermore, the implantation of synthetic materials is associated with a number of potential complications, such as inflammation, extrusion, calcification, and abnormal skin appearance (5).
Recently, we described the potential use of human auricular (ear) cartilage progenitor cells to regenerate self-renewing elastic cartilage with expected long-term tissue restoration, which may be used as an alternative grafting method for reconstructive surgery. Specifically, the presence of elastic cartilage progenitor cells was shown in the perichondrial tissue of the ear cartilage in a surrounding structure that wraps the chondrium layer in humans (6), mice (7), rabbits (18), and dogs (13). These progenitors possess robust expansion potential and high chondrogenic differentiation capacity, and after subcutaneous transplantation, they reconstruct fully mature elastic cartilage with a perichondrium layer that contains self-renewing progenitor cells (6). Compared with conventional stem cell sources such as bone marrow mesenchymal stem cells (1,15), ear perichondrium-derived progenitors are easily isolated using minimally invasive procedures and are associated with a much lower risk of unpleasant ectopic tissue formation, such as calcifications or fibrous tissue formation. Collectively, this cartilage-regenerative medicine technology utilized in clinics is highly promising in the context of craniofacial reconstructive surgery.
We have confirmed the feasibility of this regenerative principle of xenotransplantation using human cells in immunodeficient animals; however, whether autotransplantation may work as well as xenotransplantation remains unknown. For instance, a patient will normally provide an immunocompetent environment; hence, autoimmunity might affect transplanted cell survival, differentiation, and absorption, as described in several reports (4,17,25). Furthermore, demonstrating the validity of this procedure in a clinically relevant animal will provide meaningful information to assess the efficacy and safety of this approach and to examine the noninvasive, image-based evaluation of the presence of reconstructed cartilage tissue.
Here, we adopted a monkey model to assess the safety and efficacy of our approach in a preclinical study. Monkeys share multiple characteristics with humans in terms of anatomical and biophysical facial features, which significantly alter the transplant outcomes. First, we attempted to identify the progenitor population from the monkey ear perichondrium, which has not been previously characterized. The proliferative capacity and differentiation capacity of the in vitro expanded monkey progenitors were characterized and compared to human auricle-derived cells. The in vivo cartilage regenerative capacity of the isolated progenitor cells was validated via both xeno- and autotransplantation. Finally, the autologous monkey progenitor cells were transplanted into the subcutaneous region of a craniofacial lesion, and the regenerated tissue was monitored using noninvasive magnetic resonance imaging (MRI).
Materials and Methods
Animal Welfare and Ethical Considerations
The monkey study was conducted through the Cooperative Research Program at Tsukuba Primate Research Center, National Institute of Biomedical Innovation (Ibaraki, Japan). This study was conducted according to the Rules for Animal Care and Management of the Tsukuba Primate Research Center and the Guiding Principles for Animal Experiments Using Nonhuman Primates formulated by the Primate Society of Japan. The experimental animal protocols were approved by the Animal Welfare and Animal Care Committee of the National Institute of Biomedical Innovation (Osaka, Japan) (approval ID: DS25-32).
Experiments using mice and humans were conducted after moral justification was reviewed and administered by the moral board established by the ethics committee at Yokohama City University (Yokohama, Kanagawa, Japan) because this experiment involved the harvesting of human biological samples. We obtained written informed consent regarding the risks to the donor, privacy protection, and other considerations before the experiment. We harvested each biological sample at a medical institution (Department of Plastic and Reconstructive Surgery, Yokohama City University), placed the sample into a Petri dish with saline, and sent the sample to the research facility at the Department of Regenerative Medicine. The samples were anonymized before they were sent to the research facility; therefore, the samples and the matching patient names and information could not be determined, protecting patient privacy. The samples and personal data were used according to the Protection of Personal Information Act (Act No. 57 of 2003) as administered and updated accordingly by the moral board (Yokohama City University Graduate School of Medicine Hospital Approval No. 064, B090702029).
Isolation of Perichondrium From the Auricle
We harvested several parts of bilateral auricles from all the monkeys (Fig. 1A), and each wound was closed with sutures (4-0PDS II) (Johnson and Johnson, Tokyo, Japan), retaining the external auditory meatus. We exfoliated the skin abacterially, removed fat, vessels, and other tissues with scissors, and then performed blunt dissection between the perichondrium tissue and the cartilage tissue under a binocular loupe (Fig. 1C). Redundant auricular elastic cartilage isolated during surgery was received from all three microtia patients (15-year-old male: right microtia; 11-year-old male: left microtia; 11-year-old male: right microtia) involved in this experiment, and blunt dissection between the perichondrium tissue and the cartilage tissue under a binocular loupe was performed.

