
Abstract
Platelet gel derived from peripheral blood is widely applied in many clinical fields of surgery as biomaterial containing growth factors with high proliferative properties. In 2010, we studied and patented a platelet gel derived from cord blood. In this study, due to the crucial role of the factors released by the platelet gel, we first extended the characterization of its releasate. Using a wide proteomic array and splitting the two components of the releasate, that is, platelets and plasma, we have been able to study their growth factor content. Interestingly, we discovered high levels of hormones and molecules able to support tissue growth in the cord blood platelet gel releasate and, in addition, higher concentrations of several angiogenic factors if compared with the peripheral blood counterpart. On the contrary, the latter was much richer in inflammatory factors. The second aim of our work was to study the effects on cell culture, immunophenotype, and function of mesenchymal stem cells exposed to these two platelet gel releasates as substitute for the animal serum. Since our findings nicely show that the use of the peripheral versus the cord blood platelet gel releasate can differently influence the mesenchymal stem cell commitment, we can suggest that in addition to its peculiar angiogenic properties cord blood platelet gel releasate shows excellent proliferative properties as cell culture supplement.
Keywords
Introduction
There is a growing interest in the topical use of human platelet-based biomaterials, such as platelet gel (PG), in regenerative medicine. Several fields already obtained beneficial clinical outcomes from the use of PG, in particular, dentistry, oral-maxillofacial and bone surgery, wound healing, and soft tissue injuries (1,30).
The PG is composed by platelets containing biofactors that trigger important actions for healing and hemostasis and by plasma (also mentioned as platelet poor plasma, PPP), which contains fibrinogen and other agents (27). The therapeutic effects of PG are attributed primarily to the release of platelet growth factors (such as platelet-derived growth factor-BB, transforming growth factor-β1, fibroblast growth factor-basic) contained in the α-granules, which exhibit chemotactic and mitogenic properties promoting tissue regeneration and cell proliferation (3,22). However, other authors hypothesize that the fibronectin content that comes with the platelet-rich plasma (PRP) preparation may exert an extra bioactive effect to the cells/tissues, such as matrix metalloproteinase activation (32).
Usually PG is obtained from platelets derived from peripheral blood (PB) (29), and recently our group developed and patented a procedure to obtain PG from human umbilical cord blood (CB) (PCT WO/2010/007502). It is well known that CB is an innovative source of hematopoietic and mesenchymal stem cells (MSCs), and CB banks have been established worldwide for CB storage (5). We demonstrated that CBPG contains factors more prone to support soft tissue repair if compared to PBPG (37). These factors are released by the platelet concentrate forming the PG, which is called PRP. In the literature, there are several studies regarding the use of PRP on MSC culture. MSCs are adult stem cells that are responsible for the maintenance and repair of mesodermal tissues (6). Commonly, MSCs are isolated from bone marrow and from other sources such as adipose tissue (AD) (25) and umbilical cord blood (CBMSCs) (31,50), and they are considered the cell of choice in a clinical setting of regenerative medicine. However, to achieve efficient results in some tissue injuries, a large number of MSCs is necessary, which may require expansion via ex vivo cell culture. In this sense, the use of fetal bovine serum (FBS) should be minimized because proteins from ruminant materials have been implicated in prion transmission, and their use is not highly recommended by European legislation (48), except after additional and extensive investigations. In this context, serum substitutes are desirable for an easier translation of MSCs to clinical use, and PBPG has been recently considered as a valid alternative (18). In addition, it is important to emphasize that numerous reports are showing how important and relevant is the use of sera or substitutes to modulate the differentiation of stem cells (26,28), and therefore, the use of these new supplements should be extensively investigated. Finally, the use of PGs is becoming very emergent in the field of tissue engineering for their peculiar properties as resorbable biomaterial rich in growth factors (4).
Previously, we have demonstrated that CBPG possesses interesting tissue regeneration properties (40). In this study, we have showed the in vitro potential of CB platelet gel releasate (PR) on MSC cultures as a serum substitute. Moreover, we characterized the CB-PR proteomic profile compared with the PB counterpart in order to better identify future appropriate clinical applications.
Materials and Methods
Sample Collection
CB was collected from healthy male newborns (n = 19) in plastic bags containing 29 ml of citrate–phosphate–dextrose anticoagulant (Macopharma, Mouvaux, France) after informed consent and by trained midwives in vaginal deliveries and cesarean sections (41). All the CB collections were performed only after successful deliveries from healthy newborns with Apgar scores between 9 and 10. Buffy coats were obtained, according to standard blood banking practices, from standard 450-ml whole blood units donated for transfusion purposes by healthy male donors (n=5; age 25-50 years) after informed consent. Both cord and peripheral blood units were processed within 24 ± 2 h of collection to isolate platelets.
