
Abstract
Neurodegenerative disorders, chronic diseases that can severely affect the patient's daily life, include amyotrophic lateral sclerosis, Parkinson's, Alzheimer's, and Huntington's diseases. However, these diseases all have the common characteristic that they are due to degenerative irreversibility, and thus no efficient drugs or therapy methods can mitigate symptoms completely. Stem cell therapy, such as adipose tissue-derived stem cells (ADSCs), is a promising treatment for incurable disorders. In this review, we summarized the previous studies using ADSCs to treat neurodegenerative disorders, as well as their therapeutic mechanisms. We also suggested possible expectations for future human clinical trials involving minimized intracerebroventricular combined with intravenous administration, using different cell lineages to finish complementary therapy as well as change the extracellular matrix to create a homing niche. Depending on successful experiments in relevant neurodegenerative disorders models, this could form the theoretical basis for future human clinical trials.
Keywords
Introduction
Neurodegeneration results in chronic neurological diseases that can severely affect a patient's daily life and is therefore a burden in both developed and developing countries (86). With the growing aging population, the issues of cognitive and behavioral dysfunction are becoming more of a concern (47). New therapies are receiving a lot of attention in hopes that they can achieve symptomatic treatment of neurodegenerative disorders (28). In this review, we introduced the current knowledge of neurodegenerative disorders and their characteristics, as well as the benefits of stem cell transplantation focusing on the application of adipose tissue-derived stem cells (ADSCs) for neurodegenerative disorders. Further, we propose the possibility of cures using combined therapies and raise strategies for using complementary methods and identifying new potential therapeutic targets.
Neurodegenerative Disorders
Neurodegenerative disorders arise due to chronic progressive neuronal cell death, as well as loss of function due to myelin sheath deterioration or impaired neuronal transmission (13,20). Some form of abnormal cellular protein accumulation occurs in the central nervous system with most of the age-associated neurodegenerative disorders, such as amyotrophic lateral sclerosis (ALS), Parkinson's, Alzheimer's, and Huntington's diseases (34,83). These aggregations result from misfolding of proteins or polyglutamine-dependent pathogenesis (42,64). The pathogenesis of intracellular mechanisms includes impaired ubiquitin–proteasome and/or autophagy– lysosomal pathways (5,84), which can further give rise to membrane damage of organelles (85), and intrinsic mitochondrial apoptotic (16) and programmed cell death (82). The pathogenetic mechanisms of neurodegeneration are well known from many thousands of studies; however, due to their irreversibility and the lack of knowledge of what exactly causes the pathology, there are still no effective drugs or treatment methods available to restore symptoms completely.
Stem Cell Applications in Neurodegenerative Disorders
Recent progress has shown that cell replacement therapy of neural stem cells has potential therapeutic effects in most neurodegenerative disorders (11,43). Many kinds of stem cells can be differentiated into neuronal progenitors and then transplanted into the brain of animal models of disease to analyze their therapeutic potential (44,50,51). Cell-based therapies might be able to replenish lost cells and play a protection role below the neurodegenerative area, which may be to restore permanent paralysis and loss of sensation (11,78). It has been demonstrated that transplanted stem cells can integrate into the existing neural and synaptic circuits to achieve neurological functional recovery in many animal models of human neurodegeneration (8,9,43). Moreover, human clinical trials have tried to figure out what the roles of the transplanted stem cells in neuronal protection, replacement, and repair are (55). Thus, stem cell-based therapy should certainly be considered as a potential aid in alleviating and reversing symptoms of human neurodegenerative disorders (29).
There are well-known protective or functional improvement mechanisms of transplant therapy in neurodegenerative disorders, which are coupled with inflammatory moderation and antioxidant capacity (67). It has been shown that transplanted stem cells, via both an intracerebroventricular (ICV) or intravenous (IV) route, can differentiate into neuron-like or glia-like cells at the circumference of the injury region (24,72,81). Stem cells and differentiated neuronal cells can secrete neurotrophic factors to protect nerve cells, such as vascular endothelial growth factor (VEGF) (3), glial-derived neurotrophic factor (GDNF) (77), and basic fibroblast growth factor (bFGF) (48,62). Moreover, stem cell transplantation therapy has been shown to beneficially regulate the inflammatory response and antioxidant capacity in neurodegenerative disorders (14,52,79). In certain conditions, cell-based treatment has been shown to delay the syndromes of neurodegenerative disease and even reverse symptoms with prolonged survival in animal models of neurodegeneration (12,32,40).