Harvested monkey auricular cartilage and isolated perichondrium. (A) Left: auricular cartilage before harvest (the white dotted line is the incision line), right: harvested auricular cartilage with skin measuring approximately 30 × 25 mm. Scale bars: 10 mm. (B) Staining with H&E (left), AB (middle), and EVG (right) confirmed elastic cartilage. Scale bars: 2 mm (top); 100 μm (bottom). (C) Left top: posterior side of the auricular cartilage after skin and subcutaneous tissue trimming. Left bottom: perichondrial tissue was manually dissected from the auricular chondrium. Right: magnification of left bottom (black dotted area: perichondrial tissue was overturned by forceps, gray dotted area: exposed auricular chondrium). Scale bars: 10 mm.
The following procedures were conducted similarly in both the monkeys and humans.
Primary Culture of Auricular Cartilage Progenitor Cells
We divided the tissue into the perichondrial and cartilaginous layers using scissors (ophthalmologic scissors; KEISEI Medical Industrial Co., Tokyo, Japan) and a scalpel (No. 15; FEATHER Safety Razor Co., Osaka, Japan) under a stereomicroscope (Keelar & Y. Na Ltd., Tokyo, Japan). Then dissected tissues were digested for 2 h at 37°C in phosphate-buffered saline (PBS; Wako Pure Chemical Industries, Osaka, Japan) containing 0.2% type II collagenase (Sigma-Aldrich Japan, Tokyo, Japan), to degrade the extracellular matrix and separate the cells. After passing through a 100-μm nylon mesh (BD Falcon, Franklin Lakes, NJ, USA), the cells were washed three times with PBS and centrifuged. Cell suspensions were cultured in Dulbecco's modified Eagle medium and Ham's F-12 medium (DMEM/F-12; Sigma-Aldrich Japan) supplemented with 10% fetal bovine serum (FBS; Gibco-Life Technologies Japan, Tokyo, Japan), 1% antibiotic/antimycotic solution (AMS; Invitrogen-Life Technologies Japan, Tokyo, Japan), and basic fibroblast growth factor (Fiblast spray®; Kaken Pharmaceutical Company, Tokyo, Japan), in 5% CO2 at 37°C. We passaged the cells using DMEM/F-12 containing 0.2% type II collagenase (Worthington Biochemical Corp., Lakewood, NJ, USA) to free them from the plate. The seeding concentration was set at 1,200 cells/cm2, and when confluency was achieved, passaging was repeated until the desired cell count was obtained.
In Vitro Chondrocyte Induction
For chondrogenic induction, when the cells were confluent, cells were detached and seeded into a 10-cm cell culture dish (FALCON; Ikeda Scientific Co., Tokyo, Japan). The cells were initially cultured in DMEM/F-12 supplemented with 10% good manufacturing practice (GMP) grade FBS (Lot: 6030111; Serana, Aidenbach, Germany), 1% antibiotic/AMS (Sigma-Aldrich Japan), and 10 ng/ml basic fibroblast growth factor. We later changed the media to chondrocyte differentiation medium. DMEM/F-12 supplemented with 1% antibiotic/AMS (Sigma-Aldrich Japan), ascorbic acid (vitamin C inj. 10% PBS; Nissin Pharmaceutical Company, Yamagata, Japan), dexamethasone (DEXART injection®; Fuji Pharma Company, Tokyo, Japan), 10 ng/ml basic fibroblast growth factor, and 650 μl insulin (Humulin R®; Eli Lilly Japan, Kobe, Japan) were used as the differentiation culture to induce cartilage differentiation. All culturing procedures were performed in a tissue culture incubator (Thermo Fisher Scientific, Waltham, MA, USA). Auricular perichondrium-derived cells were processed by papain (Wako Pure Chemical Industries) treatment before and after differentiation induction, and the glycosaminoglycan (GAG) levels were assessed via the Blyscan Assay (Biocolor, Antrim, UK) to evaluate the cartilaginous maturity.