Adipose tissue (5 ml) was collected from the lower abdomen of three healthy female donors (age 25-50 years) after informed consent and the Ethics Committee approval and processed within 5 h from lipoaspiration (25).
Platelet Gel Releasate (PR) and Platelet Lysate (PL) Preparation
A single CB or PB buffy coat unit was centrifuged for 10 min (550 × g) to obtain a PRP unit. Then the PRP was centrifuged for 10 min (2,000 × g) to obtain a platelet pellet. This platelet fraction was diluted in an appropriate volume of supernatant PPP to obtain a final concentration of 2 × 106 platelets/μl. Successively, the sample was allowed to rest for 30 min at room temperature and, subsequently, activated. The activation was performed with calcium gluconate and batroxobin (Plateltex-Act; Plateltex, Bratislava, Slovakia). The gel consolidation was completed in approximately 10 min. The PG was centrifuged for 10 min (2,000 × g) to obtain the PR that was used for further investigations.
To obtain PL, a different technique was employed The platelet pellet obtained after PRP centrifugation was diluted in an appropriate volume of phosphate-buffered saline (PBS; Macopharma) to a final concentration of 2 × 106 platelets/μl. Then the platelets were subjected to three cycles of freezing at −80° and thawing at 37°C, and they were centrifuged at 2,000 × g to obtain the PL. Study design is represented in Table 1.
Study Design
Inflammatory Profile
The inflammatory profile was analyzed in CB plasma from vaginal delivery (n=7) and from caesarean section (n=7). The inflammatory cytokines were detected by a multiplexed sandwich ELISA (SearchLight Human Inflammatory Cytokine Array 4; Aushon Biosystems, Billerica, MA, USA) that allows quantitative chemiluminescent measurement of four proteins per well: interleukin-1β (IL-1β), IL-6, interferon-γ (IFN-γ), and tumor necrosis factor-α (TNF-α). To identify the signal, SuperSignal ELISA femto chemiluminescent substrate (Pierce, Rockford, IL, USA) was used. The luminescent signal was acquired within 10 min using a cooled CCD camera, and the amount of each target protein was obtained following the manufacturer's recommendations.
Proteome Array
The protein profiling of PB-PL (n = 2), CB-PL (n = 2), and of their PPP was analyzed using a commercially available multiplexed immunoassay system (RBM, Austin, TX, USA) based on Luminex xMulti-Analyte profiling (MAP) platform (52).
Starting from a 500-μl sample, a panel of 188 protein biomarkers comprising cytokines, inflammatory markers, and growth factors was quantified using the DiscoveryMAP™ v1.0 multiplex immunoassay system (list of markers: http://www.rulesbasedmedicine.com/products-services/humanmap-services/human-discoverymap).
Angiogenic Assay
In this assay, the CB/PB-PR (diluted in the culture medium as supplementation) was tested on a model of angiogenesis where the human endothelial cells were cocultured with human interstitial cells at the earliest stages of tubule formation for 11 days (n=3; AngioKit; TCS CellWorks Ltd., Buckingham, UK).
To identify endothelial structures/morphology, the monolayers, previously exposed to CB/PB-PR, were then fixed and stained with endothelial markers such as CD31 and von Willebrand factor (AngioKit). A known angiogenic stimulator [vascular endothelial growth factor (VEGF) at 5 ng/ml] and an angiogenic inhibitor (suramin at 10 μg/ml) were included as positive and negative controls, respectively.
ADMSC Isolation and Culture
Samples of lipoaspirate obtained from three healthy subjects were aseptically collected in syringes and transported to our laboratories at controlled temperature. Soon after, the lipoaspirate was transferred into a modified Top&Bottom triple bag (Fresenius Kabi, Bad Homburg, Germany), diluted, and centrifuged with sterile PBS to discard red blood cells. Then the sample was digested for 40 min at 37°C with NB6 Good Manufacturing Practice-grade collagenase (Nordmark Arzneimittel GmbH&C, Uetersen, Germany). The digestion was stopped using PBS and 10% FBS (Australian origin, γ-irradiated; Gibco Invitrogen Corporation, Carlsbad, CA, USA). After centrifugation (1,185 × g for 30 min) to discard the solid fat phase, the stromal vascular fraction was seeded into a one-layer cell stack (Macopharma) in a complete medium (aMEM, 10% FBS; Macopharma). After 24 h, the nonadherent fraction was removed, and adherent cells were cultured in complete medium.