ADSC Therapy in Neurodegenerative Disorders
It is self-evident that one problem with the use of autologous stem cells to treat neurodegeneration is the difficulty in obtaining a large number of neural progenitors without harming the patient. In 2001, Zuk et al. found that a wealth of ADSCs can be separated from liposuction surgery aspirate (88). ADSCs have been applied in several types of neurodegeneration, and their primary mechanism of action is the secretion of neurotrophic factors and chemokines to protect nerve cells after transplantation (59,60) (Table 1). In comparison to other adult stem cells, ADSCs were obtained more easily by a minimally invasive manner, and the patients are unlikely to undergo immune rejection of their own transplanted cells following transplant therapy (58). Prolonged culturing did not appear to alter the cell characteristics or result in tumor formation after transplantation (59). ADSCs have also been used in human trials of autoimmune diseases, multiple sclerosis, polymyositis, dermatomyositis, and rheumatoid arthritis, and thus, they could be a resource with good clinical applicability (22).
ADSC Application in Neurodegenerative Disorders
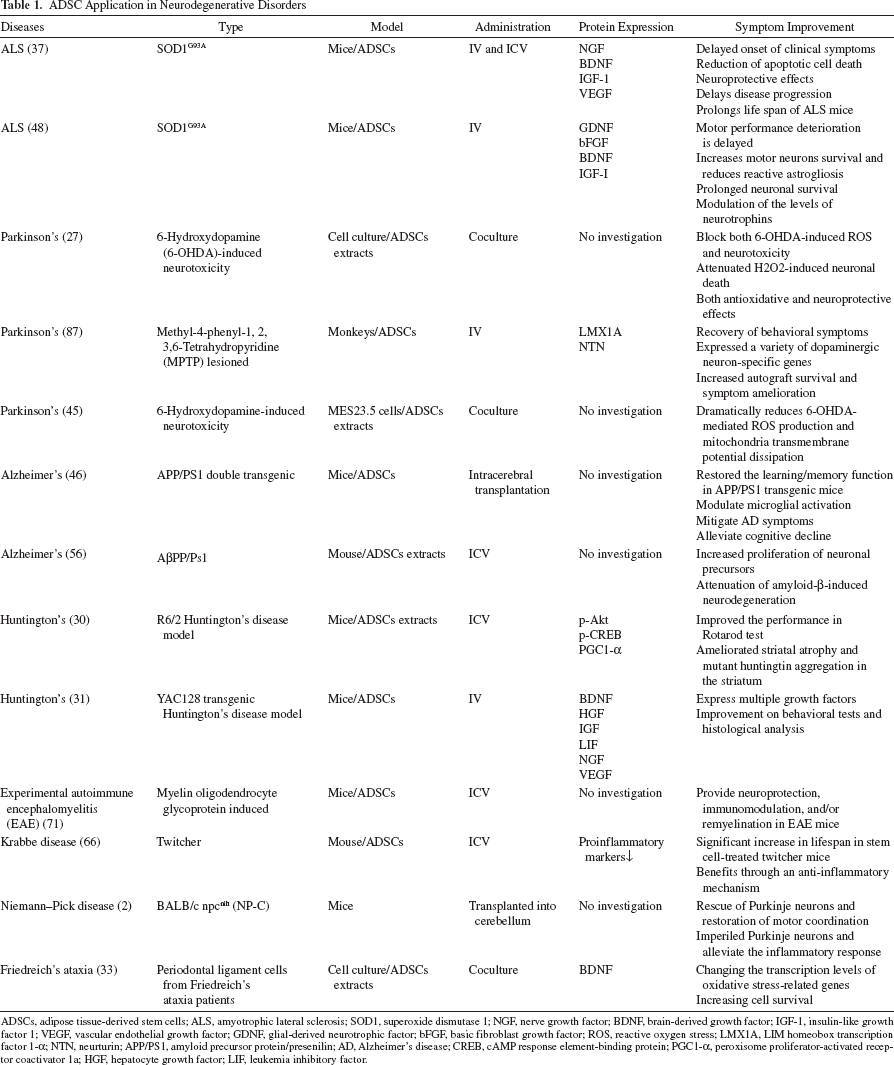
ADSCs, adipose tissue-derived stem cells; ALS, amyotrophic lateral sclerosis; SOD1, superoxide dismutase 1; NGF, nerve growth factor; BDNF, brain-derived growth factor; IGF-1, insulin-like growth factor 1; VEGF, vascular endothelial growth factor; GDNF, glial-derived neurotrophic factor; bFGF, basic fibroblast growth factor; ROS, reactive oxygen stress; LMX1A, LIM homeobox transcription factor 1-α; NTN, neurturin; APP/PS1, amyloid precursor protein/presenilin; AD, Alzheimer's disease; CREB, cAMPresponse element-binding protein; PGC1-α, peroxisome proliferator-activated receptor coactivator 1a; HGF, hepatocyte growth factor; LIF, leukemia inhibitory factor.