Animal Surgical Experiments
Three female monkeys (Macaca fascicularis) were used in this study. The monkeys were 6.9, 9.8, and 10.5 years old at the beginning of the experiment. Inspection for infectious disease, such as simian varicella virus (SVV) and simian retroviruses (SRV), was conducted before the experiments (Table 1). All the animal surgical experiments were performed under general anesthesia. All the monkeys were fasted for 1 day before surgery. Atropine sulfate (0.05 mg/kg, IM; Mitsubishi Tanabe Pharma, Tokyo, Japan) was injected into the experimental monkeys preoperatively, and ketamine hydrochloride (10 mg/kg; Daiichi Sankyo Company, Tokyo, Japan) was used for sedation. Each monkey was intubated with endotracheal tubes according to their size, and the balloon was inflated. The ventilator was connected to a hose, and anesthesia was maintained using isoflurane (0.5–1.5%/50% oxygen; Sumitomo Dainippon Pharma, Tokyo, Japan) under mechanical ventilation. The blood pressure, electrocardiogram (EKG), SpO2, respiration rate, heart rate, CO2 concentration, and body temperature of each monkey were monitored every 10 min to assess the pain response, and anesthesia was maintained at the appropriate level. We used buprenorphine (0.012 mg/head; Nissin Pharmaceutical Company, Yamagata, Japan) postoperation, just before emergence from anesthesia, and for 2 days postoperatively for pain management. Cefazolin (250 mg/body, IM; Astellas, Tokyo, Japan) was administered before the operation and for 2 days postoperatively to prevent infection. We applied 10% Isodine gel (Meiji Seika Pharma, Tokyo, Japan) and 3% Actosin ointment (NIPROPATCH, Tokyo, Japan) once a day to the surgical site. During the experiment, the weight of each animal was maintained, and no abnormalities involving a decrease in activity were observed. Facial abnormalities and loss of appetite were observed temporarily and resulted from the use of the postoperative antibiotics and from the general anesthesia.
Characteristics and General Status of the Monkeys

SVV, simian varicella virus; SRV-WB, simian retroviruses, Western blotting; SRV-PCR, simian retroviruses, polymerase chain reaction.
Unexpectedly soft stool.
Xenotransplantation and Autotransplantation
For xenogeneic cell transplantation of monkey cells, we mechanically harvested the differentiation-induced progenitor cells from the dish with a cell scraper (As one, Osaka, Tokyo), collected them into a syringe, and attached an 18-gauge needle. Approximately 4.0 × 106 cells of differentiation-induced progenitor cells were transplanted with their generated cartilage extracellular matrix (ECM) as a vehicle into female mice at a subcutaneous site by injecting a total volume of 3–4 ml with syringe similar to our published methods (6). Three months after transfer, we removed only the reconstructed tissue. We used 18 female 6-week-old healthy immunodeficient mice [nonobese diabetic/severe combined immunodeficient (NOD/SCID) mice; Oriental Yeast, Tokyo, Japan]. Nine mice were injected with human-derived cells, and nine were injected with monkey-derived cells. Both groups were injected from three individuals as triplicates.
For autologous cell transplantation of monkeys, we removed the differentiation-induced progenitor cells from the dish using a syringe as described above. Transplanted cell numbers were estimated by evaluating the doublestrand DNA (dsDNA) levels of equivalent volumes of cell culture products with the PicoGreen® dsDNA quantitation assay according to the manufacturer's protocol (Thermo Fisher Scientific). A small incision was made into the supraorbital border, and the physiologically depressed forehead under the frontalis muscle/galea aponeurotica and above the periosteum was dissected. Approximately 1.0 × 108 cells were transplanted into the exfoliated area as described above, the wound was closed with sutures, and the transplanted cells were then retrieved 3 months later. Using a bicoronal approach, the region between the galea aponeurotica and the periosteum en bloc was removed, including the reconstructed cartilage-like tissue, and the skin was sutured to close the wound.
Clinical Evaluation
We took MRI images (3.0T system, Allegra; SIEMENS, Munich, Germany) before transplantation and 3 months after transplantation. We took T-weighted images (repetition time: 600 ms; echo time: 9.5 ms; slice thickness: 2 mm) and T2-weighted/proton density images (repetition time: 4,000 ms; echo time: 18 ms, 108 ms; slice thickness: 2 mm) by spinecho method under isoflurane inhalation anesthesia.
