
Abstract
Patients with severe hypophosphatasia (HPP) develop osteogenic impairment with extremely low alkaline phosphatase (ALP) activity, resulting in a fatal course during infancy. Mesenchymal stem cells (MSCs) differentiate into various mesenchymal lineages, including bone and cartilage. The efficacy of allogeneic hematopoietic stem cell transplantation for congenital skeletal and storage disorders is limited, and therefore we focused on MSCs for the treatment of HPP. To determine the effect of MSCs on osteogenesis, we performed multiple infusions of ex vivo expanded allogeneic MSCs for two patients with severe HPP who had undergone bone marrow transplantation (BMT) from asymptomatic relatives harboring the heterozygous mutation. There were improvements in not only bone mineralization but also muscle mass, respiratory function, and mental development, resulting in the patients being alive at the age of 3. After the infusion of MSCs, chimerism analysis of the mesenchymal cell fraction isolated from bone marrow in the patients demonstrated that donor-derived DNA sequences existed. Adverse events of BMT were tolerated, whereas those of MSC infusion did not occur. However, restoration of ALP activity was limited, and normal bony architecture could not be achieved. Our data suggest that multiple MSC infusions, following BMT, were effective and brought about clinical benefits for patients with lethal HPP. Allogeneic MSC-based therapy would be useful for patients with other congenital bone diseases and tissue disorders if the curative strategy to restore clinically normal features, including bony architecture, can be established.
Keywords
Introduction
Hypophosphatasia (HPP) is a bone metabolic disorder caused by mutations in the liver/bone/kidney alkaline phosphatase (ALPL) gene, which encodes tissue-nonspecific alkaline phosphatase (ALP) (24,38). The disease is characterized by the disturbance of bone and tooth mineralization and reduced serum ALP activity (24,38). Many patients with HPP show autosomal dominant inheritance, while others show autosomal recessive inheritance (24,38). Clinically, the former has a mild phenotype, whereas the latter has a severe one. The clinical severity of HPP often depends on the age of onset. In particular, patients with HPP during the perinatal and infantile periods have a poor prognosis because they usually die from respiratory failure caused by a profound reduction in the osteogenesis of the thorax(24,38). The phenotype of patients with HPP is also closely related to the residual enzyme activity affected by ALPL mutations (24,38). Bone-targeting enzyme replacement therapy, cell transplantation derived from bone and bone marrow, and gene therapy are under development for the treatment of HPP(5,39,40). However, there is currently no well-established therapy for HPP.
Mesenchymal stem cells (MSCs) reside in bone marrow (BM) and other tissues such as fat, cartilage, synovium, tonsil, dental pulp, placenta, and umbilical cord. MSCs possess self-renewal capacity and can differentiate into various mesenchymal lineages and several mesoderm lineages, including the osteogenic, chondrogenic, and adipogenic lineages (1). MSCs function as a multipotent modality in immune regulation as well as the repair and regeneration of tissues and organs (1,36). Their regenerative ability makes MSCs an ideal source for transplantation in patients with osteogenesis imperfecta, inborn errors of metabolism, and ischemic heart diseases (1,10,11,17,36). Furthermore, MSCs support the maintenance of hematopoietic stem cells, facilitate hematopoietic recovery, and reduce graft-versus-host disease (GVHD) by modulating the immune functions of T cells, B cells, natural killer cells, monocytes, and dendritic cells (1,32,36).
Some studies have reported the use of bone marrow transplantation (BMT), BM stromal cells, bone fragment, and cultured osteoblasts in the treatment of HPP (5,40). However, the clinical efficacy of these procedures is limited (5,40). We previously performed allogeneic BMT, MSC transplantation (MSCT), and osteogenic construct implantation for a patient with severe HPP. Symptoms of the patient improved to some extent, and new bone formation derived from cells of both the donor and the patient was detected (34). Nevertheless, the procedure was very complicated, and clinical features such as mineralization were not sufficient compared with healthy children, while the titer of serum ALP remained very low (34). To focus on the osteogenic effects of the MSCs, we performed transplantation of ex vivo expanded MSCs for patients with severe HPP who had previously undergone BMT.
Materials and Methods
The Purpose
This clinical trial (UMIN ID: 000003828) was approved by the ethical committees of Shimane University Hospital and the National Institute of Advanced Industrial Science and Technology. This trial was also approved by the Ministry of Health, Labour, and Welfare under the guidelines for clinical trials using human stem cells. The primary endpoint of this study was to assess the 3-year survival rate, as most patients with severe HPP died before the age of 1 (35,38). The secondary endpoints were to assess the following: (I) clinical symptoms, including respiratory condition, height, weight, and infant development assessed by the Enjoji scale; (II) osteogenic parameters such as X-ray/computed tomography (CT), biochemical markers, and bone density measured by dual-energy X-ray absorptiometry (DXA); and (III) adverse effects of the treatments. The biochemical markers evaluated were ALP; urine phosphoethanolamine (PEA; a substrate of ALP); bone formation markers [bone-type ALP (BAP), osteocalcin (OC), undercarboxylated osteocalcin (ucOC), and type I procollagen N-terminal propeptide (intact PINP)]; and bone resorption markers [urine deoxypyridinoline (DPD), urine cross-linked N-telopeptide of type I collagen (NTx), pyridinoline cross-linked carboxyterminal telopeptide of type I collagen (ICTP), and type 5b tartrate-resistant acid phosphatase (TRACP-5b)].
