
Abstract
Hepatocyte transplantation is an upcoming treatment for patients with metabolic liver diseases. Repeated cell infusions over 1–2 days improve clinical outcome. Isolated hepatocytes are usually cold stored in preservation solutions between repeated infusions. However, during cold storage isolated hepatocytes undergo cell death. We investigated if tissue preservation and repeated isolations are better than storage of isolated hepatocytes when cold preserving human hepatocytes. Liver tissue obtained from liver surgery or organ donors was divided into two pieces. Hepatocytes were isolated by collagenase digestion. Hepatocytes were analyzed directly after isolation (fresh) or after storage for 48 h at 4°C in University of Wisconsin solution (UW cells). Liver tissue from the same donor was stored at 4°C in UW and hepatocytes were isolated after 48 h (UW tissue cells). Hepatocyte viability and function was evaluated by trypan blue exclusion, plating efficiency, ammonia metabolism, CYP 1A1/2, 2C9, 3A7, and 3A4 activities, phase II conjugation, and apoptosis evaluation by TUNEL assay and caspase-3/7 activities. Hepatocytes stored in UW showed a significantly lower viability compared to fresh cells or hepatocytes isolated from tissue stored for 48 h (54% vs. 71% vs. 79%). Plating efficiency was significantly decreased for cells stored in UW (40%) compared to fresh and UW tissue cells (63% vs. 55%). No significant differences between UW cells and UW tissue cells could be shown for CYP activities or ammonia metabolism. Hepatocytes stored in UW showed a strong increase in TUNEL-positive cells, whereas TUNEL staining in cold-stored liver tissue and hepatocytes isolated after 48 h was unchanged. This observation was confirmed by increased caspase-3/7 activities in UW cells. Although preservation of isolated hepatocytes in UW maintains function, cold storage of liver tissue and repeated hepatocyte isolations is superior to cold storage of isolated hepatocytes in preserving hepatocyte viability and function.
Introduction
Hepatocyte transplantation is an evolving therapy for patients with inherited metabolic liver diseases that are characterized by deficiency of one particular enzyme or protein, giving rise to hepatic and/or extrahepatic disease. As the liver has a high redundancy in function, selective replacement of a fraction of the liver cell mass is clearly therapeutic, and replacement of the whole liver by orthotopic liver transplantation may not be required (15). It is assumed that replacement of 10–20% of the liver with healthy donor hepatocytes can correct a wide range of inherited metabolic liver diseases. However, only 5% of the liver mass can be infused at one transplantation event distributed over hours to days due to the risk of portal thrombosis (7). Thus, repeated transplantations are necessary to obtain adequate engraftment. As a result, hepatocytes are cold stored between repeated infusions (7,8,22). University of Wisconsin (UW) preservation solution is currently the gold standard for storage of isolated hepatocytes. However, this solution was originally developed for organ preservation and not for preservation of isolated cells. Several authors have shown that isolated hepatocytes can successfully be cold stored for more than 3 days without major loss of viability and function (12,17). Hepatocytes for clinical transplantation have been shipped between isolation center and transplantation site over long distances in UW solution (7). It is also well known that hepatocytes, after isolation, undergo programmed cell death due to loss of cell anchorage, a mechanism called anoikis (21). Furthermore, Abrahamse et al. showed that hypothermic storage in UW, histidine-tryptophan-ketoglutarate (HTK), or Celsior solution induces hepatocyte necrosis and DNA fragmentation after 24 and 48 h (1).
In the current study, we compared traditional cold storage of isolated hepatocytes in UW solution to storage of liver tissue with repeated hepatocyte isolations on hepatocyte viability and function.
Materials and Methods
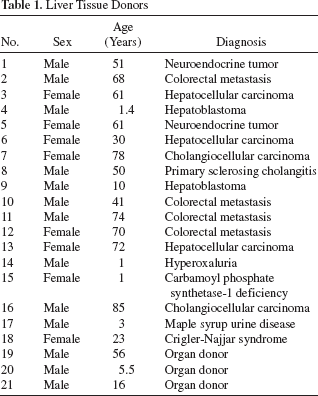
Human liver tissue was obtained with informed consent and approval by the Regional Ethics Board, Stockholm, Sweden (Dnr: 2010/678-31/3), and IRB protocol 0411142, University of Pittsburgh, PA, USA. Liver tissue was obtained from patients undergoing liver resection or liver transplantation due to metabolic liver diseases, or from deceased organ donors (Table 1). Hepatocytes were isolated from 21 different individuals (8 females, 13 males). Donor age ranged from 1 to 85 years.