Histological Assessment of the Reconstructed Tissue (13)
The general parameters, such as wet weight and the projected area of the retrieved tissue, were measured. A portion of the tissue was processed by papain treatment, the disrupted cell suspension was retrieved, and the GAG levels were assessed via the Blyscan Assay to evaluate the cartilaginous maturity condition. We fixed the remaining tissue with 2% paraformaldehyde (Wako Pure Chemical Industries) at 4°C for 2 h. Then the paraformaldehyde was removed with 100 mM NH4Cl, (Wako Pure Chemical Industries) and the tissue was dehydrated with 15% and 30% sucrose (Wako Pure Chemical Industries) and was embedded with optimal cutting temperature (OCT) compound (Sakura Finetek Japan, Tokyo, Japan) to create a tissue-embedded block. Next, the tissue-embedded block was cut into 5-mm slices for hematoxylin and eosin (H&E) (Leica Biosystems, Nussloch, Germany), Alcian blue (AB) (Wako Pure Chemical Industries), and Elastica van Gieson (EVG) (Wako Pure Chemical Industries) staining.
Immunohistochemical Analysis (13)
The expression of cartilage-specific proteins was analyzed by immunohistochemistry. Sections embedded in OCT compound were washed with 0.1% Tween-tris-buffered saline (TBST) (Wako Pure Chemical Industries). After blocking with Protein Block Serum-Free (Dako Japan, Kyoto, Japan) for 2 h at 4°C, sections were incubated with the following antibodies for 3 h at 4°C: mouse anti-human type II collagen polyclonal antibody (1:200 dilution; Millipore Japan, Tokyo, Japan) and type I collagen polyclonal antibody (1:200 dilution; Acris Antibodies, Herfold, Germany). After washing three times, Alexa Fluor 488-conjugated (1:200 dilution; Thermo Fisher Scientific) and/or Alexa Fluor 555-conjugated secondary antibody (1:500 dilution; Thermo Fisher Scientific), specific for the appropriate species, was added, followed by incubation for 2 h at 4°C. Samples were counterstained with 1 μg/ml 4,6-diamidino-2-phenylindole (DAPI; Thermo Fisher Scientific). Samples were analyzed with a BIOREVO microscope (BZ-9000; Keyence, Tokyo, Japan).
In Vitro Adipogenic and Osteogenic Induction
We tested the adipogenic and osteogenic potential of perichondrocytes. We used the MSC adipogenic differentiation kit and the MSC osteogenic differentiation kit (both Lonza Japan, Tokyo, Japan), respectively
Statistical Analysis
For the statistical analysis, data are expressed as the median with quartile ranges from three independent experiments. Differences between two groups were analyzed using the nonparametric Mann-Whitney's U-test. Two-tailed values of p < 0.05 were considered significant.
Results
Isolation of Monkey Auricular Perichondrium-Derived Cells with High Proliferative Capacity
Initially, we collected bilateral auricular cartilage with skin measuring approximately 30 × 25 mm (Fig. 1A). The dissected primary auricular tissue was stained with H&E, AB, and EVG, confirming that the mature elastic cartilage was composed of both chondrium and perichondrium (Fig. 1B). The perichondrial tissue was manually dissected from the auricular chondrium in a similar manner as performed in humans (Fig. 1C), and 0.186–0.54 g (11–32% of the collected auricular weight) of perichondrial tissue was obtained. Subsequently, after collagenase treatment, viable cells were successfully isolated from the digested perichondrial tissues, and over 2.0 × 105 cells per gram were derived from monkey perichondrium (Table 2).
Grafted Volume of Auricular Cartilage and Perichondrium

The expansion culture of the primary auricular cartilage progenitor cells was then examined (Fig. 2A). As a control experiment, we prepared human progenitor cells, which were passaged similarly to the monkey progenitor cells (6). The progenitor cells derived from both species exhibited a similar growth rate from the passage day to the 7th day after passage (Fig. 2B). The doubling time was 43.3 and 43.0 for the monkey progenitor cells and the human progenitor cells as the median, respectively, and both species exhibited nearly the same growth potential in similar culture conditions. Both of them showed no significant difference statistically (Fig. 2C).

