
Abstract
We previously developed a collagen tube filled with autologous skin-derived stem cells (SDSCs) for bridging long rat sciatic nerve gaps. Here we present a case report describing a compassionate use of this graft for repairing the polyinjured motor and sensory nerves of the upper arms of a patient. Preclinical assessment was performed with collagen/SDSC implantation in rats after sectioning the sciatic nerve. For the patient, during the 3-year follow-up period, functional recovery of injured median and ulnar nerves was assessed by pinch gauge test and static two-point discrimination and touch test with monofilaments, along with electophysiological and MRI examinations. Preclinical experiments in rats revealed rescue of sciatic nerve and no side effects of patient-derived SDSC transplantation (30 and 180 days of treatment). In the patient treatment, motor and sensory functions of the median nerve demonstrated ongoing recovery postimplantation during the follow-up period. The results indicate that the collagen/SDSC artificial nerve graft could be used for surgical repair of larger defects in major lesions of peripheral nerves, increasing patient quality of life by saving the upper arms from amputation.
Introduction
Peripheral nerve repair with satisfactory functional recovery remains a great surgical challenge, especially for severe nerve injuries resulting in extended nerve defects. Although autologous nerve grafting is generally accepted as the gold standard for reconstructive strategies, the technique has inevitable drawbacks such as graft availability, donor site morbidity, and intolerable neuropathic pain; seeking alternatives to it has thus become a high priority (3,6,26). The combination of stem cell grafting with scaffold support has recently been developed for nerve repair and serves important roles in nerve growth and guidance. Neural stem cells (NSCs) can differentiate into supportive cells and contribute to promotion of axonal regeneration (2). However, the use of autologous Schwann cells or NSCs has several clinical limitations including a readily accessible source of these cells (8,16). Skin-derived stem cells (SDSCs) can regenerate nerves with nerve collagen guides (11), whereas bone marrow mesenchymal stem cells in vitro can express glial markers and induce nerve regeneration with glial growth (5,9,10,15,23). We hypothesized that the combination of autologous SDSCs as accessible sources of stem cells for nerve regeneration and collagen tubes aimed at restoring anatomical continuity of injured nerves would save from amputation of the upper arms of a patient with polyinjury to motor and sensory nerves.
Materials and Methods
Cell Culture
This study was approved by the Ethics Committee of the Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico di Milano (Milan, Italy; CR456-H). All cell preparation was completed in the Cell Factory of the Policlinico Hospital of Milan, which was formally certified in compliance with good manufacturing practice (GMP) standards in 2007 by the Italian Drug Agency (Agenzia Italiana del Farmaco – AIFA, Rome, Italy). Patient skin biopsy was performed on her left arm after informed consent was obtained, according to the guidelines of the Committee on the Use of Human Subjects of the Policlinico Hospital of Milan (Milan, Italy). Owing to the serious clinical conditions of the patient, we excised a larger portion of skin (about 4 cm2) in order to obtain a high cell number. Skin biopsy was made at the Fondazione Cà Granda Ospedale Maggiore Policlinico and released by the quality control unit according to Cell Factory internal procedure.
The medicinal product was released to an authorized investigator and transferred at 4°C with a data logger for temperature check in a specific storage box to the clinical center for infusion in the Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico di Milano. The Cell Factory and the clinical center are located within contiguous buildings. According to our unpublished stability results, a syringe containing cells can be stored at 4°C for a maximum of 6 h. All of the procedures of stem cell isolation were made in compliance with GMP regulations at the Cell Factory of the Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico di Milano.
