
Abstract
Insufficient donor nerve graft material in peripheral nerve surgery remains an obstacle for successful long-distance regeneration. Schwann cells (SCs) can be isolated from adult mammalian peripheral nerve biopsies and can be grown in culture and retain their capacity to enhance peripheral nerve regeneration within tubular repair strategies in multiple animal models. Human Schwann cells (hSCs) can be isolated, expanded in number, and retain their ability to promote regeneration and myelinate axons, but have never been tested in a clinical case of peripheral nerve injury. A sural nerve biopsy and peripheral nerve tissue from the traumatized sciatic nerve stumps was obtained after Food and Drug Administration (FDA) and Institutional Review Board (IRB) approval as well as patient consent. The SCs were isolated after enzymatic digestion of the nerve and expanded with the use of heregulin β1 (0.1 μg/ml) and forskolin (15 mM). After two passages the Schwann cell isolates were combined with sural nerve grafts to repair a large sciatic nerve defect (7.5 cm) after a traumatic nerve injury. The sural nerve and the traumatized sciatic nerve ends both served as an excellent source of purified (90% and 97%, respectively) hSCs. Using ultrasound and magnetic resonance imaging (MRI) we were able to determine continuity of the nerve graft repair and the absence of tumor formation. The patient had evidence of proximal sensory recovery and definitive motor recovery distal to the repair in the distribution of the tibial and common peroneal nerve. The patient did experience an improvement in her pain scores over time. The goals of this approach were to determine the safety and clinical feasibility of implementing a new cellular repair strategy. In summary, this approach represents a novel strategy in the treatment of peripheral nerve injury and represents the first reported use of autologous cultured SCs after human peripheral nerve injury.
Introduction
Major advances made in the field of peripheral nerve surgery and repair occurred in the midportion of the 20th century with the wartime experiences of Seddon 1 . He was the first surgeon to use autologous sensory nerve grafts to bridge gaps in the peripheral nervous system. While this technique has its own set of shortcomings—including sensory loss at the donor site, possible neuroma formation, and a lack of sufficient graft material in the repair of the large diameter nerves (e.g., sciatic nerve)—it has become the gold standard. A common candidate nerve for autologous grafting is the sural nerve, a “nonessential” sensory nerve2,3. It has a cross-sectional area 15 to 20 times less than that of the sciatic nerve 4 . When both lower extremity sural nerves are harvested, donor graft material is exhausted at about 6 cm of sciatic nerve gap 4 . Clinical data from nerve grafts bridging gaps of the sciatic nerve greater than 5 cm indicate that the prognosis for functional recovery is poor 5 .
Currently there are 11 Food and Drug Administration (FDA)-approved conduits 6 . Multiple reports are available in the literature of successful nerve repair using stand-alone axon guidance channels (AGCs). These reports focus on small-diameter nerves and tend to bridge short gaps7–11. The use of these AGCs for larger gaps in large-diameter nerves appears to be less effective 12 . Supplementation of AGCs with growth-enhancing substrates has also been studied. These include nerve growth factor (NGF), brain-derived neurotrophic factor (BDNF), glial growth factor (GGF), denatured muscle, small segments of peripheral nerve, and most recently purified Schwann cells (SCs)13–29. Adding autologous SCs suspended in serum within a collagen tube significantly enhanced the gap distance that can be repaired after a long segmental nerve defect in the sciatic nerve of rats 30 .