Patients and Donors
The patients fulfilled the following conditions: (I) disease onset before 6 months postbirth; (II) respiratory disturbance; (III) ALPL mutations with low serum ALP activity; (IV) impaired osteogenic differentiation capability of patient's MSCs; and (V) normal cardiac, liver, and renal functions, which predict the safety of BMT. The criteria of the donors were as follows: (I) first- or second-degree relative; (II) normal bone mineralization evaluated by clinical features and radiological imaging tests and bone density measured by DXA; (III) normal range of serum ALP; (IV) no mutations or heterogeneous mutations of ALPL; (V) negative results for blood-borne viruses, including human immunodeficiency virus, hepatitis B virus, hepatitis C virus, human T-lymphotropic virus, and human parvovirus B19; and (VI) healthy condition suitable for marrow donation. Two male patients were recruited in this study. Each donor of the two patients was one of the patient's parents.
BMT Procedure
After obtaining consent from the patients’ parents, we determined the timing of the transplantation procedure. First, we performed single allogeneic BMT, and subsequently multiple allogeneic MSCT from the same BM donor at Shimane University Hospital. BM was obtained from iliac bone of each donor under general anesthesia. The conditioning regimen of BMT was a myeloablative protocol. Intravenous dosages of the following drugs were administered: intravenous busulfan (Kyowa Hakko Kirin, Tokyo, Japan) at 0.9–1 mg/kg per dose every 6 h (days -10, –9, –8, and –7), cyclophosphamide (Baxter, Weiterstadt, Germany) at 60 mg/kg per dose (days –6, –5), and rabbit-derived anti-thymocyte globulin (BMT Genzyme Japan, Tokyo, Japan) at 1.25 mg/kg per dose (days –4, –3, –2, –1). Short-term methotrexate (Pfizer, Tokyo, Japan) or tacrolimus (FK506; Astellas Pharma, Northbrook, IL, USA) was administered for the prophylaxis of GVHD. Trough titer concentrations of FK506 ranged from 5 to 10 ng/ml.
Ex Vivo Expansion of MSCs and the Procedure of MSCT
The first MSCT was performed 2 weeks after BMT. Under good manufacturing practices, MSCs were expanded ex vivo in our aseptic cell-processing center. Approximately 20–40 ml of the donor-derived BM was used for culture expansion of MSCs in a flask (Corning, New York, NY, USA) containing basal medium [a-minimum essential medium (Gibco, Grand Island, NY, USA) with 15% fetal bovine serum (FBS; SAFC Biosciences, Inc., Lenexa, KS, USA) and 20 μg/ml gentamicin (Merck & Co., Inc., Whitehouse Station, NJ, USA)]. The FBS was certified as endotoxin free, sterilized by γ rays, and produced in countries (Australia or New Zealand) where occurrences of bovine spongiform encephalopathy have not been reported. The adherent cells became nearly confluent after 10 to 12 days and were passaged using a trypsin-like enzyme solution (TrypLE Select; Invitrogen Corp., Carlsbad, CA, USA) into another flask. After several days, the first passaged cells were collected using the TrypLE Select and used for transplantation. In some cases, to acquire enough cell numbers, the first passaged cells were further passaged once, and the second passaged cells were used for the transplantation. The mean population doubling level (cumulative population doublings) of these passaged cells for the transplantation was 3.48 ± 1.31.
The expression pattern of cell surface antigens was mesenchymal type [cluster of differentiation 34 (CD34) negative, CD45 negative, CD105 positive, and SH3 (CD73) positive] (Immunotech, Marseille, France). All fluorescent antibodies were mouse monoclonal IgG1 (Immunotech) against human cell surface antigen. Final concentrations of all antibodies were described in the manufacturer's instruction. To identify the expression of cell surface antigens, we performed flow cytometric analysis. MSCs were incubated with fluorescein isothiocyanate (FITC)-conjugated CD antibodies (the concentration of each antibody, 2.5 mM) on ice for 30 min. They were then washed and passed through cell strainers [Becton, Dickinson and Company (BD), Franklin Lakes, NJ, USA] to remove any cell clumps. Flow cytometric analysis was performed on a FACSCalibur system (BD). We defined the passage number of MSCs up to two because excessive passages of MSCs can provoke malignant transformation (29). The number of transplanted MSCs ranged from 1.0 to 2.0 × 106 cells per kilogram of body weight. The MSCs, dissolved in 20 ml of phosphate-buffered saline (Gibco), were intravenously administered. MSCT was only repeatedly performed if symptoms did not improve or worsened 2 to 4 months after BMT and the first MSCT.