The cultures were maintained at 37°C in a humidified atmosphere containing 5% CO2 from passage 0 (P0) to P3 in order to establish the culture, and the medium was changed twice a week. The ADMSC lines were passaged after detachment (TryPLE Select; Gibco) and counted once they reached 80% confluence until P3.
From P3 when the cell population was homogenous with no hematopoietic contamination, ADMSCs (n=3) were cultured in αMEM containing (A) 10% CB-PR, (B) 10% FBS, (C) 10% PB-PR. The medium was changed twice a week.
At the end of each passage, ADMSCs cultured under these conditions were harvested, counted, and the population doubling (PD) rate was determined using the following formula:

N is the ratio between the harvested cells and the seeded cells. The PD for each passage was calculated and added to the PD of the previous passages to generate data for cumulative PD.
Flow Cytometry
ADMSCs were extensively characterized by flow cytometry during A and B culture conditions (n=3). The cells were washed in PBS for 20 min at room temperature and incubated at a concentration of 100,000 cells per tube with the following directly conjugated mouse anti-human antibodies: CD90 FITC (dil. 1:75; Becton Dickinson Pharmigen, BD, San Jose, CA, USA), CD105 PE (dil. 1:15; BD), CD73 PC5 (1:15; Miltenyi Biotec, Bergisch Gladbach, Germany), CD45 PC7 (dil. 1:15; Beckman Coulter, Krefeld, Germany), PDGFR-β PE (dil. 1:15; R&D Systems, Minneapolis, MN, USA), HLA-ABC FITC (dil. 1:15; Beckman Coulter), HLA-DR PE (dil. 1:15; Beckman Coulter). After staining, the cells were washed once with PBS. For each sample, at least 50,000 list mode events were acquired using a Cytomics FC500 (Beckman Coulter).
Cell Differentiation Capacity
At P3 and P5, total RNA was extracted from ADMSCs in conditions A, B, and C (n = 3) using the RNeasy Mini Kit (Qiagen AG, Hilden, Germany) according to the manufacturer's instructions. RNA purity was determined by measuring absorbance A260/A280 in a Nanodrop spectrophotometer (ND-1000; Celbio Spa, Milan, Italy). Reverse transcription was carried out using iScriptTM cDNA Synthesis Kit (Bio-Rad Laboratories Ltd., Hemel Hempstead, Herts, UK). Real-time PCR was performed on a CFX96 Real Time System using Sso FastEva Green Super mix (Bio-Rad), according to the manufacturer's instructions.
The expression of the following genes was studied. CCAAT/enhancer-binding protein β are genes that are actively expressed very early during adipogenic differentiation: CEBPβ (F: GACAAGCACAGCGACGAGTA, R: AGCTGCTCCACCTTCTTCTG) and CDBPΔ (F: GA CCGTGGTGAGCTTGGCGG, R: TCTTGCCGGCGCTCTTCTCC); genes involved in osteogenic differentiation: runt-related transcription factor 2 (RUNX2) (F: AAGGCTGCAAGCAGTATTTACAA, R: CTCGGATCCCAAAAGAAGTTTTGCT) and MSX2 (F: ATTCGCCGCC GCCAAGACA, R: AGGGCGAGGAGCTGGGATGT); and gene correlated to chondrogenic differentiation: type 10 collagen α1 (COL10A1) (F: ACTCCCAGCACGCAGAATCCA, R: TGGGCCTTTTATGCCTGTGGGC).
Ribosomal protein large P0 (RPLP0) (F: TGTGGGCTCCAAGCAGATGCA, R: GCAGCAGTTTCTCCAGAGCTGGG) and ribosomal protein L13a (RPL13A) (F: GGCTTTCCTCCGCAAGCGGAT, R: GCAGCATACCTCGCACGGTCC) gene expressions were used as controls (38).
After A, B, and C culture conditions, the ADMSC potential to differentiate toward other tissues was evaluated by staining assays (n=3).
Adipogenic Differentiation
Cells were plated in six-well culture plates (Falcon; Corning Incorporated, USA) at 2.1 × 104 cells/cm2 in αMEM containing 10% FBS, and once they reached the confluence, they were cultured for 2 weeks in the presence of human MSC adipogenic induction medium (Lonza S.p.A., Milano, Italy). Medium was replaced every 3-4 days for 15 days. Cells were stained with Oil red O solution (Sigma-Aldrich, St. Louis, MO, USA), in order to detect the presence of lipid vacuoles.