Amyotrophic Lateral Sclerosis
ALS is a degenerative disease of the nervous system, involving the death of both the upper and lower motor neurons (17). The disease normally progresses rapidly in the majority of patients, and the incidence of ALS is approximately 1.4/100,000 patients with an onset in the 50s (61,75). The major clinical manifestation is gradual muscle atrophy and weakness, as well as the resulting progressive failure of the neuromuscular system and eventually death (7). The pathological factors of ALS include familial genetic factors, reactive oxygen stress (ROS), abnormal protein aggregation, and excitotoxicity (17). Moreover, molecular mechanisms of motor neurodegeneration include impaired axonal transport and mitochondrial dysfunction as well as altered RNA processing (17). However, an effective treatment modality is still a mystery, and there are currently no effective therapies (36). ADSC transplantation has been widely used in various animal models of neurological deficit-related diseases, and thus it might be a potential therapeutic therapy for ALS.
Studies have investigated whether ADSCs can differentiate into neuron-like cells, and they demonstrate a significant improvement of symptoms and prolonged neuronal survival in G93A mutated superoxide dismutase (SOD1G93A) ALS mice (37). Presymptomatic ALS mice were transplanted with ADSCs via both ICV and IV routes, and the results showed delayed onset of clinical symptoms (37). After transplantation, increased neurotrophic factors such as nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), insulin-like growth factor (IGF-1), and VEGF, as well as abridged apoptotic cell death was observed (37). Another report also showed similar outcomes with significantly enhanced GDNF and bFGF, indicating that ADSCs might play a neuroprotective role as well as mitigate symptoms (48). These experimental data support a preliminary treatment in animal models with subsequent ALS efficacy trials.
Parkinson's Disease
The motor symptoms of Parkinson's disease are due to the death of dopaminergic neurons in the substantia nigra, as well as the interruption of the nerve conduction pathway (25). Parkinson's disease is commonly considered as a nongenetic disorder, but around 5% of individuals have mutations in specific genes and therefore reflect a genetic disorder (69). The main cause of Parkinson's disease in these individuals is α-synuclein gene mutations resulting in protein aggregation and ultimately the formation of Lewy bodies, Lewy neuritis, and cytotoxicity, which may induce spontaneous cell death (35). There is no efficient cure for Parkinson's disease; most treatments attempt to control and delay the state of the illness, such as by surgery and multidisciplinary management (80). Currently, the main treatment medications for Parkinson's disease include levodopa, anticholinergic agents, catechol-O-methyltransferase (COMT) inhibitors, dopamine agonists, and amantadine (15). Parkinson's disease is therefore another neurodegenerative disorder for which we need to find more efficient therapies.
A previous report indicated that the secretion of various cytokines and neurotrophic factors can help protect rat brains from 6-hydroxydopamine (6-OHDA), which normally causes specific degeneration of substantia nigra neurons and induced neurotoxicity (26). Therefore, in vitro cell culture systems have been used first to test whether the proteins secreted from ADSCs have the ability to confer protection from 6-OHDA (27). The results showed that ADSC-conditioned media could recover both 6-OHDA-induced ROS and neurotoxicity in rat mesencephalic neurons and cerebellar granule neurons, as well as straightforwardly attenuated H2O2-induced neuronal death (27). ADSC-conditioned media can also promote neurite regeneration in pheochromocytoma 12 (PC12) cells, while showing increased expression of bone morphogenetic protein 2 (BMP2) and fibroblast growth factor 2 (FGF2) (53). Moreover, ADSC implantation into hemiparkinsonian rhesus monkeys, made parkinsonian by methyl-4-phenyl-1, 2, 3, 6-tetrahydropyridine (MPTP) treatment, has neuroprotective effects (87). With improved protocols, the transplanted monkeys showed behavioral improvements and symptom amelioration (87). Thus, in the future, ADSCs might be a cellular resource of cells for autologous transplantation to treat Parkinson's disease.
Alzheimer's Disease
Alzheimer's disease is the most common type of dementia; it is multifarious and heterogeneous as it progresses and is generally known as a late-onset disease (76). The occurrence of dementia is expected to be up to 81.1 million in 2040. Genetic factors such as rare mutations in amyloid precursor protein (APP), apolipoprotein E, and presenilins (PS) represent <5% (18,76). New approaches such as genome-wide screening have found an additional 13 familial genes for Alzheimer's disease (21,63). With the complexity and uncertainty of this disease, there exists several opposing hypotheses, which have been proposed to explain the cause of the dementia including the cholinergic (19), amyloid (39), tau (10), myelin (4), and oxidative stress (73) hypotheses. The available treatments for dementia involve the categories of pharmaceutical, caregiving, and psychosocial, but these remain palliative in essence (23,41,57).