Measurement of Osteogenic Parameters
Each osteogenic biochemical marker was measured in the following way: ALP in enzyme reaction method using p-nitrophenyl phosphate (pNPP) as substrate; urine PEA in high-performance liquid chromatography (Wako Pure Chemical Industries, Osaka, Japan); BAP in enzyme immunoassay (EIA; Quidel, San Diego, CA, USA); OC in immunoradiometric assay (LSI Medience, Tokyo, Japan); ucOC in electrochemiluminescence immunoassay (EIDIA, Tokyo, Japan); intact PINP in double-antibody radioimmu-noassay (RIA2 antibody assay; Orion Diagnostica, Espoo, Finland); urine DPD in EIA (Quidel); urine NTx in EIA; ICTP in RIA2 antibody assay (Orion Diagnostica); TRACP-5b in EIA (Quidel). Each image analysis was performed by the following instrument: X-ray by RADspeed Pro (Shimzu, Kyoto, Japan); CT by Brilliance CT 64 (Philips, Amsterdam, the Netherlands); DEA by QDR Discovery (Hologic, Bedford, MA, USA).
ALPL Gene Analysis
Informed consent was obtained from the families of patients, and DNA was extracted from peripheral blood samples. Mutations were analyzed by PCR throughout the ALPL coding region (Ensembl/Havana merged gene: ENSG00000162551). PCR and sequencing procedures were performed as previously described (35).
Matrix Mineralization Assay
Matrix mineralization of osteoblasts differentiated from MSCs was detected by the intensity of the fluorescence of calcein, a fluorescent calcium-binding chemical. MSCs from donors at passage one were seeded at a density of 2 × 104 cells/well in a 12-well plate in the presence of 10 mM β-glycerophosphate (β-GP; Merck KGaA, Darmstadt, Germany) with or without 0.07 mM ascorbic acid 2-phosphate (Sigma-Aldrich Corp., St. Louis, MO, USA) and 100 nM dexamethasone (Dex) (Nacalai Tesque, Kyoto, Japan) in basal medium for 2 weeks. Calcein (Dojindo Laboratories, Kumamoto, Japan) was added to the medium at a concentration of 1 μg/ml for 14 days in culture. The fluorescence of the calcein incorporated into the matrix minerals was visualized using an image analyzer (Typhoon 8600, 526 nm short-pass filter; GE Healthcare Life Sciences, Pittsburgh, PA, USA) by placing the culture plate directly in the analyzer. The scanned fluorescence images of each well in the culture plate were quantified by ImageQuant software (Molecular Dynamics World Headquarters, Sunnyvale, CA, USA) and represented as pixel intensity per area.
In Vitro Assay of ALP Activity
MSCs from donors at passage one were seeded at a density of 2 × 104 cells/well in a 12-well plate (Corning) in the presence of 10 mM β-GP with or without 0.07 mM ascorbic acid 2-phosphate and 100 nM Dex in basal medium for 2 weeks. MSCs were harvested with 0.5 ml of buffer containing 10 mM Tris-HCl (Nacalai Tesque), 1 mM EDTA (Nacalai Tesque), and 100 mM NaCl (pH 7.4) (Nacalai Tesque). The cell suspension was sonicated and centrifuged at 14,000 × g for 3 min at 4°C. The reaction mixture, which was incubated at 37°C for 30 min, consisted of both an aliquot (20 μl) of the supernatant and 100 μl of pNPP solution (Zymed Laboratories Inc., South San Francisco, CA, USA). After termination of the enzymatic reaction with 100 μl of 1 M NaOH (Nacalai Tesque) solution, the absorbance of the p-nitrophenol (pNP) product formed was measured at 405 nm on a microplate reader (Wallac 1420 ARVOsx; PerkinElmer Life & Analytical Sciences, Shelton, CT, USA). The DNA contents of the cells were measured using an aliquot (20 μl) of the sonicated sample with 200 μl of 1.25 μg/ml Hoechst 33258 (Life Technologies, Osaka, Japan). A standard curve was set up using salmon sperm DNA (Invitrogen Corp.). ALP activity was expressed as μmol of pNP released per 30 min per unit of DNA content.