Osteogenic Differentiation
Cells were plated in six-well culture plates at 2.1 × 104 cells/cm2, and they were grown for 2 weeks in the presence of human MSC osteogenic medium (Lonza). Osteocytes were stained with Alizarin red (Sigma-Aldrich) in order to detect the presence of calcium deposits.
Chondrogenic Differentiation
Cells (2.5 × 105) were centrifuged in a polypropylene tube (Falcon) at 150 × g to form a pellet. Without disturbing the pellet, the cells were cultured for 3 weeks in the complete chondrogenic differentiation (Lonza) medium including 10 ng/ml TGF-β3 (Lonza). The medium was changed twice a week. To examine chondrogenesis, the micromass pellets were embedded in Tissue-Tek with OCT compound (Sakura Finetek, Torrance, CA, USA) and then frozen in liquid nitrogen and cryosectioned (6 μm thickness). For the cartilage-specific proteoglycan examination, these sections were stained with Alcian blue (Sigma-Aldrich) (47).
Quantitative Telomerase Detection
The level of telomerase was detected in P3 ADMSCs cultured in standard conditions versus P5 ADMSCs in all the three different conditions (A, B, C) (n=3) using a quantitative telomerase detection kit (QTD Kit; Allied Biotech Inc, Ijamsville, MD, USA) according to the manufacturer's protocol for qPCR. Briefly, the activity of telomerase was measured from 2 × 105 lysed ADMSC. The analysis of each sample consists of two assays: one with a test extract and one with a heat-treated test extract (85°C for 10 min) used as negative control. In the first part of the analysis, the active telomerase added telomeric repeats (TTAGGG) onto the 3’ end of the oligonucleotide substrate in vitro upon the addition of the appropriate buffer conditions and dNTPs. In the second part, these extension products were then amplified by PCR and detected by measuring the increase in fluorescence caused by binding of SYBR Green to double-strand DNA. In addition, the kit provided the control template for quantitative analysis of the samples, and HeLa cells (CCL-2; www.atcc.org) were used as positive control.
Clonogenic Potential
The fibroblastic colony-forming unit (CFU-F) assay was performed on ADMSC (n=3) to determine the clonogenic capacity in the different conditions (A, B, C). For optimal counting of colonies, ADMSC at P5 were seeded at 1-2 cells/cm2 in duplicates in 58.9-cm2 culture Petri dishes (Corning Life Technologies, MA, USA). The cells were cultured in αMEM with 10% FBS/CB-PR/PB-PR, respectively, and the medium was changed every 3-4 days.
After 2 weeks, ADMSCs were washed, fixed with methanol (Sigma-Aldrich), and finally visualized using crystal violet (Sigma-Aldrich). Then ADMSC clonogenic precursors were scored macroscopically considering only the clusters of more than 50 cells as a colony.
Statistical Analysis
The data were analyzed by unpaired t-test using the Bonferroni method to correct for multiple comparisons to determine the p value. The results are expressed as the mean ± standard deviation. Statistical significance level was accepted as p < 0.05.
Results
Platelet Gel Proteomic Profile
The ELISA assay for the most common inflammatory factors (HL-1β IL-6, IFN-γ, TNF-α) did not show any significant difference (p > 0.05) between plasma obtained from CB collected after vaginal and cesarean deliveries (Fig. 1A). Subsequently, an explorative and extensive multianalyte profiling (188 biomarkers) was performed on the two components of PG, that is, CB/PB-PPP and CB/PB-PL. In order to choose only the factors that were highly significantly different, a cutoff obtained from twofold ratios was applied. Interestingly, as shown in Table 2, CB-PPP and CB–PL contain higher concentrations of hormones and molecules related to pregnancy and fetal growth such as α-fetoprotein and prolactin than the PB counterparts. Moreover, we observed that two groups of biofactors (angiogenic and inflammatory) gave the major differences where CB had higher concentrations of angiogenic factors (resistin, prolactin, VEGF, growth hormone, trefoil factor 3, erythropoietin) than PB. Instead, PB was richer in inflammatory and immunomodulatory factors (chemokine HCC-4, CD5 antigen-like, matrix metalloproteinase-3, RANTES, IgA, IgM) than CB (Table 2).

Inflammatory profile and angiogenic potential of platelet gel. (A) Inflammatory factors were quantified in CB plasma collected from vaginal (black) and cesarean (gray) deliveries (y-axis: pg/ml; media and DS). The p value was obtained by performing an unpaired t-test (p > 0.05). (B) The angiogenic potential of CB/PB-PR was tested on human endothelial cell culture. Suramin and VEGF represent CTRL- and CTRL+, respectively. Scale bars: 10 μm.