Monkey auricular perichondrium-derived cells with high proliferative capacity. (A) Cultured auricular cartilage progenitor cells. Scale bars: 400 μm. (B) Growth curve of monkey and human cartilage progenitor cells. Doubling times of monkey and human cartilage progenitor cells. Data are shown as the mean ± SD (n = 3) (blue: monkey, red: human). (C) Doubling times of monkey and human cartilage progenitor cells. Data are shown as the median with quartile ranges (n = 3) (white: monkey, gray: human). (D) Differentiation of progenitor cells. Scale bar: 400 μm. (E) Alcian blue staining of the injected cells [top: monkey, bottom: human. pre (left): before cartilage differentiation, post (right): after cartilage differentiation]. Scale bars: 400 μm. (F) GAG volume of the injected cells. Data are shown as the median, quartile ranges (n = 3 triplicate) (left: predifferentiation, right: postdifferentiation) (white: monkey, gray: human). *p < 0.05. (G) Adipogenic potential of monkey and human perichondrocyte-derived cells. Top: monkey, bottom: human. Perichondrocytes were stimulated in the adipogenic induction medium for 3 weeks. Adipogenesis was indicated by the accumulation of lipid vacuoles stained with Oil red O [pre (left): cartilage culture procedure, post (right): adipogenic assay procedure]. Scale bars: 50 μm). (H) Osteogenic potential of monkey and human perichondrocyte-derived cells. Top: monkey, bottom: human. Perichondrocytes were stimulated in the osteogenic induction medium for 3 weeks. Alizarin red S staining was used for the detection of osteocytes [pre (left): cartilage culture procedure, post (right): osteogenic assay procedure]. Scale bars: 100 μm.
In Vitro Chondrogenic Differentiation of the Monkey Auricular Perichondrium-Derived Cells
A high-density differentiation culture was utilized to determine the differentiation potential as assessed by morphological characterization using AB staining and the GAG assay. Chondrogenic differentiation was initiated immediately after achieving confluency in the culture (Fig. 2D). Exposure to differentiation medium made the cells smaller and more tightly packed. This culture method stimulated the cells to produce cartilage matrix, such as GAGs, making the medium extremely viscous. The differentiated cell types (post) stained well with AB compared to the monolayer cells (pre) (Fig. 2E). GAG increased after the high-density culture of both cell types. GAG increased 2.1-fold in the monkeys and 7.6-fold in the humans (Fig. 2F). Based on these data, we successfully established a monkey perichondrium cell culture system and extended the culture using the same differentiation protocol as used with the human cells.
In Vitro Adipogenic and Osteogenic Differentiation of the Monkey Auricular Perichondrium-Derived Cells
Multipotency, one of the essential features of stem cells, was tested by assessing the adipocyte and osteocyte differentiation. After 3 weeks of lineage induction, Oil red O and Alizarin red staining demonstrated the successful differentiation into adipogenic and osteogenic lineages, respectively, suggesting the multipotency of monkey progenitors, as observed in humans (Fig. 2G, H).
Xenotransplantation and Cartilage Reconstruction From Monkey Perichondrium-Derived Cells Into Immunodeficient Mice
We then tested the tissue regeneration capacity by subcutaneously transplanting differentiated cells into immunodeficient mice. Three months after transplantation, we collected the reconstructed tissue by cutting the mice's back skin and dissecting the tissue from a subcutaneous site. Gross observation confirmed the presence of reconstructed tissue, which was a highly elastic mass (Fig. 3A, B). Histochemical staining, including H&E (2nd row), AB (3rd row), and EVG (bottom row), showed the typical chondrocyte morphology packed in a lacunae with abundant elastic fibers and GAG, suggesting the formation of mature elastic cartilage. The volume of the reconstructed tissue was almost equivalent between monkey- and human-derived progenitors. The median weight of the reconstructed tissue was 30.0 and 83.3 (mg), the median maximum length was 5.87 and 9.69 (mm), and the median projected area was 15.6 and 39.3 (mm2), and all of these showed no significant difference statistically (Fig. 3C).

Xenogenic transplantation and cartilage reconstruction from monkey perichondrium-derived cells into immunodeficient mice. (A) Top: Schematic of injected perichondrium-derived cells in the subcutaneous area of the back of mice. Bottom: the detection of reconstructed tissue 3 months postinjection. (B) Reconstructed tissue (1st row) and staining with H&E (2nd row), AB (3rd row), and EVG (bottom row) confirmed elastic cartilage. Scale bars: 10 mm (reconstructed tissue), 1,000 μm (staining). (C) Reconstructed tissue weight, maximum length, and projected areas. Data are shown as the median, quartile ranges (n = 3) (white: monkey, gray: human).