Chimerism Analysis of BM and Isolated MSCs From BM
DNA was extracted from BM and MSCs of patients. Short tandem repeat analysis was performed using AmpFlSTR® SGM Plus (PE Biosystems, Foster City, CA, USA) and ABI PRISM® 310 Genetic Analyzer (PE Biosystems). The method of MSC isolation from BM was as follows. BM cells (10 ml) were centrifuged at 400 × g for 5 min at 4°C. The supernatant was discarded by pipetting. Then, 5 ml of 1× PBS was added to the tube and pipetted gently. Next, 10 ml of the cell solution was added to 3 ml of lymphocyte separation solution (Nacalai Tesque) without mixing. The tube was centrifuged at 400 × g for 25 min at 4°C. Lymphocytes were transferred into a 14-ml tube (BD), and 10 ml of 1× PBS was added to it. The tube was then centrifuged at 200 × g for 5 min at 4°C. It was washed twice by 10 ml of 1× PBS containing 0.5% bovine serum albumin (BSA; Sigma-Aldrich) and centrifuged at 200 × g for 5 min at 4°C. Then, 2 ml of 1× PBS containing 0.5% BSA was added and mixed by pipetting. Cells (300 μl) in PBS were stained for CD45 (FITC), CD235a (FITC), CD105 (PE), and CD90 [PE-cyanine 5 (PC5); Beckman Coulter, Marseille, France] for 30 min on ice in the dark. All antibodies were mouse monoclonal antibodies against human cell surface antigens. Final concentrations of all antibodies were described in the manufacturer's instructions. Each isotype (mouse monoclonal IgG1) was used as a negative control. Cells were washed with 1 ml of 1× PBS containing 0.5% BSA and centrifuged at 200 × g for 5 min. Then, 250 μl of 1× PBS containing 0.5% BSA was added and mixed by pipetting. Cells were filtered with preseparation filters (Miltenyi Biotec, Bergisch Gladbach, Germany). MSCs were harvested and sorted (BD FACS Aria II; BD Immunocytometry Systems, San Jose, CA, USA) into a 15-ml tube containing 10 ml of 1× PBS containing 0.5% BSA.
Results
Clinical Course
Patient 1
The patient was observed to have shortening and deformity in the extremities during the fetal period. The male infant was delivered vaginally at the gestational age of 40 weeks and 1 day. Tachypnea, low titers of ALP (7 IU/L), and high titers of urine PEA (5727.4 nmol/mg Cr) were seen at birth. The radiograph findings revealed hypomineralization, flared metaphyses, and a narrow thorax, all of which suggested perinatal lethal HPP. The patient's respiratory disturbance gradually deteriorated, and he was artificially ventilated 3 months after birth. ALPL mutation analysis showed the homozygous mutation of c.1559delT, and bone mineralization assay of his BM-derived MSCs revealed a very low osteogenic capacity of the MSCs.
With the parents’ consent, the male patient, at the age of 14 months, underwent allogeneic BMT (HLA 2 locus mismatch) from his father (30 years old), whose clinical bone structure, serum ALP titer, and in vitro MSC mineralization of BM were normal. Sixteen days after BMT, we intravenously performed the first MSCT for the patient. BM was engrafted 17 days after BMT, and FK506 administration was stopped 2 months after BMT. The second MSCT was performed at the age of 17 months because severe cyanotic attacks repeatedly occurred owing to tracheobronchomalacia, a lethal complication of HPP, and hypoxic brain damage, including visual disability, developed at the age of 16 months. After the second MSCT, tracheobronchomalacia disappeared, and the patient's respiration improved even without artificial respiration during the daytime. The third (at 27 months old) and fourth (at 32 months old) MSCTs were performed because of low titers of ALP and prolonged hypomineralization. At the age of 3 years, the patient could sit on a chair and walk with a walker. His height, weight, and length of the extremities gradually improved (Fig. 1A1, B1). The psychomotor scores evaluated by the Enjoji scale increased, although this score temporarily decreased due to hypoxic brain damage (Fig. 2A1). The number of MSCTs performed was four (from 15 to 32 months old), and the average MSC number per transplantation was 1.4 × 106 cells/kg.

Physical growth of height, weight, and length of extremities. (A1 and B1) Patient 1; (A2 and B2) patient 2; M, month. (A) Bold and dashed lines indicate height and weight, respectively; (B) bold and dashed lines indicate length of upper and lower extremity, respectively. Arrowhead and arrows indicate BMT and MSCT, respectively.
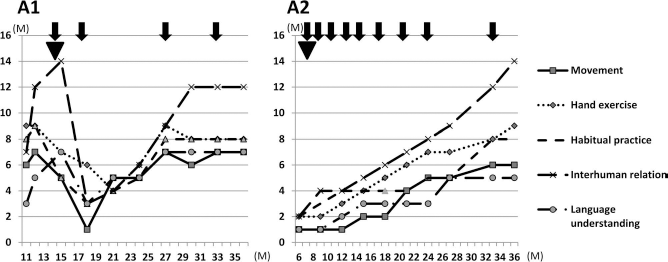
Development assessment by the Enjoji scale. (A1) Patient 1; (A2) patient 2; M, month. The Enjoji score is an assessment of infant analytical development. Vertical axis indicates the age that is equivalent to development; horizontal axis shows the chronological age. Arrowhead and arrows indicate BMT and MSCT, respectively.
Radiography demonstrated that cupping of the linea epiphysialis at the age of 12 months, which was present before transplantation, disappeared, and that mineralization in the area improved. Mineralization and the length of long bones also gradually recovered (Fig. 3A1–F1). Interestingly, both bone density and muscle mass increased, as shown by DXA measurement (Fig. 4A1). Bone fragility, however, persisted. Subsequently, bone deformities became progressively worse. Biochemical analysis showed that low titers of ALP, BAP, and OC continued, although intact PINP and ucOC increased (Fig. 5A1–C1). Bone resorption markers such as DPD, NTx, ICTP, and TRACP-5b remained unchanged (Fig. 5D1, E1).