Proteomic Profile
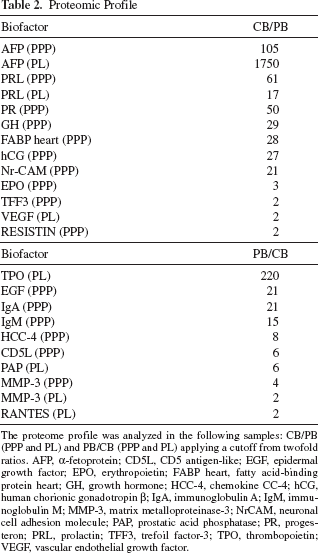
The proteome profile was analyzed in the following samples: CB/PB (PPP and PL) and PB/CB (PPP and PL) applying a cutoff from twofold ratios. AFP, α-fetoprotein; CD5L, CD5 antigen-like; EGF, epidermal growth factor; EPO, erythropoietin; FABP heart, fatty acid-binding protein heart; GH, growth hormone; HCC-4, chemokine CC-4; hCG, human chorionic gonadotropin β; IgA, immunoglobulin A; IgM, immunoglobulin M; MMP-3, matrix metalloproteinase-3; NrCAM, neuronal cell adhesion molecule; PAP, prostatic acid phosphatase; PR, progesteron; PRL, prolactin; TFF3, trefoil factor-3; TPO, thrombopoietin; VEGF, vascular endothelial growth factor.
Interestingly, PB platelets contain a classical platelet factor such as thrombopoietin that is present even 220-fold more than in CB platelets (Table 2).
Platelet Gel Angiogenic Potential
The angiogenic potential of CB and PB-PR was tested using a classical assay on human endothelial cell culture. During the first days, in the presence of these platelet gel releasates in culture medium, the endothelial cells formed small islands; then they started proliferating and moving through the culture matrix to form threadlike tubule structures. These gradually joined up to form a network of anastomosing tubules. After 11 days, the development of capillary-like structures was observed in both conditions by staining with CD31 and von Willebrand factor.
Results showed that the addition of CB-PR to culture medium produced an increased number of endothelial junctions compared to the use of PB-PR (Fig. 1B), and they were morphologically similar to networks formed by the positive control (VEGF). No tubule formation was visible in the negative control, whereas the positive control showed a dense tubule network.
ADMSC Morphology, Clonogenic and Proliferative Capacity
ADMSCs were cultured using a medium supplemented with A, B, and C, and during the culture they showed a fibroblastic shape with more elongated morphology when treated with conditions A and C (Fig. 2A). Therefore, ADMSC images were processed for measuring length, width, and cell elongation index (CEI) by the image program. CEI is defined as the ratio of cell length to cell width. The ADMSCs treated with CB-PR (6.89 ± 2.42) and PB-PR (7.38 ± 2.20) were slimmer than ADMSCs in FBS (3.33 ± 1) (Fig. 2B).
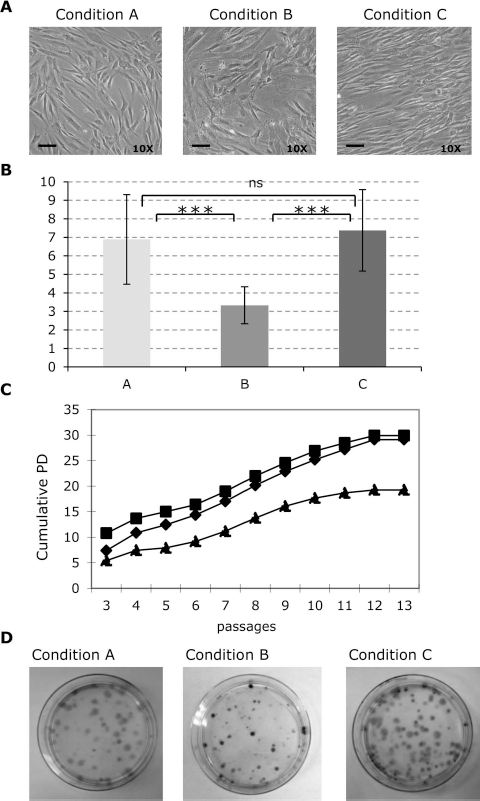
Morphology and growth of ADMSCs. (A) ADMSC morphology at P5 in αMEM + 10% CB-PR (condition A) or + 10% FBS (condition B) or + 10% PB-PR (condition C). Scale bars: 10 μm. (B) Cell elongation index was calculated on three pictures of ADMSCs for each culture condition; 10 ADMSC measurements were taken for each picture. CEI ratio was reported on the y-axis. The p value was obtained by unpaired t-test (*p < 0.001 in comparison with B condition). (C) Cumulative PD was calculated on ADMSCs in the three culture conditions. Square (condition A), triangle (condition B), lozenge (condition C). (D) CFU-F assay was performed in ADMSCs after the three culture conditions.