Reconstruction of Elastic Cartilage From Autologous Perichondrium-Derived Cells
Finally, we assessed the elastic cartilage formation by autologous progenitors into a clinically relevant transplantation site (Fig. 4). Cultured monkey perichondrium-derived progenitors were injected into the forehead space of immunocompetent monkeys (Fig. 4A). The injected volumes in the three monkeys were 2.8, 6.0, and 1.8 ml, and the amounts of DNA were 320, 477, and 342 μg, respectively (Table 3). The surgical operation method did not differ among the three independent operations, and in all cases, dissection under aponeurosis and injection of the cultured perichondrium cells were successfully performed. No obvious adverse events, such as infarction or inflammation, occurred related to surgical procedures. A few months after the injection of the cultured perichondrium cells, marked enlargement of the lesion in the recipient was observed, and the tissue was firm on palpation, presumably due to the generation of elastic cartilage (Fig. 4C). To assess the cartilage formation by noninvasive clinical imaging, we conducted MRI on pre- and posttransplanted monkeys (Fig. 4B). A significant density difference was detected in the subcutaneous tissue of the forehead in the T1/T2 images, corresponding to the site of transplantation.

Reconstruction of elastic cartilage from autologous perichondrium-derived cells. (A) Schematic representation of our strategy. Cultured perichondrium cells injected into the forehead after dissection under the frontalis muscle/galea aponeurotica and above the periosteum (red dotted area). (B) MRI images. Clinical findings, T1-weighted images, and T2-weighted images with fat suppression. The arrow shows the augmentation section (left: preinjection, right: 3 months postoperation). (C) From top: clinical appearance before collection, intraoperative findings (black dotted area is reconstructed tissue), magnification, after trimming some of the other tissue. The arrow shows augmentation section. Scale bar: 10 mm. (D) Staining with H&E (top), AB (middle), and EVG (bottom) confirmed the presence of elastic cartilage. Scale bars: 10 mm (macro), 200 μm (micro). (E) Individual reconstructed cartilage weight, maximum length, projected area, and GAG amount of the reconstructed tissue and primary ear cartilage. light gray: #2 monkey, gray: #3 monkey, white: primary ear cartilage. GAG data are shown as the median with quartile ranges of three independent transplantation experiments for each individual. (F) Immunohistochemical staining of monkey primary and reconstructive cartilage. Scale bars: top 200 μm, bottom 400 μm. The matrix, which was neo-synthesized in the regenerated chondrium layer, showed strong collagen II deposition similar to primary ear cartilage, while the regenerated cartilage contained a collagen I-positive layer. DAPI, 4,6-diamidino-2-phenylindole.
Autologous Cell Transplantation
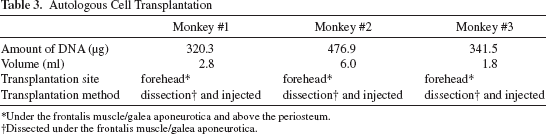
Under the frontalis muscle/galea aponeurotica and above the periosteum.
Dissected under the frontalis muscle/galea aponeurotica.
Three months after transplantation, we collected the reconstructed tissue and identified the tissue. The tissues were positively stained for AB and EVG, suggesting the regeneration of elastic cartilage, similar to xenotransplantation (Fig. 4D). The maximum size of the reconstructed tissue was 42 × 28 × 2.5 mm. Mature elastic cartilage with regenerated perichondrium was successfully reconstructed in all monkeys; however, individual differences were observed (Fig. 4E). For example, in monkeys #2 and #3, we observed marked enlargement and collected firm elastic tissue; in contrast, these characteristics were not apparent in monkey #1, but a small piece of elastic cartilage was confirmed after grafting. The process can be improved by surgical protocol optimization (Fig. 4A).
For further in-depth characterization of the cartilage matrices, the reconstructed tissues were treated with papain, and GAG was evaluated to confirm the production of a large amount of cartilage ECM deposition. Although the GAG amount was 65.0% (#2) and 91.3% (#3) of the primary auricular cartilage at 2 months post-transplantation, the tissue was located near the primary auricular cartilage and is expected to continue increasing to a comparable level of native, adult tissue, followed by a long-term transplant course (Fig. 4E). Furthermore, immunohistochemical staining of monkey primary and reconstructive cartilage was performed. The matrix, which was neo-synthesized in the regenerated chondrium layer, showed strong collagen II deposition similar to primary ear cartilage, while regenerated cartilage contained a collagen I-positive layer (Fig. 4F).