The tissue was dissected and minced into smaller pieces using sharp razor blades. The specimen was washed with Earle's balanced salt solution (Life Technologies, Bethesda, MD, USA) and enzymatically dissociated with the addition of 0.2% collagenase type XI (Sigma, St. Louis, MO, USA) and 0.1% trypsin (Life Technologies) for 1 h at 37°C. The cell extract was filtered with a 70-μm nylon mesh (Dako, Carpinteria, CA, USA) and subsequently plated on noncoated flasks (Euroclone, Milan, Italy) to offer the advantage of isolating different populations of skin-derived cells. Preplate 1 (pp1) represented a population of skin-derived cells that adhered in the first 24 h after isolation and was highly enriched in fibroblasts. Preplate 2 (pp2), a population of skin-derived cells that did not adhere, was the target population. We counted 4.6 × 106 cells at pp2 (48 h after the first plating of skin-derived cells), and we let them proliferate for 7 days before the transplant. The growth medium was composed of Dulbecco's modified Eagle's medium/F-12 (1:1; Euroclone), 20% fetal bovine serum (Life Technologies), including 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) buffer (5 mM; Life Technologies), glucose (0.6%; Life Technologies), sodium bicarbonate (3 mM; Sigma), and glutamine (2 mM; Sigma). A hormone and salt mixture composed of insulin (25 μg/ml; Sigma), transferrin (100 μg/ml; Sigma), progesterone (20 nM; Sigma), putrescine (60 μM; Sigma), and sodium selenite (30 nM; Sigma) was also used. Mitogens, epidermal growth factor (20 ng/ml), and basic fibroblast growth factor (10 ng/ml) (murine recombinant; Chiron Corporation, Emeryville, CA, USA) were added to the medium. The growth medium was used to promote the proliferation of SDSCs used for the transplantation in the patient.
Flow Cytometry Characterization of Patient-Derived SDSCs
Patient-derived SDSCs were characterized in vitro by flow cytometry before transplantation. Cells were resuspended in phosphate-buffered saline (PBS; Sigma) and incubated with anti-cluster of differentiation 34-phycoerythrin-conjugated (CD34-PE), CD33-, CD38-, CD45- (all 1:10; BD – Becton, Dickinson and Company, Franklin Lakes, NJ, USA), anti-CD90 [thymocyte antigen 1 (Thy-1)]-fluorescein-isothiocyanate (FITC, 1:10; BD), anti-CD45-FITC (1:10; BD). Isotype-matched mouse immunoglobulin served as controls. After incubation was performed at 4°C for 20 min, the cells were washed in PBS containing 1% heat-inactivated fetal calf serum (FCS; Euroclone) and 0.1% sodium azide (Sigma). Finally, cells were analyzed using a FACS Cytomics FC500 and cxp 2.1 software (Beckman Coulter, BC, Brea, CA, USA). Each analysis included at least 5,000–10,000 events. A light-scatter gate was set up to eliminate cell debris from analysis.
Self-Maintenance and In Vitro Differentiation Potential of SDSCs
Self-maintenance and differentiation potential of human patient SDSCs isolated for transplantation were tested as previously described (11).
For the differentiation experiments, the SDSCs were plated on laminin-coated dishes (Sigma) in a B27 neurobasal medium supplemented with serum (Life Technologies).
Immunofluorescence staining was performed on cultured cells to test their neural differentiation properties. After fixation in 4% paraformaldehyde (Sigma), cells were incubated in blocking solution composed of 5% FCS and 2% human serum (Euroclone) in PBS for 30 min and with primary antibodies anti-nestin (1:50; BD) and anti-glial fibrillary acidic protein [GFAP; cyanine 3 (Cy3) conjugated, 1:100; Sigma]. Nestin was then detected using an Alexa Fluor 488-conjugated anti-rabbit IgG, secondary antibody (1:100; Molecular Probes-Life Technologies). Cell nuclei were stained with 4′,6-diamidino-2-phenylindole (DAPI, 1 μg/ml; Sigma). Cells were visualized by Leica DMIRE2 fluorescent microscope (Leica Microsystems, Wetzlar, Germany).
The NeuraGen® Nerve Guide
The NeuraGen® nerve guide (Integra Lifesciences, Plainsboro, NJ, USA) was used for nerve repair of an injured patient. This guide is a US Food and Drug Administration (FDA)-approved (Certificate Reference G7A091230790054, Reference Number EQ10123566) absorbable collagen tube designed as an interface between the nerve and the surrounding tissue and to create a conduit for axonal growth across a nerve gap. NeuraGen® nerve guides were filled with SDSCs (6 × 106 cells for the left median nerve graft and 7 × 106 cells for the left ulnar nerve graft).