Contributions and discoveries in the last few decades that have made this possible in humans include: 1) the ability to isolate SCs in culture from adult human nerve31,32, 2) the ability to induce human Schwann cells (hSCs) to divide in response to mitogen (heregulin β1/forskolin) so that millions of SCs can be grown from a small nerve biopsy33–36, 3) establishing that the cultured hSCs when isolated and driven to divide with mitogens can still function by promoting regeneration and forming myelin32,33,37,38, and 4) proving that these stimulated human cells do not go on to produce tumors in vivo, thus further establishing their safety 39 . Since these advances, SC transplantation has continued to be studied in the setting of peripheral nerve injury. The addition of SCs to AGCs has been demonstrated to enhance axonal regeneration and improve functional recovery in mice, rats, and in nonhuman primates25,30,33,40,41. When combined with the extensive preclinical data submitted for FDA approval of autologous hSCs (ahSCs) for subacute thoracic spinal cord injury (SCI), the record for safety of autologous hSC transplantation is extensive 42 .
The case presented here is uncommon, devastating, and limb threatening and represents the worst case scenario in nerve injuries. Using an approach that combines standard sural nerve graft repair and supplemental cultured SCs, we repaired a large sciatic nerve defect (7.5 cm). The goals of this approach were to determine the safety and clinical feasibility of implementing a new cellular repair strategy. In addition to realizing the technical aspects of the nerve repair we were able to define and compare traumatized nerve ends and sural nerves as sources of SCs. In summary, this approach represents a novel strategy in the treatment of peripheral nerve injury and represents the first reported use of autologous cultured SCs after human peripheral nerve injury.
Materials and Methods
Case History
A 25-year-old female sustained multiple deep, lacerating wounds to her right posterior thigh (Fig. 1), including the gastrocnemius muscle, quadriceps, and Achilles tendon as she was run over by a boat propeller. She went immediately to the trauma operating room for her life-threatening injuries to debride her posterior thigh musculature, control the vascular injury, and explore the sciatic nerve, which was completely transected. At the time of initial debridement of the sciatic nerve ends, a small (0.5 cm) segment of nerve was kept in Belzer UW® (Bridge to Life, Columbia, SC, USA) solution. She endured a total of four additional surgeries over a period of a month including: 1) thigh wound washout—debridement of necrotic muscle, 2) Achilles tendon repair and sural nerve graft (5 cm) harvest for the preparation of autologous hSCs, 3) anterior quadricep washout and tendon repair, and 4) skin grafting to posterior thigh.

Intraoperative view of transected sciatic nerve at time of exploration in the trauma operating room demonstrating significant nerve loss. Thirty days after initial exploration for definitive repair, a 7.5-cm gap between nerve endings was revealed. This was due to resection and retraction of scarred nerve ends. Distal ends of the sciatic nerves were held by forceps. Proximal side indicated by asterisk.
Ethical and Legal Approvals
We filed simultaneously for FDA approval [expanded access to Investigational New Drug (IND) 14856 for a single patient] and for Institutional Review Board (IRB) approval (protocol #20130722), and then obtained consent from the patient and family to supplement traditional sural nerve graft repair with autologous hSCs.
Isolation of Sciatic and Sural Nerve Segments
To prevent retraction of the nerve ends, epineurial sutures were placed and attached in the adjoining muscle. A small piece of nerve tissue (0.5 cm) from traumatized sciatic nerve ends was placed in Belzer solution, refrigerated at 4°C, and transported to the cell-manufacturing laboratory (cGMP facility) for cell culture. The facility at the University of Miami consists of a 2,500-square foot area of space under HEPA-filtered air conditioning certified to meet ISO-Class 7 (ISO 14644) standards, and a general laboratory area certified to meet ISO-Class 8. Three days later, during the repair of the patient's Achilles tendons, she underwent a right-sided 5-cm sural nerve biopsy. The sural nerve harvested was distal to the main area of sciatic nerve injury in the thigh and thus represented nerve that was already denervated. The boat propeller injury at the level of the Achilles tendon also cut the sural nerve. The amount of nerve harvested represented a very small portion of the total bilateral (both legs) sural nerve harvested at the time of sciatic nerve repair [5 cm/(12 × 7.5 cm) + 5 cm] = 5.3%.