Current reports suggest that ADSCs may be a promising new cell source for regenerative cure, which can ameliorate the neuropathological deficits in Alzheimer's disease (46,56). Ma et al. showed that intracerebral administration of ADSCs has the potential efficacy to restore spatial learning/memory ability in APP/PS1 double transgenic mice (46). The improvements were believed to arise due to a dramatic reduction in amyloid-β aggregation, which is one of the fundamental pathologies of the disease, and also included learning and memory recovery. It was evident that administration of ADSCs could alter microglial activation, as well as mitigate dementia symptoms and alleviate the cognitive downturn. IV administration of ADSCs also palliated dementia symptoms and had therapeutic effects in another Alzheimer's disease mouse model (38). Pérez-González et al. investigated the issue of neurogenesis in the adult hippocampus (56). They proposed the possibility that leptin, an adipose-derived hormone, could promote neurogenesis, as well as its mechanism of action. The results indicated that the proliferation of neuronal precursors was increased in APP/PS1 double transgenic mice following leptin, as well as neuroprotective consequences. In summary, transplantation of ADSCs might have potential beneficial effects in preventing the pathological deterioration of Alzheimer's disease.
Huntington's Disease
A rare inherited disease, Huntington's disease, is a late-onset neurodegenerative genetic disorder, which is characterized by muscular coordination defects, cognitive decline, and spiritual illness (68). The disease arises from an autosomal dominant mutation that causes abnormal expansion of CAG in the huntingtin gene, resulting in the loss of the medium spiny neurons and the presence of nuclear inclusions in the basal ganglia. This abnormal CAG expansion leads to polyglutamine protein aggregation of the CAG repeat coding sequence, which ultimately leads to programmed cell death. The pathology mechanisms include activated apoptotic signals, abnormal glutamine function, as well as impairment of energy production and altered gene expression since misfolded mutant huntingtin causes a cellular toxicity (54,74). The clinical therapy of Huntington's disease consists of pharmaceutical and supporting treatment, which only relieve their symptoms and do not completely cure (1).
The potential therapeutic effects of administration of ADSCs have been investigated, and behavioral and histological analysis suggests that the symptoms of Huntington's disease are delayed (30,31,49). It has been shown that transplantation of ADSCs into YAC128 Huntington's disease transgenic mice led to the secretion of multiple paracrine growth factors (31). These protective factors were able to prevent apoptotic phenomena and recover the behavioral deficiency in animal models of the disease. An alternative method has been proposed from the same group in which they intraperitoneally injected cell extracts, instead of the direct transplantation of ADSCs into R6/2 Huntington's disease animals (30). Significant improvements in behavior exam, Rotarod test, as well as improved striatal atrophy and abnormal Huntington aggregation were observed, which may be regulated through the cAMP response element-binding protein-peroxisome proliferator-activated receptor-γ coactivator 1a (CREB-PGC1a) pathway. Various other animal models of Huntington's disease have also been generated to develop strategies for searching possible treatments (49). ADSCs could be tested in these additional models, and depending on the results of the rodent studies, they may support ADSCs as a clinically feasible source of cells for an autologous cell-based therapy for Huntington's disease.
Future Expectations
ADSCs are suitable for use as a treatment of human neurodegenerative disorders, due to their being easily isolated from adipose tissue as well as the ability to perform ex vivo expansion without losing the ability to differentiate into neuron-like cell lineages (22). Autologous ADSCs are being widely used in currently performed or ongoing human clinical trials. Previous clinical trials have indicated that ADSCs can be used for various diseases such as lipodystrophy, Romberg disease, depressed scar, breast deformities after lumpectomy, and Crohn's disease, but fewer trials were neurodegenerative disorder related (22). In the future for clinical applications, the manipulation method of ADSCs for administration should be improved since neurodegenerative disorders are chronic. The degenerative tissues may not possess a homing signal for transplanted cell targeting, as well as invasive administration of ADSCs would cause surgical injury (6). Thus, a good idea would be to perform minimized ICV administration of ADSCs, for creating a homing niche, combined with continuous IV injection to prevent invasive injury. Multiple cell lineages have been proposed as a treatment for multiple sclerosis, in order to complement the restrictions of a single cell type (65). It also has been reported that removal of chondroitin sulfate, an abundant extracellular matrix, could facilitate the ability of stem cells to interact with the host tissue for curing currently incurable neurodegenerative diseases (70). These data and improvements will allow ADSC clinical trials to be more feasible and may promote safety, thus promoting their great potential to develop into effective therapies for neurodegenerative diseases.
Footnotes
Acknowledgments
This work was supported by the National Science Council of the Republic of China (NSC 102-2320-B-039-011), Taiwan Department of Health Clinical Trial and Research Center of Excellence (DOH102-TD-B-111-004), Aim for the Top University Plan of the National Chiao Tung University and Ministry of Education, Cancer Research Center of Excellence (Taiwan), Ministry of Economic Affairs (102-EC-17-A-19-I1-0051), Industry-Academy Cooperation Office (102426AB), and MOHW103-TD-B-111-03. The authors declare no conflicts of interest.