Longitudinal course of image findings. (A1–F1) Patient 1; (A1, C1, and E1) 12 months old; (B1, D1, and F1) 36 months old; (A2–F2) patient 2; (A2, C2, and E2) 6 months old; (B2, D2, and F2) 24 months old; (A–D) X-ray; (E and F) computed tomography.

Chronological observation of bone density and muscle volume. (A1) Patient 1; (A2) patient 2; M, month; bold and dashed lines indicate bone density and muscle volume, respectively. Both bone density and muscle volume were evaluated by dual-energy X-ray absorptiometry measurements. Arrowhead and arrows indicate BMT and MSCT, respectively.
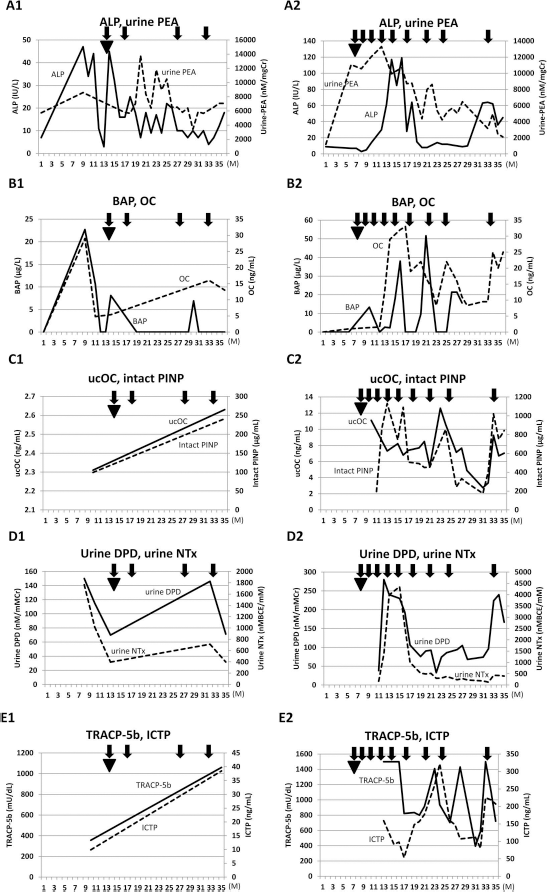
Sequential change of biochemical markers. (A1-E1) Patient 1; (A2-E2) patient 2; M, month; ALP, alkaline phosphatase; PEA, urine phosphoethanolamine; BAP, bone-type ALP; OC, osteocalcin; ucOC, undercarboxylated osteocalcin; intact PINP, type I procollagen N-terminal propeptide; DPD, urine deoxypyridinoline; NTx, urine cross-linked N-telopeptide of type I collagen; TRACP-5b, type 5b tartrate-resistant acid phosphatase; ICTP, pyridinoline cross-linked carboxyterminal telopeptide of type I collagen. (A) Bold and dashed lines indicate ALP and urine PEA, respectively; (B) bold and dashed lines indicate BAP and OC, respectively; (C) bold and dashed lines indicate ucOC and intact PINP, respectively; (D) bold and dashed lines indicate urine DPD and urine NTx, respectively; (E) bold and dashed lines indicate TRACP-5b and ICTP, respectively. Each biochemical marker was measured in the following way: ALP in enzyme reaction method using pNPP as substrate; urine PEA in high-performance liquid chromatography; BAP in EIA; OC in immunoradiometric assay; ucOC in EIDIA; intact PINP in RIA2 antibody assay; urine DPD in EIA; urine NTx in EIA; ICTP in RIA2 antibody assay; TRACP5b in EIA. Arrowhead and arrows indicate BMT and MSCT, respectively.
The side effects of BMT were acute skin GVHD (grade 1) and drug-induced liver dysfunction. Hypothyroidism developed 2 months after BMT, and the patient's thyroid function recovered by thyroid hormone treatment. There were no adverse effects of MSCT.
Patient 2
During the patient's fetal phase, hydramnion was present, and bone abnormality was detected. The male infant was born transvaginally at the gestational age of 41 weeks and 2 days. Respiratory impairment became worse soon after birth; therefore, mechanical ventilation was performed. Low titers of serum ALP (9 IU/L), hypomineralization, fluttering in the epiphyseal regions, and narrow thorax revealed by X-ray indicated that the patient had developed perinatal lethal HPP. Convulsions developed 5 days after birth, which ceased with the administration of pyridoxine (Torii Pharmaceutical Co., Ltd., Tokyo, Japan). Tracheobronchomalacia frequently appeared from 6 months after birth. Similar to patient 1, the patient harbored a homozygous mutation in c.1559delT of ALPL; moreover, bone mineralization assay of his BM-derived MSCs showed very low osteogenesis.