Cell Culture Methods
The sural nerve (5 cm) and sciatic nerve biopsy (0.5 cm) were dissected, and fascicles were pulled from the epineurium and transferred to a triangular T-75 flask (Corning, Oneonta, NY, USA) (Fig. 2). The flask was placed in an incubator at 37°C with 8% CO2. Culture medium (CM), which contained 1× Dulbecco's modified Eagle medium (DMEM; Life Technologies, Grand Island, NY, USA), 10% fetal bovine serum (FBS; Hyclone, GE Healthcare Life Sciences South Logan, UT, USA), 2 mM forskolin (Sigma-Aldrich, St. Louis, MO, USA), 10 nM human recombinant heregulin β1 (Genentech, South San Francisco, CA, USA), 4 mM L-glutamine (Life Technologies), 0.064 mg/ml gentamicin (APP Pharmaceutical/Fresenius Kabi USA, Lake Zurich, IL, USA), was changed every other day. On day 7 for sciatic and day 5 for sural nerve, the dissociation enzyme solution (5 ml) that contained neutral protease NB (2 DMCU/ml; SERVA Electrophoresis GmbH, Heidelberg, Germany), collagenase NB1 (0.5 PZU/ml; SERVA Electrophoresis GmbH) in 1× high-glucose DMEM (Life Technologies) supplemented with 3.1 mM CaCl2 (International Medication Systems Limited, South El Monte, CA, USA) was added to the fascicles and placed inside the incubator at 37°C with 8% CO2 for 18 h. The fascicles were dissociated, and D-10 (Life Technologies) (10 ml) was added to the flask containing the fascicles, and it was centrifuged at 150 × g for 5 min at 4°C to pellet the cells. The cells were then washed two more times and plated onto mouse laminin-coated (1 μl/cm2, with a stock concentration of 1 mg/ml; Sigma-Aldrich) plates using the CM. The cells were fed with CM every 3 days. After 7 days, cells reached 80% confluence for both nerve preps. One of the 636-cm2 chambers (Corning) for sural SC cultures was found to be contaminated with Aspergillus fumigatus and discarded. The viable cell count of sural nerve was 19.2 million cells and of the sciatic nerve was 10 million cells. The SC purity by immune staining for sural nerve was 90.2% (Fig. 3A) and sciatic nerve was 97% (Fig. 3B). The final cell product was washed three times to remove mitogens, laminin, and bovine products. Several controls were employed throughout the manufacturing process to ensure that the product was essentially free of process-related contaminants. These controls included the wash steps described above and release testing of the final product. Investigations into the potential related impurities of the manufacturing process had been conducted during process validation studies at the time of our IND #14856 submission. The samples were analyzed for residual levels of heregulin β1 peptide, mouse laminin, gentamicin, and bovine serum albumin.

Schematic diagram demonstrating the process of SC harvesting and expansion in culture to repair the injured sciatic nerve. Small peripheral nerve segments from the 5-cm sural nerve biopsy were collected, placed in cell culture, and expanded using mitogens (heregulin and forksolin) and ultimately transplanted back into a long segment (7.5 cm) sciatic nerve defect along with sural nerve autografts.
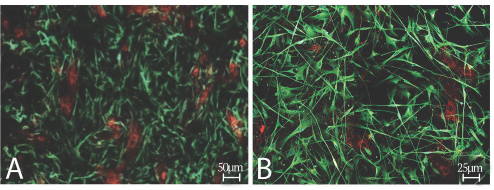
ahSC culture from sural (A) and sciatic nerve (B) indicating purity by immunostaining at 90.2% and 97%, respectively. hSCs were stained with antibodies to S100 (green), and fibroblasts were stained for fibronectin (red). Scale bars: 50 μm (A), 25 μm (B).