Discussion
The Use of a Larger Animal Model for Craniofacial Reconstruction
Autologous postnatal stem/progenitor cell transplantation is expected to be an invaluable approach to treat currently intractable diseases by restoring the function of damaged organs. In this context, cartilage is one of the primary target tissues for regenerative therapy due to its relatively simple structure. The promise of various tissue-derived mesenchymal stem cells has been shown in the context of hyaline (joint) cartilage regeneration in the orthopedic field. However, elastic cartilage regeneration in plastic surgery has not been effective, although the implantation of regenerated elastic cartilage may be a beneficial treatment for the reconstruction of craniofacial abnormalities.
Previously, we showed that elastic ear cartilage-specific progenitor cells reside in the outer layer of the perichondrium and presumably contribute to long-term tissue maintenance through their continuous self-renewal and differentiation capacities (6,7). Due to the unique nature of cartilage, future clinical use of cartilage regenerative therapy is anticipated. We confirmed that the xenotransplantation of human cartilage progenitors exhibited cartilage-regenerative potential, but it remains to be determined whether autotransplantation is effective for regenerating elastic cartilage in a preclinical animal model. One other limitation of our previous study was associated with the use of small rodent animal models (6,7). The anatomy of the skull bones of various laboratory animals, including mice, is very different from Homo sapiens; therefore, the effectiveness of transplantation experiments for future clinical use should be assessed in larger animals. In this context, the monkey craniofacial structure is equivalent to Homo sapiens, offering a superior model for transplant evaluation; therefore, we evaluated our proof of concept using a monkey model.
Identification and Differentiation of the Progenitor Cells of Monkey Ear Cartilage
To this aim, we first reported the successful isolation of cartilage progenitor cells from monkey auricular cartilage, which is located in the auricular perichondrium, similar to humans and mice. The monkey progenitor cells demonstrated a comparable doubling time to that of humans; therefore, the cells were propagated extensively ex vivo to provide a sufficient graft volume in vivo. The cells also showed a multilineage differentiation capacity into chondrocytes, osteocytes, and adipocytes, which is considered a standard criterion for mesenchymal progenitors.
Furthermore, the protocols for the chondrogenic differentiation of monkey progenitors were successfully adapted from humans (6). Specifically, high-density cultivation with exogenous differentiation factors stimulated the maturation of the progenitors into chondrocyte-like cells in vitro with a considerable amount of glycosaminoglycans, a major class of cartilage ECM molecules. Differentiated cells were subsequently transplanted into immunodeficient mice, confirming the elastic cartilage reconstruction 3 months after transplantation. Reconstructed tissues were composed of bilayer structures, as observed in the native cartilage, and the chondrium and perichondrium layers suggested the presence of progenitor cells in the regenerated perichondrium. Monkey progenitors are predicted to be efficient for a variety of preclinical studies in a clinically relevant transplantation model, not only in plastic surgery but also in orthopedic surgery, because we have demonstrated their differentiation capacity into hyaline cartilage in vivo (13).
Reconstruction of Autologous Elastic Cartilage by Autotransplantation
Finally, we transplanted the autologous progenitor cells into the forehead of the monkeys, which is a physiologically depressed region. Both the periodical MRI measurements and the histological analysis of the harvested grafts showed that the reconstructed elastic cartilage was successfully regenerated into the physiologically depressed region even under immunocompatible conditions, unlike in immunodeficient mice. One limitation of this study includes the lack of a disease-specific transplantation model with fractures or punctures of the facial bones because invasive procedures in the monkey were not justified at the beginning of this study due to the ethical considerations. Nevertheless, we are still convinced that our approach would be highly effective for correcting deformities, such as deletions without bone/cartilage, which would have much lower tension than intact tissue, preventing the dispersion of the transplanted cells. Thus, we succeeded in reconstructing autoelastic cartilage in the face using autotransplantation of cartilage progenitor cells into the subcutaneous area. Reconstituted perichondrium will be expected to contain self-renewing progenitors and thus contribute to long-term tissue restoration.
MR images have several good properties. First, MR images can detect the reconstructive tissue without having to collect it. Second, MR images are superior to other modalities in important ways. Some other modalities, such as echo and computed tomography (CT), also detect reconstructive tissue, but echo images have some objective problems and CT images cannot detect cartilage tissue. Exposure to radiation is also a problem with CT imaging. We can adapt this method to humans to check the reconstructed tissue conditions.