Allogeneic BMT from the patient's mother (27 years old, HLA 1 locus mismatch) was performed at the age of 7 months with the parents’ consent. The patient's mother had clinically normal bone structure, serum ALP titer, and in vitro mineralization. BM was engrafted 19 days after BMT, and MSCs were first transplanted 17 days after BMT. Severe acute gut GVHD (grade 4) developed and did not improve with the administration of several immunosuppressive drugs, including cyclosporin A (Novartis Pharma, Tokyo, Japan), FK506, steroids, and infliximab (Mitsubishi Tanabe Pharma, Osaka, Japan). Interestingly, 1 week after the second MSCT, which took place 51 days after BMT, intractable bloody diarrhea dramatically improved. Chronic liver GVHD, which occurred 3 months after BMT, was cured with the third MSCT and treatment with FK506. As a result, we administered FK506 until the patient was 24 months old. However, respiratory disturbance and hypomineralization did not ameliorate. Therefore, we performed three additional MSCTs (fourth to sixth) until the patient was 17 months old. At the age of 18 months, his respiratory condition became stable, and tracheobronchomalacia disappeared. Two additional MSCTs (seventh and eighth, at 21 and 24 months old, respectively) were performed because chronic hypoxemia and bone fragility persisted. When the patient was 29 months old, tracheobronchomalacia relapsed because severe pneumonia occurred. Two months after the ninth MSCT at the age of 33 months, the issue of tracheobronchomalacia was resolved. At the age of 3 years, the patient could sit on a chair, and his respiratory condition stabilized, although he breathed with the help of a ventilator. His height, weight, and length of extremities gradually increased (Fig. 1A2, B2). However, the psychomotor scores evaluated by the Enjoji scale were lower than those of healthy children (Fig. 2A2). The number of MSCTs performed was nine (from 7 to 33 months old), and the average MSC number per transplantation was 1.8 × 106 cells/kg.
Hypomineralization of both the long bone and the flat bone improved. In particular, mineralized areas of the cranial bone, which were lost before treatment, recovered dramatically. The length of the long bones also recovered gradually (Fig. 3A2–F2). Similar to patient 1, both bone density and muscle mass, measured by DXA, increased (Fig. 4A2). The titer of ALP started to increase from 11 months old, but decreased from 20 months old. The ALP titer increased again at 30 months old, and urine PEA gradually decreased (Fig. 5A2). Intriguingly, markers of bone formation such as BAP, OC, ucOC, and intact PINP changed along with ALP (Fig. 5B2, C2). NTx decreased, but levels of other bone resorption markers did not vary erratically (Fig. 5D2, E2).
For the treatment of BMT side effects and acute severe gut GVHD and chronic liver GVHD, combination treatment with MSCs and immunosuppressant agents was administered. Hypothyroidism developed 18 months after BMT. However, thyroid function recovered with thyroid hormone treatment. Moreover, complex partial epilepsy, of which the seizure type was apnea attack, occurred 16 months after BMT, and this attack ceased with car-bamazepine. There were no adverse effects of MSCT.
Chimerism Analysis
To confirm whether the transplanted BM and MSCs were engrafted, we performed chimerism analysis. In terms of BM chimerism, patient 1 achieved complete donor type 30 days after BMT, but the proportion of donor cells declined to 10%. On the other hand, patient 2 maintained complete donor type until he was 3 years old. The number of MSCs isolated from BM using flow cytometry was very small, so we performed chimerism analysis by short tandem repeat. To confirm whether donor-derived MSCs exist, we carried out ALPL mutational analysis. In both patients, we identified the normal wild-type ALPL gene as well as the mutant one (Fig. 6), suggesting that donor-derived MSCs were engrafted in BM.

Chimerism analysis of MSCs from BM. Representative data of patient 1. MSCs were isolated from BM by flow cytometry. The first fraction was CD90-positive, CD45-negative, and CD235a-negative. The second fraction was CD90-positive and CD105-positive. DNA was extracted from the second fraction, and exon 12 of the ALPL gene was sequenced. The upper sequence (pre-MSCT) shows the data from patient BM before MSCT, and the lower sequence (post-MSCT) shows that after MSCT. The upper and lower data indicate homozygous deletion of c.1559delT and heterozygous deletion of c.1559delT, respectively. In the lower data, the backward base sequence from the enclosed character “T,” c.1559T, cannot be determined because wild type and deletion of c.1559delT overlap.
Osteogenic Capacity of MSCs From Donors
MSCs can show osteogenic differentiation capability, which can be ascertained by culturing the MSCs in medium containing Dex (28). However, due to mutations in the patients’ ALPL gene, the MSCs from the patients scarcely had normal osteogenic differentiation capabilities. Therefore, we transplanted donor MSCs instead of the patient's own MSCs. To examine whether the ex vivo expanded donor MSCs exhibited osteogenic differentiation capability, we measured ALP activity and matrix mineralization by culturing donor MSCs in the presence or absence of Dex. The capacity of the mineralization was measured by examining the uptake of calcein, a fluorescent calcium-binding chemical (37). As seen in Figure 7, the MSCs from two donors showed high ALP activity when cultured in the medium containing Dex. The activity was comparable to normal MSCs from a third party (16). Furthermore, calcein uptake was drastically elevated when cultured with Dex, although the uptake differed substantially between each expanded MSCs from BM. Therefore, the ex vivo expanded donor MSCs possessed osteogenic differentiation capabilities.