SCs were plated onto laminin-coated four-well glass chamber slides at 50,000 viable cells per well and fixed the following day with 4% paraformaldehyde (Electron Microscopy Sciences, Hatfield, PA, USA), and fixed slides were stored at +4°C for immunostaining. For identification of hSCs, an intracellular protein called S100 was used. S100 is normally present in cells derived from the neural crest (i.e., SCs, melanocytes, and glial cells) as well as chondrocytes, adipocytes, myoepithelial cells, macrophages, Langerhans cells, dendritic cells, breast epithelial cells, and keratinocytes. Within the peripheral nerve tissue, it is the only type of cell that expresses S100 protein. For identification of S100 protein in the human SCs, an anti-human S100 (final dilution 1:200; Dako, Dallas, TX, USA) primary antibody was used. Also, to identify the second major cell type that is a constituent in the SC, we used a protein called fibronectin, which is abundantly present in fibroblasts in contrast to human SCs. For identification of fibronectin protein, an anti-fibronectin (final dilution 1:200; Santa Cruz Biotechnology, Santa Cruz, CA, USA) as a primary antibody was used. During the immunostaining procedure, one well of the four-well slide was kept as a negative control, which received only the secondary antibodies. The secondary antibodies used were the solution of Alexa 488 goat anti-rabbit IgG and Alexa 594 goat anti-mouse IgG (Life Technologies) diluted (1:200) in 1.5% normal goat serum and 1× DPBS (Life Technologies). The other three wells of the four-well slides were stained with both the primary and the secondary antibodies. All wells received Hoechst nuclear marker (final dilution 1:1,000; Life Technologies). Fluorescent images were taken using the fluorescent microscope. Mycoplasma (PCR) test was negative for both sural and sciatic SCs. The final endotoxin levels were 0.87 EU/kg for the sural nerve source and 0.7 EU/kg for the sciatic nerve. Two Gram stains were done on both the final product and mixed product with serum, as part of lot release, and then a second Gram stain was done on the mix, all of which were negative. Posttransplant sterility results after 14 days of culture were also negative for aerobic, anaerobic, and fungal organisms. The total SC count injected was 28.8 million at a concentration of 100,000 cells/μl with greater than 99.9% viability. Cells were placed on ice to transport to the operating room for transplantation.
Method of Transplantation
Definitive surgical repair of the sciatic nerve defect took place 30 days postinjury and consisted of harvesting of bilateral sural nerve and placement of 12 × 7.5-cm nerve grafts sutured with 7-0 prolene to the sciatic nerve stumps supplemented by 29 million autologous hSCs placed within an FDA-approved collagen matrix (Duragen®; Integra LifeSciences Corporation, Plainsboro, NJ, USA) wrap (Fig 4A–F). Duragen® Secure Dural Regeneration Matrix is an absorbable implant used for the repair of dura mater. This absorbable, sutureless only graft is comprised of a porous, highly purified collagen matrix and a thin layer of hydroxypropyl methyl cellulose (HPMC). HPMC is a non-cytotoxic, nonimmunogenic, biocompatible plant-derived cellulose-based material. The hSC preparation was layered across the sural nerve grafts.

Schematic diagrams (A–F) demonstrating the method of augmenting sural nerve graft repair of the sciatic nerve with autologous hSCs. On the left are line drawings and on the right actual intraoperative images. (A, B) Sural nerve repair with Duragen graft® in background. (C, D) Nerve construct is then supplemented by hSCs. (E, F) Duragen graft® is sewn around nerve/hSC construct.
Postoperative Follow-up
The patient was serially tested for motor and sensory function according to the Medical Research Council (MRC) grading scale 43 . Additionally, postoperative ultrasounds were performed to assess continuity of the grafts.
Results
At time of injury and preoperatively, the patient had complete sensory loss to pinprick and light touch without allodynia (Fig. 5A), and absence of motor (0/5) function distal to the innervation of the knee flexors (biceps femoris/semimembranosus and semitendinosus), which still contracted against gravity (3/5). This pattern of injury was consistent with a complete transection of the sciatic nerve at the upper thigh.