To examine the possible influence of different culture conditions on cell proliferation, the cumulative PD levels were determined in ADMSC culture until plateau phase; a representative example of cumulative PD on a single ADMSC batch in the three culture conditions is reported in Figure 2C. In particular, ADMSCs in condition A had a similar proliferative trend as ADMSCs cultured in condition C, and ADMSCs in condition A showed a higher proliferation in comparison with ADMSC in the presence of FBS (30 CPD vs. 19 CPD, respectively).
At P5, the CFU-F frequency of ADMSCs under different culture conditions was 10.8% in A (p < 0.05 vs. B), 5% in B, and 10.5% in C (p < 0.05 vs. B). Moreover, colony size and density of CFU-F were much higher in conditions A and C than in B (Fig. 2D).
In addition, to evaluate possible tumorigenic modifications during ADMSC passages due to the presence of different supplements, the telomerase activity was analyzed. ADMSCs did not show any modification during passages in all the culture conditions. In addition, all of them showed much lower concentrations of telomerase (molarity, M) compared with HeLa cells (positive control) (steady state: 1.29 × 10-11 M; A: 1.22 × 10-11 M; B: 3.45 × 10-11 M; C: 1.49 × 10-12 M; HeLa: 1.57 × 10-6 M).
ADMSC Phenotypical Characterization
ADMSCs grown in conditions A, B, and C were analyzed at P5 for their phenotype to confirm their MSC features. By flow cytometry, they were found to express the typical human MSC surface antigens, represented as median fluorescence intensity ratio. It was calculated as ratio between mean fluorescence intensity of the stained sample and its corresponding isotype control ± standard deviation (MFI-R ± DS), such as CD73 (A: 42 ± 11; B: 81 ± 56; C: 64 ± 4), CD90 (A: 111 ± 1; B: 135 ± 45; C: 157 ± 17), CD105 (A: 75 ± 0; B: 72 ± 27; C: 42 ± 4), and HLA-ABC (A: 11 ± 0; B: 12 ± 0; C: 18 ± 0). The cells were negative for hematopoietic markers such as CD45 (A: 1 ± 0; B: 1 ± 0; C: 1 ± 0) and HLA-DR (A: 1 ± 0; B: 0 ± 0; C: 1 ± 0). The only relevant difference was observed for the PDGFR-β expression where ADMSC cultured in A and C showed a statistically higher MFI-R of PDGFR-β (30 ± 12 and 35 ± 8) in comparison with B condition (12 ± 7) (p < 0.05).
ADMSC Functional Characterization
An initial molecular characterization was performed on ADMSCs at P3 (steady state) and on ADMSCs cultured in A, B, and C conditions at P5 to analyze the influence of different supplements on the commitment. No significant differences were found between ADMSCs in steady state and ADMSCs in B condition at P5.
At P5, the expression of MSX2 and RUNX2 genes was higher in ADMSCs cultured in the presence of PB-PR with respect to FBS (3.5- and 1.6-fold, respectively), while CEBPβ, CEBPΔ, and COL10A1 did not show any significant difference within the three groups (Fig. 3A).

Differentiation capacity of ADMSC. (A) Comparative gene expression of ADMSC in A (gray) and C (white) conditions with respect to B condition at P5 (n = 3; media and SEM). The p value was obtained by unpaired t-test (*p<0.05 in comparison with B condition). (B) Adipogenic, osteogenic, and chondrogenic differentiations of ADMSC in all the three conditions (A, B, C). Scale bars (10x): 10 μm; (20x): 20 μm.
Differentiation capacity into osteogenic, adipogenic, and chondrogenic lineages was assayed using commercial and standardized media on ADMSC at P5 (Fig. 3B). No difference was observed within the three groups: ADMSCs were able to differentiate into osteoblasts, as demonstrated by the histological detection of calcium deposition stained with Alizarin red (Fig. 3, osteogenic differentiation), into adipocytes, as revealed by the formation of lipid droplets, stained with Oil red O (Fig. 3, adipogenic differentiation), and into chondrocytes by Alcian blue staining (Fig. 3, chondrogenic differentiation).