Surgical Protocol in Animal Models
In preclinical experiments, 24 male nude rats (age 2 months, weight 170–200 g; Charles Rivers Italia, Calco, Italy) were submitted to sectioning of the sciatic nerve to create a gap of 1 cm, as previously described (11). All the experiments were performed in compliance with the NIH guidelines for Laboratory Animal Care. The experimental protocol was approved by Ministero della Salute, Italy (Permit Number: 6/10). Surgery was carried out in aseptic conditions with the aid of a microscope (Leica Microsystems). Anesthesia was induced by an intraperitoneal injection of chloral hydrate (2 ml, 6.25%; LGC Standards, Teddington, London, UK). In 12 rats (control group), the sectioned sciatic nerve was reconnected using the NeuraGen® guide without SDSCs. In another 12 operated rats (experimental group), the sectioned sciatic nerve was reconnected using NeuraGen® tubes filled with 5 × 105 SDSCs. Animals were sacrificed at 30 (n = 6 per each group) and 180 days (n = 6 per each group).
Histological Staining of Treated Animals
For morphological analysis, specimens were fixed in 4% glutaraldehyde (Sigma) in phosphate buffer for 24 h. After dissection and postfixation in 2% osmium tetroxide (Sigma) for 1 h, the specimens were dehydrated and embedded in Spurr resin (Sigma). Morphologic analysis was performed on 0.5-μm semithin sections stained with toluidine blue (Bio-optica, Milan, Italy), using a computer-assisted Leica light microscope (Leica Microsystems).
Immunofluorescence Analysis of Treated Animals
Immunofluorescent staining of tissue was done at 30 and 180 days after surgery. Sciatic nerves were removed, fixed in 4% paraformaldehyde for 2 h, dehydrated in 30% sucrose (Sigma) overnight, frozen in liquid nitrogen-cooled isopentane (Sigma), and stored at −80°C until sectioning. Both longitudinal and transverse sections of 10 μm thickness were cut on a cryostat (Leica Microsystems). Sections were fixed in 4% paraformaldehyde for 4 min, incubated in blocking solution (Life Technologies) for 30 min, and with primary antibodies anti-laminin (1:50; Sigma) and anti-neurofilament-180 (NF180, 1:50; Chemicon, Billerica, MA, USA), incubated with the Alexa Fluor 488-conjugated anti-rabbit IgG secondary antibody (1:100; Molecular Probes-Life Technologies). Grafted cells were detected by immunofluorescence assays for human lamin A/C-positive cells with polyclonal anti-human lamin A/C (1:50; Molecular Probes) followed by Alexa Fluor 488-conjugated anti-mouse IgG (1:100; Molecular Probes-Life Technologies). Cell nuclei were stained with DAPI. Slides were analyzed using a Leica TCS-SP2 confocal microscope (Leica Microsystems).
Case Report and Surgical Procedure
In October 2009, a 23-year-old female was admitted to the emergency unit of the Policlinico Hospital of Milan, after polytrauma of the upper arms and head. The patient presented with hemorrhagic shock due to multiple knife-induced open wounds in the arms, left interscapular region, left lumbar region, and head. A brain CT scan revealed the presence of extradural hematomas. The patient immediately underwent two neurosurgical operations because of intracranial lesions and also combined surgical interventions by vascular and trauma surgeons to repair the severe bone and vessel damage. At the neurological examination, 1 month after the event, the patient was alert, awake, and oriented. Cranial nerve deficits were not present. The motility of the lower limbs was good, while radial nerve palsy was detected in the upper right limb together with an upper left limb monoplegia. Almost full anesthesia was detected in the left upper limb, while hypoesthesia at the volar, dorsal, and lateral sides was present in the right one. Deep tendon reflexes were absent in both upper limbs. Neurophysiological data over time [electromyography (EMG) and nerve conduction studies (NCSs) (20)] are reported in Tables 1 and 2. The extent of the nerve lesions and the severity of the clinical picture meant that the probability of a spontaneous and efficient recovery of both motor and sensory functions of the upper limbs (especially on the left side) was extremely low. Owing to the urgency of the clinical case and based on our preclinical experiences (11), we opted for compassionate use of NeuraGen® guides filled with autologous SDSCs, in agreement with the Ethic Committee of the Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico of Milan and after the collection of informed consent. Then, the patient underwent new neurosurgical operation.
The right radial nerve was found interrupted for a length of 5 cm over the elbow; it was rejoined using the left sural nerve. The left radial and median nerves were interrupted between the arm and the forearm for a length of 8–10 cm. Two 3-cm collagen guides (NeuraGen®) were filled with autologous stem cells (Fig. 1) and positioned at the proximal and distal portion of the stumps. A sural nerve graft was then interposed between the two guides. This procedure was performed for both the median and radial nerves. The choice of using the SDSCs only in the left arms was made after checking the gap length, which was longer than that for the right nerves and to improve the classic surgical approach, which is known to be less efficacious in such long lesions.