Sensory diagrams to pin prick at time of injury (A) and at 15-month (B) follow-up, demonstrating recovery in proximal superficial aspect of the peroneal nerve.
There were no postoperative complications with the nerve harvest and sciatic nerve repair with the posterior thigh, but the patient required a debridement of the anterior quadricep wound for a staphylococcus (MSSA) infection supplemented by antibiotics. The leg was immobilized for 2 months with a knee immobilizer to allow for healing of her anterior quadriceps. The patient had a brief period of formal physical therapy (4 weeks) after she came out of her knee brace. She continued to do Pilates and exercises at home to maximize her recovery. She wore an ankle–foot orthosis following her trauma. As per protocol, the patient underwent serial neurological assessments at 3-month intervals as well as magnetic resonance imaging (MRI; not shown) and ultrasound (Fig. 6) imaging postoperatively at 6 and 12 months. The patient underwent fat grafting to provide tissue bulk over her soleus and cosmetic revision of her skin graft site.

Sagittal (long axis) ultrasound of sciatic nerve 3 months after surgical repair indicating continuity of the grafts to both sciatic nerve ends.
The patient's neurological exam gradually improved so that at 15 months (Fig. 5B) she had demonstrated recovery of sensitivity to pin prick in the distribution of the proximal superficial of peroneal nerve. Sensory deep peroneal branch would be between first and second toe for which she never recovered. Motor recovery of ankle plantar flexion was first noted at 15 months and at 18 months achieved a strength of 4/5 and was a definitive sign of regeneration across the sural nerve/autologous hSC construct (https://youtu.be/D_CluQzh1C0) within the tibial nerve division of the sciatic nerve. At 24 months postrepair she recovered grades 1–2 movement of her ankle dorsiflexion/eversion consistent with peroneal division motor recovery. Her pain in the distribution of the sciatic nerve was maximal soon after injury and diminished over time where it was rated as 0/10 at the 15-month time point with occasional lancinating pain in the sciatic nerve distribution. MRI demonstrated scar tissue around the grafted region without and ultrasound revealed gadolinium and continuity of the sural nerve grafts with the sciatic nerve.
Discussion
The sciatic nerve is the largest nerve in the human body. The repair of this nerve, particularly when a significant gap exists, represents one of the most difficult challenges in nerve surgery. One of the major limiting factors in the repair is the absence or lack of donor nerve material. Even in cases in which a relatively small gap exists, the donor sural nerves, which are the typical nerves that are harvested for this repair, are rapidly depleted as the cross-sectional area is at least 15 times the width of the donor nerve 4 . Insufficient donor material reduces the chance of successful regeneration through a segmental peripheral nerve defect.
The sciatic nerve can be injured in a variety of different scenarios. High sciatic nerve injury often occurs iatrogenically as a result of intramuscular gluteal injections or as a complication of surgical repair of the hip joint, but it can also occur from compression, hip fracture/dislocation, or penetrating trauma 44 . At the midthigh the sciatic nerve can be injured as the result of a gunshot wound, knife, or boat propeller. Repair of sciatic transection with the use of nerve autograft has yielded variable success in the past in both civilian and military populations5,44–48. From these studies we see variable rates of success depending on the level of injury and whether the tibial or peroneal branches were involved. The worst outcomes are seen in the peroneal division of the sciatic nerve at the level of the buttock44,48. In contrast, somewhat higher rates of recovery are seen with tibial graft repairs in the midthigh. In addition to location of injury within the leg and branch involved, other factors cited to affect success of nerve grafting include length of time to surgery (>4 months) and a nerve defect or gap >5 cm; both are associated with worse outcomes 5 . In my (A.D.L.) clinical experience, much shorter traumatic gaps within the proximal sciatic nerve (n = 5; with 4-, 6-,-4-, 4-, and 5-cm gaps, respectively) repaired using traditional methods with sural nerve autograft only have not obtained similar clinical outcomes to the case described above.