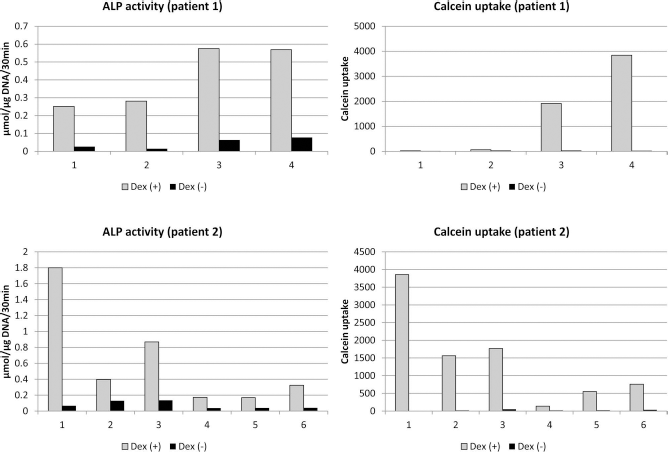
Osteogenic capacity of MSCs from donors. ALP activity was examined by determining the absorbance of p-nitrophenol, which is produced by dephosphorylation of p-nitrophenyl phosphate, a substrate of ALP. Matrix mineralization was detected by the intensity of the fluorescence of calcein. The number of donor bone marrows used for culture expansion of the MSCs was four from patient 1 and six from patient 2. The MSCs were cultured in the presence (Dex+) or absence (DEX–) of dexamethasone.
Discussion
We performed multiple courses of allogeneic, ex vivo expanded MSCTs (four times in patient 1, and nine times in patient 2) following initial BMT for patients with lethal HPP. The reasons why we used a combination of single BMT and multiple MSCTs were as follows: (I) MSCs that reside after allogeneic BMT are derived from patients themselves, not donors (3,8), and thus cellular replacement therapy using only BMT for osteogenesis would be insufficient (12,30); (II) allogeneic MSCs (without BMT) could not be engrafted for a long time (4); (III) in animal studies, allogeneic MSCs survived and induced ossification only with the administration of immunosuppressant agents (7,18,28); (IV) most of the intravenously infused MSCs were trapped in the capillary blood vessels of the lung (41), and thus the number of MSCs homed to bone seemed to be low; (V) in many clinical trials, MSCT was safe, without allergic reaction, lung infarction, or malignant transformation of MSCs (1,10,11,17,36); and (VI) the method of BMT for infancy is established.
Although biochemical markers such as ALP and BAP were not normalized, bone mineralization in the two patients improved to some extent, resulting in both survival with the recovery of respiratory disturbance and the progression of physical and mental development. Interestingly, muscle mass ameliorated. We also confirmed the engraftment of donor-derived MSCs. The natural course of patients with severe HPP, especially those having homozygous deletion of c.1559T in the ALPL gene, is lethal, with the decline and disappearance of bone mineralization (22,35). We are thus encouraged by the long-term survival of these two patients. Moreover, side effects of BMT were tolerated. Severe instances of immunosuppressant-refractory GVHD in patient 2 were cured with MSCT. Adverse events did not occur in spite of multiple infusions of MSCs in both patients. These data suggested that allogeneic MSCT combined with BMT might be one of the safer and more effective remedies for patients with severe HPP, although long-term effectiveness remains unknown and warrants further study.
Nevertheless, bony architecture did not develop as in normal healthy children. In this regard, combining allogeneic MSCT with BMT for patients with osteogenesis imperfecta, metachromatic leukodystrophy, and Hunter syndrome is also considered safe, but offers only limited effectiveness against clinical features (10,11,17). The reasons attributed are as follows: (I) the number of MSCs migrating and engrafting to bone and BM was low (10,11,15,17,23,41), (II) the engrafted MSCs had a low capacity for self-renewal and differentiation into osteoblasts (21,23), (III) some MSCs were rejected by the alloimmune response (2), and (IV) the timing of MSCT was too late to achieve normal bony structure because bone formation began in the fetal phase.