Safety Evaluation Associated with Cell Transplantation
Tumorigenicity is one of the most important concerns in the field of stem cell-based therapeutics. In conventional reports, tumorigenicity is typically evaluated using soft agar nutrient medium and by comparative genomic hybridization (CGH) examination (3); however, identifying reliable risks of tumorigenicity with these methods remains challenging. Therefore, a subcutaneous transplant experiment system specific for the type of animal is the prevailing approach in place of using cultured cell groups. Indeed, mesenchymal stem/progenitor cells, which are an upstream lineage of cartilage progenitor cells, have been closely examined both in preclinical and clinical studies (1,20–24). We did not identify previous reports regarding the identification of tumorigenicity using extended culture or transplantation experiments, but recently tumorigenicity examination was decided gradually (3). We thus followed the protocol of clinical studies in humans and monkeys to properly apply the cultivated cartilage progenitor cells and to assess the tumorigenicity upon transplantation. Up to 10 months posttransplant in mice, there was neither obvious tumor formation nor ectopic tissue formation associated with human cell xenotransplantation (6) or monkey cell autotransplantation (unpublished observation). Thus, the risks for developing uncontrollable tissue formation are extremely minimal within the current investigation standards, but we need to consider this issue in future clinical studies.
Clinical Prospects
There are several clinical applications for cartilage reconstruction: cell-based therapies [autologous chondrocyte implantation (ACI) and MSC implantation], biological scaffolds, and their combinations, which are mostly investigated in joint cartilage repair (10). On the contrary, in plastic and reconstructive surgery, autocartilage, bone grafts, and synthetic materials (9,11,12,14,26) are commonly used for craniofacial deformities. Recent pioneering efforts include ear and nose reconstruction by using autologous mature chondrocytes isolated from ear or nasal chondrium rather than perichondrium layer (2,19,24). Thus, although there are several preexisting methods to generate elastic cartilage, no reports evaluated the promise of autologous progenitors for regenerating cartilage.
Aiming at future clinical studies, we will first target the disease to a relatively small and simple range of craniofacial abnormalities, such as 2.5-mm thickness defects in plastic surgery, before examining more complicated cases, such as microtia or pectus excavatum. We have also confirmed that our progenitor cells can be stored using simple freezing methods (Cellbanker2; LSI Medicine, Tokyo, Japan) (unpublished data), which will allow multiple injections, in accordance with the morphological changes of the deformed region by postnatal growth.
To make a much larger defect, such as an auricular shape in the microtia case, we generally collect the unilateral Nos. 6, 7, and 8 costal cartilages (14) and require approximately 6 cm length × 3 cm width × 2 cm thickness size and 6 g weight costal cartilage for reconstructing the auricular framework. In these complicated cases, we have to consider the two-stage operation reported by Yanaga et al. (21–23). Initially, a large number of differentiated cells are transplanted into the lower abdomen skin, followed by a secondary grafting into the actual affected tissue using a reconstructed cartilage graft. The inspection of the correlation between the injected cell quantity and the reconstructed cartilage quantity is insufficient and needs to be addressed in a future study, especially when we consider the two-stage operation. Overall, we conclude that the use of autologous cartilage progenitor cells is highly promising to treat craniofacial deformities in plastic and reconstructive surgery.
Footnotes
Acknowledgments
We thank M. Mizuno, A. Toi, C. Kawakami, M. Oishi, M. Masutani, and N. Sasaki for technical support and all the members of our lab for performing the experiments and providing comments. We also thank K. Yasumura, S. Matsubara, S. Kitayama, E. Adachi, K. Hasegawa, M. Shinoki, S. Haga, M. Kobayashi, and C. Okouchi and all the plastic and reconstructive surgery department members for kindly helping with several experiments and providing comments. Finally, we are grateful to I. Itagaki, Y. Katakai, H. Shibata, and Y. Yasutomi for the animal experiments. This work is supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology (MEXT) to T. Takebe (Nos. 24106510, 24689052, and 24659785), Y. Yabuki (No. 24791911), S. Kobayashi (No. 20592101), and T. Takebe by the Health and Labor Sciences Research Grants Research (No. 12103252). This work was also supported by a grant for Research and Development Project III (No. 22) from Yokohama City University, Japan. Drs. Takebe and Taniguchi have served on a scientific advisory boards for Healios Inc. The authors declare no other conflicts of interest.