The sural nerve is a common candidate for autologous nerve grafting as it represents a noncritical sensory nerve leaving a relatively small area of sensory deficit after harvest3,49. The sural is most commonly made up of medial and lateral components, which are branches from the tibial and common peroneal nerve, respectively 3 . Cadaveric studies have demonstrated a median sural length of 43 cm with a range of 35 to 47 cm49. We studied cadaveric specimens of sural and sciatic to obtain morphometric data on cross-sectional area (CSA), fascicular content, etc. We found an incredible amount of heterogeneity of the sural nerve CSA and fasicular content and estimated, using a 95% confidence interval, that patients with sural nerves exhibiting a small CSA may only be able to cover a 2.5-cm gap of sciatic nerve defect, whereas those with larger CSA may bridge up to an 8-cm gap 4 . Therefore, numerous sural nerve grafts must be cut, layered, and sutured across a human sciatic nerve gap to bridge a traumatic defect. Insufficient autologous nerve is a major obstacle to successful repair strategies for sciatic nerve injuries with large gaps.
Donor nerve for the preparation of autologous hSCs can be harvested either from a relatively small segment of sensory nerve (e.g., sural nerve) or from local debridement of injured nerve at the epicenter of the nerve injury in the cases of penetrating injury in which early exploration is performed to determine gap length and stabilize the nerve ends. In the current case we were able to demonstrate using growth curves and cell viability assays that either could serve as a source of hSCs. Sharp injuries, which include forces that bruise the nerve ends (e.g., propeller injury, gunshot wound, chain saw), cannot be repaired immediately as one allows the traumatized nerve ends to “mature,” permitting the surgeon to define normal fascicular anatomy some 3–4 weeks postinjury. This 3- to 4-week delay is a perfect opportunity to use the cell culture laboratory to enhance the quantity of donor SCs. Adding autologous SCs suspended in serum within a collagen tube significantly enhanced the gap distance that can be repaired after a long segmental nerve defect in the sciatic nerve of rats with no observed toxicity 30 . In fact, the addition of SCs within a guidance channel resulted in less autophagy when compared to reverse sciatic nerve autografts.
The primary goals for nerve repair are restoration of motor and sensory function. An area of nerve repair that is underemphasized is pain control. Our patient did not develop neuropathic pain after her injury. There is mounting evidence that entubulation strategies after nerve repair in animals30,50 and humans 51 can reduce pain. The mechanisms advanced for pain reduction with entubulation or wrapping include the prevention of neuroma formation by eliciting orderly and linear growth of axons. In experimental models, nerve autografts may demonstrate abundant regeneration, as measured by myelinated axon counts and larger axonal profiles but they also had the highest autotomy scores 30 . One possible explanation is that the guidance channel provides a scaffold for more directional growth and/or is less permissive for the growth of pain fibers compared with an autograft.
One other potential safety concern, in addition to pain, in the field of cellular autotransplantation for peripheral nerve repair is the need to rule out the possibility of creating tumors by transplanting cells expanded in cell culture with mitogens. While our published data demonstrating 39 that hSCs extensively expanded in cell culture do not form tumors when transplanted in immune-deficient rats and mice, the current report along with our eight current clinical patient cases of autologous hSCs for subacute and chronic thoracic SCI (unpublished observations) support the safety of SC use in an autotransplantation protocol.
The current patient was considered to be an ideal candidate for initial proof of concept for autologous hSCs for nerve repair, as repair techniques using standard nerve grafting described above are unable to restore sciatic nerve integrity and function in cases of long gap nerve defects. Future studies will attempt to improve the method of delivery of hSCs to the injured area. In summary, combining standard nerve grafting with autologous SCs within a collagen wrap (Duragen®) provides an opportunity to maximize nerve regeneration and restoration of function.
Footnotes
Acknowledgment
Dr. Allan D. Levi receives teaching honorarium from Medtronic.