Neurosurgical intervention to repair the polyinjured major peripheral nerves. Polyinjured motor and sensory nerves of the upper arms of the patient. Posttraumatic neuroma formation was found during surgical procedures before positioning the NeuraGen® nerve guide (A). During neurosurgical intervention, the NeuraGen® nerve guide filled with autologous SDSCs (B) was inserted as an interface between the nerve and the surrounding tissue and to create a conduit for axonal growth across a nerve gap (C, D). MRI sequences in T1 showed the absence of tumor or adipose tissues in the left arm 6 (E) and 18 months (F) after the treatment.
Assessment of Outcome
The patient was followed up by neurological clinical examination, MRI, and electrophysiological studies every 2 months after the treatment for 3 years. NCSs and needle EMG of both upper limbs were performed systematically over a period of approximately 2 years. Sensory NCSs of the median, ulnar, and radial nerves were performed using antidromic techniques, with surface-stimulating and recording electrodes. Skin temperature at the hand was maintained at greater than 31°C. Sensory nerve action potential (SNAP) amplitude was measured from the peak of the negative wave to the peak of the following positive wave (peak-to-peak amplitude), and SNAP latency was measured at the peak of the negative wave. Motor NCSs of the median, ulnar, and radial nerves were conducted using standard techniques. The median nerve was stimulated at the wrist and antecubital fossa, recording from the abductor pollicis brevis. We stimulated the ulnar nerve at the wrist and just below the ulnar groove at the elbow, recording from the abductor digiti minimi. The radial nerve was stimulated near the antecubital fossa and at the spiral groove, recording from the extensor indicis. Measurements included distal and proximal compound muscle action potential (CMAP) negative amplitudes and distal CMAP latency and motor conduction velocity. Needle EMG was performed on several muscles innervated by the median (opponens pollicis), ulnar (first dorsal interosseous), and radial nerves (extensor digitorum, extensor indicis) of both sides.
Results
Isolation and Characterization of Patient-Derived SDSCs
The SDSCs isolated from the skin biopsy of the patient grew as floating clusters of cells with morphological resemblance to spheres. They were lineage negative (CD33-, CD38-, CD45-), CD34-, Thy 1+, and possessed clonal capacity as previously described (11). The spheres were positive for nestin, the major cytoskeletal protein expressed in neuronal progenitors, and were able to differentiate into the GFAP astroglial cell type (Fig. 2A, B). Moreover, single cell-derived primary SDSC spheres generated clonally derived secondary spheres capable of producing, after their dissociation, tertiary spheres, which could be differentiated into either glia or Schwann cells. All of these data demonstrated the stem cell characteristics of the patient-derived SDSCs.
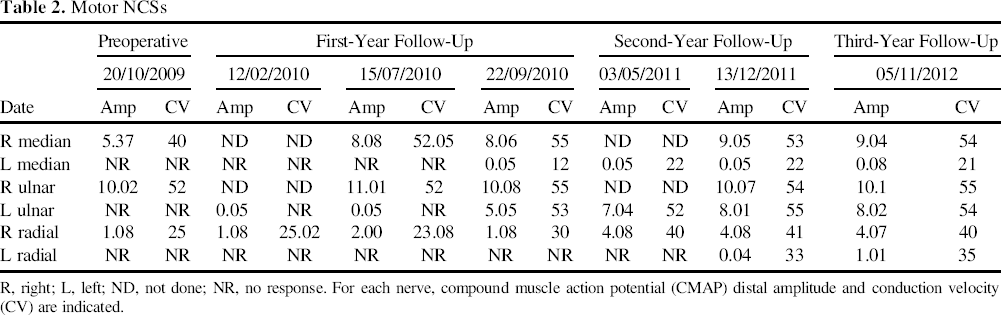
Patient-derived SDSCs in culture in proliferative medium and after transplantation in rodents. A floating cluster of cells with morphological resemblance to spheres (A) (magnification: 10×). SDSCs express the glial cell marker glial fibrillary acidic protein (GFAP; red), when cultured in differentiation medium as confirmed by immunostaining (B) (magnification: 20×). At 180 days, qualitative analysis of nerve sections stained with toluidine blue showed that grafted patient-derived SDSCs led to reconnection of the sectioned sciatic nerve (C–F) [magnification: 10× (C–E); 40× (D–F)]. An enhancement in SDSC migration was observed away from the proximal stump, as was advanced linear axonal regrowth in the nerve guide-treated animals. Indeed, after 6 months, the diameter of the conduit was considerably reduced (E). SDSC transplantation immunofluorescence analysis was positive for NF180 (red in G) (magnification: 20×) and laminin (red in H) (magnification: 20×). Human lamin A/C cells were found around nerves (green in detail of H) (magnification: 63×). Nuclei are shown with blue staining [4′,6-diamidino-2-phenylindole (DAPI)]. Motor NCSs R, right; L, left; ND, not done; NR, no response. For each nerve, compound muscle action potential (CMAP) distal amplitude and conduction velocity (CV) are indicated.