The mechanism of MSCT for its therapeutic efficacy is generally cell replacement and trophic action. The former occurs through transplanted MSCs, which were homed and engrafted to target host tissues and organs, resulting in functional restoration via the replacement of dysfunctional cells (1,36). The latter involves nutritional factors, cytokines, extracellular matrices, and endocytic microvesicles produced by the transplanted MSCs, providing a protective effect and tissue-repair ability for host cells and resulting in the restoration of functions (1,36). The effect of GVHD corresponded to the latter mechanism because anti-inflammatory and immunosuppressant cytokines released by MSCs regulated immune cells, including T cells (1,32,36). The drastic efficacy of severe gut GVHDs in patient 2 was thought to be due to cytokine suppression and tissue repair by the transplanted MSCs, although we could not examine the cytokine levels and the histology of the gut tissues. On the other hand, improvements in bone mineralization for both patients fit the former mechanism. Recently, fresh platelet-derived growth factor receptor α-positive stem cell antigen-positive CD45-negative TER119 antibody-negative (PDGFRa+Sca-1+CD45–TER119–) MSCs, isolated by flow cytometry from adult mouse BM, were found to generate colonies at a high frequency and could migrate to BM and differentiate into hematopoietic niche cells, osteoblasts, and adipocytes after in vivo transplantation (23). However, it was reported that ex vivo MSCs cultured using a common practice like our culture method could hardly migrate into BM, and most of the MSCs were trapped inside the pulmonary capillary vessels (22). The trapping of MSCs in the lung could be reduced with intravenous sodium nitroprusside, one of the vasodilator drugs (33). In the osteogenesis imperfecta murine model, intramedullary MSCs implanted in femurs were engrafted, differentiated into osteoblasts and osteocytes, and maintained their progenitor potential in vivo (20). Mabuchi et al. reported that rapidly expanded clones in human low-affinity nerve growth factor receptor-positive thymocyte antigen 1-positive (LNGFR+THY-1+) MSCs from BM, peripheral blood, and dental pulp exhibited robust multilineage differentiation and self-renewal potency (21). Moreover, we used MSCs with heterozygous mutations of the ALPL gene, although in vitro ALP activity and matrix mineralization in donor-derived MSCs were detected. However, our donors were adults. The self-renewal capacity and proliferation of MSCs derived from the umbilical cord and BM from young children were higher than those of BM-derived MSCs from adults (9,31). Therefore, to consolidate curative treatments with MSCT for patients with congenital skeletal and soft tissue diseases, including HPP, we need to design an isolated MSC culture system with excellent cellular characteristics including migration, self-renewal, and differentiation in order to target cells and to establish a suitable MSC transplant procedure, such as direct implantation into BM (20). Allogeneic umbilical cord-derived MSCT with cord blood stem cell transplantation from the same donors having normal alleles of the ALPL gene may be considered.
In both of our patients, not only bone but also muscle function, respiratory function, and mental development have improved. Recently, many reports have demonstrated that muscle mass was positively related to bone mass by mechanical stress, endocrine factors, and cytokines (14). Muscle volume improved in proportion to bone density in our patients. For lung diseases, MSCs exhibited trophic effects that regulate endothelial and epithelial permeability, reduce inflammation, inhibit apoptosis, and promote tissue repair (13,19). Temporal improvement of respiratory disturbance in our patients might be due to these trophic effects, although beneficial changes in the respiratory muscles and costal bone contributed to clinical pulmonary improvement. Moreover, MSCs can induce a neuroprotective microenvironment by antiapototic and anti-inflammatory effects and differentiate into mature neurons by proliferation and maturation of local neural precursor cells (6,36). Hypoxic brain damage in our patients may have been improved by the bystander effects of MSCs on neural cells. In addition, in vitro studies clarified the differentiation ability of MSCs into muscle cells and lung cells (of endoderm origin) as well as neural cells (of ectoderm origin) (36). Some in vivo studies demonstrated that MSCs differentiate into endothelial cells and support neovascularization (25,26), suggesting that new blood vessels were formed in the target tissues after MSC infusion. Further studies are required to clarify the mechanisms underlying the improvement of respiratory functions and mental development in our patients.
Regarding serum ALP, the titer of ALP increased after MSCT in patient 2 but remained low in patient 1. The ratios of donor-derived BM in patients 1 and 2 were 10% and 100%, respectively, suggesting that the difference in the engraftment of donor-derived BM may influence the engraftment of donor-derived MSCs. Interestingly, after a decrease, the serum ALP value in patient 2 rose again from the age of 20 months. We previously reported that ALP activity rose with 1-month administration of FK506 in rat studies (18). By contrast, Nassar et al. reported that at 60, 180, and 240 days of treatment with FK506 in rats, ALP levels significantly decreased (27). Patient 2 was treated with FK506, and the ALP value increased again 12 months after cessation of FK506. These results suggested that prolonged administration of FK506 might affect bone turnover, which reflects ALP activity, although many factors contribute to the pathogenesis of bone metabolism after MSC transplantation.
In conclusion, multiple transplantations of allogeneic ex vivo expanded MSCs following initial BMT were performed and resulted in survival and certain clinical benefits for patients diagnosed with lethal HPP. However, we need to establish curative MSC-based treatment strategies that can maintain the long-term survival and differentiation capabilities of transplanted allo-MSCs. The strategies can achieve clinically normal features, including bony architecture, and may be available for patients with other congenital bone and tissue disorders.
Footnotes
Acknowledgments
We thank Ms. Midori Furui, Mayumi Nagase, Mayumi Naito, and Rie Eda for support during the molecular analysis and flow cytometry analysis. This study was supported by the Project for Realization of Regenerative Medicine, Ministry of Education, Culture, Sports, Science and Technology, and Research on Regenerative Medicine for Clinical Application, Ministry of Health, Labour and Welfare. The authors have no financial relationships relevant to this article to disclose. The authors declare no conflicts of interest.