Discussion
The applications of PG have spread into many fields of clinical medicine, especially in sports medicine and in orthopedic surgery (2,19). PG has been considered a promising tool to treat cartilage or bone injuries when pharmacological treatments are helpless. The mechanism of “platelet therapy” is attributed to various growth factors released by platelets that can stimulate cell growth, migration, mobilization, and differentiation (9). Through these biofactors, PG can exert its ability to promote tissue regeneration.
Traditionally, PG is obtained from autologous peripheral blood. In Platelets 2010 (37), some of us described the technical procedure to obtain PG from cord blood, and currently CBPG can be processed, cryopreserved, and stored for any applications without even drawing the patient's blood. This “in advance” storage permits to have a safe, virus-free, controlled, and standardized hemocomponent ready to use.
The initial goal of this study was to better exploit the key biofactors present in CB-PR versus PB-PR to understand if there were different peculiarities that could distinguish these two gels in order to successively identify which could be the most appropriate therapeutic application.
For this purpose, we first had to be sure to rule out any outside influence that could wrongly affect the content of factors in PG. Thus, blood donors were selected with a longstanding history of blood donation, and they did not report any particular disease or infection during their anamnesis. The same was done for the CB donors; they were all full-term infants with an Apgar higher than 9, with no complication during childbirth, and with parents free from any disease or viral/bacterial infection. It remained only to determine whether a possible stress due to cesarean section could be triggering a release of inflammatory factors, and then using an ELISA assay for the most common inflammatory factors, we have ruled out this possibility. Therefore, we successively moved to investigate with the widest possible array which factors were present in larger amounts in CB-PR to the PB-PR. Since the PR is constituted by two components, the platelet poor plasma and the platelet lysate, we wondered which factors were more present in one of them. By developing an experimental strategy that excludes contamination of one another, we have been able for the first time to assign which component contained such factors.
Even if this analysis was principally explorative and performed on a minimal number of biological samples, due to the Luminex Technology that is well known to give reliable quantifications of analytes (52), we obtained very informative data. Thus surprisingly, but perhaps we should have expected it, we found that several hormones strongly supporting fetal tissue formation were present only in CB-PR components (Table 2). Indeed, many of these factors increase during pregnancy such as prolactin (35), progesterone (11), and α-fetoprotein (43). In particular, the latter is the principal plasma protein produced by the yolk sac and liver during fetal life, and it is thought to be the fetal counterpart of albumin. In the literature, some authors demonstrated the presence of albumin in the PB platelet content hypothesizing that megakaryocytes incorporate plasma proteins during developing α-granules by pinocytosis (16). Similarly, the same mechanism could be transferred to the fetal platelet compartment since we found that cord blood platelets are rich in α-fetoprotein. Some of the other factors such as growth hormone could play a role in supporting MSC growth (23), but certainly it could be interesting to investigate which pathways could be stimulated within the stem cell compartment by these factors.
When we look at the major factors expressed in platelet lysate and plasma of the peripheral blood, we discovered a completely different milieu. Interestingly, we found high levels of epidermal growth factor (EGF), which recently has been demonstrated to augment MSC proliferation and also to enhance paracrine secretion (46).
To highlight the most expressed factors divided into large groups, we clustered the proteomic results. In CB we identified higher concentrations of factors known to promote angiogenesis such as VEGF (17), in agreement with the result obtained by Murphy and colleagues (34), or to be involved in a wide variety of pathways including angiogenesis such as resistin (33), prolactin, growth hormone (8), and trefoil factor-3 (39).
To exclude that the enrichment of angiogenic factors in cord blood was driven by fetal hypoxia, we checked the level of erythropoietin as a sensitive marker. Thus, the erythropoietin is known to have an important role in regulating and promoting angiogenesis (20), and its level increases up to 100- to 1,000-fold in severe hypoxia (45). In this regard, we found that erythropoietin was mildly higher (threefold) in both plasma and platelets of CB than in the PB counterparts. The reduced increase in erythropoietin and the high Apgar scores led us to suppose that the enrichment of angiogenic factors in cord blood is a peculiar CBPG property not influenced by a possible fetal hypoxia.
On the contrary, the proteomic analysis reported that PB-PR was richer in inflammatory factors than CB. Chemokine CC4 is a chemokine that stimulates the adhesion of monocytes to endothelial cells (49); CD5 antigenlike is a factor associated to inflammatory and apoptosis processes (44); MMP-3 exerts several effects regulating platelet functions such as platelet adhesion and platelet–leukocyte aggregation (42); RANTES, aka CCL5, is present in platelet α-granules, and it is a potent chemo-attractant for T cells, monocytes, natural killer cells, basophils, and eosinophils (15).