Preclinical Experiments Revealed no Side Effects of Patient-Derived SDSC Transplantation and Showed Rescue of the Sciatic Nerve in an Animal Model
To evaluate cell transplantation safety, we injected NeuraGen® filled with SDSCs or without as a control into the lesioned sciatic nerve of nude rats as previously described (11). Neither septic collections nor tumorigenesis was observed in any treated animals at the site of treated nerves at 30 and 180 days after treatment. At 30 days, animals treated with NeuraGen® tubes filled with patient-derived SDSCs showed correct connections of lesioned nerves, whereas animals treated with only NeuraGen® tubes showed a thin fibrous reaction around connections without a thorough integration (toluidine blue staining; Fig. 2C to F). At 180 days after treatment, the NeuraGen® tubes were completely reabsorbed. Moreover, no signs of automutilation were recorded in the groups of animals treated with NeuraGen® tubes filled with patient-derived SDSCs, demonstrating the absence of dysesthesia or hyperpathia. In order to confirm the neuroregenerative potential of human SDSCs into the lesioned sciatic nerve, we characterized the transplanted NeuraGen® filled with or without SDSCs for the presence of myelinated nerve fibers. We found presence of myelinated fibers only in the NeuraGen® filled with SDSCs (Fig. 2C–F). Confocal microscopy analysis indicated the presence inside the guide of a fraction (estimated in the range of 30% of total cells inside the guide) of nerve fibers labeled with anti-NF180 and anti-laminin antibodies (Fig. 2G, H). Several human lamin A/C-derived SDSCs were found inside and around reconnected sectioned sciatic nerves (Fig. 2H).
Clinical Assessment
Before treatment, the patient was unable to move the hands, arms, and forearms. The postsurgery course was regular, and neither vascular nor infectious complications arose in the limbs. After the procedure, the patient underwent hyperbaric therapy. The patient never suffered neurogenic pain after treatment. Serial MRI sections of the arms and brachial plexuses excluded the presence of any nerve tumor and showed an absence of adipose degeneration of muscles (Fig. 1E, F).
The last neurological examination, 3 years after the polytrauma, showed normal trophism, especially in the right shoulder, arm, and forearm, while the right hand showed hypotrophic interosseous, thenar, and hypothenar muscles (Fig. 3A). Contraction of the right finger flexors and extensors with partial movement of the right hand [M1, according to the British Medical Research Council (MRC) grading system] (13) was found during the 3-year follow-up (supplementary videos: S1a, http://youtu.be/LvwQc1zLWxw; S1b, http://youtu.be/r3SlgeVAFrc; S2a, http://youtu.be/6JoQZmeV8I0; S2b, http://youtu.be/AO8spKmvSfY; S3, http://youtu.be/aDUatZvyRoE).
Neurological examination 3 years after the polytrauma. The last neurological examination, 3 years after the polytrauma, shows normal trophism, chiefly in the right arm (A). The patient was able to retain a paper sheet, a pen, and a pair of glasses between the first and second fingers (B–D).
Sensory Nerve Conduction Studies (NCSs)

R, right; L, left; ND, not done; NR, no response. For each nerve, sensory nerve action potential (SNAP) amplitude and latency are indicated.
Electrophysiological Evaluations Showed Repaired Motor and Sensory Pathways
Sensory and motor NCS data of the right median and ulnar nerves before and after treatment were higher than the left counterpart. The SNAP and CMAP of the remaining nerve were of a reduced amplitude or were absent before the treatment and slowly increased after treatment with a prevalence in the right side. The results of sensory and motor NCSs are summarized in Tables 1 and 2, where the SNAP and CMAP changes over time are underlined. Acute and chronic denervation was detected in the muscles innervated by the left median and ulnar nerves and both radial nerves.
Discussion
The assumption in peripheral nerve injury has been that peripheral nerve injuries recover, as opposed to those of the central nervous system. Although peripheral nerves do regenerate better, recovery is frequently incomplete, misdirected, or associated with debilitating neuropathic pain (22). In particular, nerve transection is associated with notoriously poor outgrowth compared with crush or other injuries, especially with longer distance between the injury and target (muscles, skin). Regenerating axons face both a challenging nerve gap and a distal denervated nerve environment where Schwann cells become increasingly less able to support axon regeneration with prolonged denervation. Nerve grafts provide a pathway for regenerating axons from the proximal nerve stump to innervate the distal stump (14); unfortunately, however, recovery after nerve or nerve graft repair is limited by incomplete regeneration and variable clinical results (4). Poor outcome from peripheral nerve injury is especially evident when repair is delayed (17,18,21). Schwann cell infusion has been successful in promoting regeneration and remyelination in animal models of the injured spinal cord and peripheral nerves (19,27,28). To serve as a realistic therapy, candidate transplant cells should be easily accessible, rapidly expandable in culture, capable of survival and integration within host tissue, and amenable to stable transfection and expression of exogenous genes. The skin and its associated structures offer an easily accessible source of stem cells. A large population of neural crest stem cells has been found in the bulge area of hair and whisker follicles that can differentiate into neurons, smooth muscle cells, Schwann cells, and melanocytes (1,7, 20). In previous work, we transplanted stem cells derived from skin into artificial nerve guidance tubes bridging a 16-mm gap in the rodent sciatic nerve, demonstrating improvement over vehicle control in behavioral, electrophysiological, and morphological parameters measured (11). The skin dermis contains neural crest-related precursor cells [termed skin-derived precursors (SKPs)] that can differentiate into neural crest cell types in vitro, including those with characteristics of peripheral neurons and Schwann cells, when supplied the appropriate cues (7). SKPs have been generated in neonatal and adult skin of rodents (25) and humans (12,24), responding to environmental cues in a similar manner. Here we translated these findings to promote nerve repair in a polyinjured patient by using autologous SDSCs, easily procured, via relatively noninvasive skin graft harvesting and placed in a NeuraGen® FDA-approved nerve guide. A graft made of biodegradable materials is a promising alternative for promoting successful long-term recovery, as has been confirmed both experimentally and clinically; after serving as an appropriate scaffold for regeneration, the conduit eventually degrades, as we confirmed here in the animal model at 180 days. EMG testing 1 year after surgery showed an improvement in the motor function of the ulnar and in minor branches of the left median nerves, amelioration of sensory stimulus of the right radial nerve, increased blockade of the right radial nerve motor conduction at the elbow (probably because of a hypertrophic keloid), and reduced active denervation in the examined muscles (especially in the left arm, which had developed fibrotic tissue in muscles innervated by the median and radial nerves). Three years after the intervention, EMG showed an improvement in sensory (detectable SNAP, although still of increased latency and reduced amplitude) and motor (detectable CMAP) conduction in the left ulnar nerve as well as right radial nerve and a better motor conduction in the right radial nerve. We thus combined the use of nerve guides and stem cells to promote nerve regeneration over longer gaps, highlighting functional recovery in a polyinjured patient. It remains to be determined whether the extent of this partial restoration of motor and sensory perception can be further improved. This report is the first case of a combinatorial approach using stem cells and a nerve guide for partial sensory and motor restoration with a valuable salvage of arms from amputation. We confirmed the feasibility of administering autologous SDSCs filled in the nerve guide for repairing polyinjured motor and sensory nerves of the upper arms of a patient. The 3-year follow-up has witnessed nerve regeneration with suitable functional recovery in the patient and salvage from upper arm amputation. This finding opens an alternative avenue for patients that risk arm amputation after important nerve injuries.
Footnotes
Acknowledgments
This work was supported by the Associazione Amici Centro Dino Ferrari and the Italian Ministry of Health (GR-2008–1146615). The funding source had no roles in study design; in the collection, analysis, and interpretation of data; in writing the report; and in the decision to submit the paper for publication. Y.T. had the full access to all data in the study and the final responsibility for the decision to submit publication. The authors declare no conflict of interest.