In addition, when we looked at the platelet counterpart, unexpectedly we observed that PB platelets contain much higher TPO levels in comparison with CB platelets (220-fold). Apart from the well-known role of platelets in TPO uptake and degradation, platelets from peripheral blood have been demonstrated to be a carrier of TPO that they release after stimulation (13). This result leads us to suppose that CB platelets have a minor function as a storage pool of TPO. In conclusion of this first part of our work, we can summarize that CBPG contains higher levels of angiogenic factors if compared to the peripheral counterpart. Indeed, we know that pregnancy requires vasculogenesis and angiogenesis in the fetal compartment and angiogenesis in the maternal one (24), and therefore this could influence the quantity of angiogenic factors present in CB.
The second aim of our work was to investigate the impact of this innovative CBPG as a substitute of FBS on the MSC growth and function.
ADMSCs were used as representative MSCs to test the effects of CB-PR versus FBS and PB-PR. MSC cultured with CB-PR, as well as in the presence of PB-PR, grew faster and gave rise to greater numbers of CFU-F with bigger colonies than ADMSCs in FBS. When we looked at the morphology, ADMSCs with CB-PR were the slenderest, which is the reason why these observations are difficult at present to understand, but it is likely that factors present in CB can modulate the MSC cytoskeleton (21,51).
By flow cytometry, ADMSCs did not show any difference in all culture conditions, and they expressed the classical MSC markers. The only one whose expression changed on ADMSCs in A and C conditions was PDGFR-β, recently known as perivascular and stemness marker (10). This change in the mean fluorescence intensity could suggest an increased stemness of ADMSCs cultured in these conditions. Nevertheless, to exclude any possible negative correlation between faster growth and tumorigenic transformation, telomerase activity was evaluated, and it confirmed the safety of ADMSCs cultured under PG.
Based on the previous findings of this work where we demonstrated that CBPG contains more angiogenic factors than its peripheral counterpart, we tried to move this observation on a more functional evaluation using the classical angiogenic assay based on the capillary-like formation. In this context, we demonstrated that CB-PR produced an increased number of tubule structures than PB-PR. Therefore, we have to underline once again the strong angiogenic influence of CBPG not only confirmed by the angiogenic factors present in CB-PR but also by its ability to support angiogenesis structures.
Regarding the differentiative potential possibly promoted by FBS versus platelet derivates, an interesting initial commitment toward osteogenic lineage was observed in ADMSC cultures in the presence of PB-PR by molecular analysis where we found a higher expression of MSX2 and RUNX2 known as osteogenic genes (7,14). But when we moved to use the classical differentiative culture systems, unfortunately this commitment was flatted, maybe due to the use of strongly osteogenic commercial media. Therefore, in the differentiation assay, no relevant differences were observed.
In conclusion, first we have extensively expanded the knowledge on the content of biofactors present in the plasma and in the platelet compartment of two different platelet gels. These findings could support the regenerative medicine field to apply them for more tailored therapeutic applications. In particular, from this study, it comes out that for osteogenic applications PBPG could give a better performance, in agreement with previous data (37) where we observed higher levels of transforming growth factor-β, known as osteogenic factor, in PB-PR than CB-PR, while for applications of angiogenic and tissue repair CBPG could be envisioned.
Second, we demonstrated that PG can represent a valid alternative to animal serum for MSC culture without changing the stability and the phenotype of MSCs. Since it is becoming more and more clear that soluble factors present in the culture media can modulate the stem cell fate and commitment (12,36), using more prone angiogenic supplements, such as the CB-PR, may result in a greater angiogenic ability of MSCs.
As a whole, this study opens the door to this innovative CBPG as FBS alternative for culturing MSCs for cell therapy and regenerative medicine.
Footnotes
Acknowledgments
The authors would like to thank Paolo Rebulla for his scientific support in developing the Cord Blood Platelet Gel project. We are also grateful to the Milano Cord Blood group for their help in providing cord blood units. This work was partially supported by funds from Regione Lombardia (PB 0098), from Ministero della Salute Italiano (“Young Researchers” grants: R.F.G.R. 2010-2318448, R.F.G.R. 2010-2312573), and from European Union's Seventh Programme (Grant Agreement No. 241879). All these funds cooperated to support this study mainly covering the salaries of the authors involved in this research. Valentina Parazzi and Lorenza Lazzari declare their role as inventors in patent No. PCT WO/2010/007502 “Platelet fraction deriving from placental blood.” The other authors declare no conflicts of interest.