Liver Tissue Donors
Directly after procurement, liver tissue was flushed with cold Eagle's Minimum Essential Medium (EMEM; Lonza, Allendale, NJ, USA) followed by cold UW (Viaspan; Bristol-Myers Squibb, New York, NY, USA). The liver tissue was dissected into two pieces (Fig. 1). From one piece, hepatocytes were isolated directly. Hepatocytes from this isolation were either analyzed immediately (fresh) or following storage in UW at 106 hepatocytes/ml for 48 h at 2–8°C (UW cells). Before analysis, UW cells were pelleted with low-speed centrifugation at 60 × g for 5 min at 4°C. Pellets were washed with ice-cold EMEM. The centrifugation/washing step was repeated three times. The second piece of liver tissue was stored in UW at 2–8°C and hepatocytes were isolated after 48 h of storage (UW tissue cells) (Fig. 1).

Schematic diagram of the experimental design. After procurement, liver tissue was divided into two pieces. From one piece, hepatocytes were directly isolated and either analyzed directly (fresh) or after 48-h cold storage in University of Wisconsin solution (UW cells). The second piece of liver tissue was cold stored in UW and hepatocytes were isolated after 48 h of storage (UW tissue cells).
Human Hepatocyte Isolation
Hepatocytes were isolated using a standardized three-step collagenase perfusion technique (11,25). In brief, one to three silicone catheters (Corning Life Sciences, Tewksbury, MA, USA) were sutured into major hepatic vessels on the cut surface of the tissue. To prevent efflux of perfusate, the remaining open vessels were closed with sutures (Vicryl 3/0, 4/0, or 5/0; Ethicon, San Angelo, TX, USA), and/or in some cases surgical tissue glue (Loctite; Henkel Corp., Westlake, OH, USA) was applied to the cut surface to close remaining leaks. Catheters were connected to a peristaltic pump and the liver specimen was placed in a sterile bag (Associated Bag Company, New Kingstown, PA, USA). Perfusion solutions and the liver specimen were kept in a water bath at 37°C. Flow rates ranged from 10 to 200 ml/min depending on the size of the tissue. The first perfusion solution consisted of Hanks' Balanced Salt Solution (HBSS; Lonza; without calcium, magnesium, and phenol red) supplemented with 0.5 mmol/L ethylene glycol tetraacetic acid (EGTA; Sigma-Aldrich, Stockholm, Sweden). The second solution consisted of HBSS without EGTA. Finally, the tissue was perfused with a third solution composed of EMEM supplemented with 250 mg/L collagenase type XI (Sigma-Aldrich) and 50 mg/L DNase (Sigma-Aldrich). The tissue was perfused with the third solution for 25–35 min during which time the solution was recirculated. Digested tissue was then mechanically disrupted in ice-cold EMEM. The resulting cell suspension was filtered through sterile gauze. Hepatocytes were pelleted by centrifugation at 70 × g for 5 min at 4°C. The centrifugation/ washing step was repeated three times. The final hepatocyte pellet was resuspended in Williams E medium (Lonza). Cell number and viability were assessed by standard trypan blue (Sigma-Aldrich) exclusion test. An aliquot of the final cell suspension was mixed with an equal volume of 0.4% (w/v) trypan blue in phosphate-buffered saline (PBS). The number of viable (unstained) and dead (blue) hepatocytes were counted in a hemacytometer (Marienfeld, Lauda-Königshofen, Germany). Hepatocyte viability is expressed as percentage of viable cells of the total cell number.
Plating Efficiency
Hepatocytes were resuspended in Williams E medium without phenol red supplemented with 5% bovine calf serum (Lonza), insulin (10–7 M; Novo Nordisk, Bagsvard, Denmark), dexamethasone (10–7 M; Sigma-Aldrich), and antibiotics-antimycotics (Lonza). Viable cells (7.5 × 105) were seeded in each well of a six-well culture plate (Corning) precoated with type I rat collagen (0.03 mg/ml concentration; in-house). Cells were cultured at 37°C in a humidified atmosphere of 5% CO2/95% air. Two hours after plating, medium from half the wells was exchanged with fresh medium without serum. After 10–18 h, these three wells were washed extensively to discard unattached hepatocytes and the remaining three wells were untouched. Cells were scraped and collected and the protein content of each well was determined with the Bio-Rad Protein Assay kit (Bio-Rad, Sundbyberg, Sweden; cat. No. 500-0006). Plating efficiency was defined as the ratio of protein content in washed wells to the protein content in unwashed wells and is expressed as a percentage.
Drug Metabolism Studies
Cytochrome P450 (CYP450) activities were measured immediately after washing while in suspension and then after 5 days of culture with treatment for the last 3 days with specific inducers: 25 μM β-naphthoflavone (BNF; Sigma-Aldrich) for CYP450 family 1 subfamily A polypeptide 1/2 (CYP 1A1/2), 10 μM rifampicin (rif; Sigma-Aldrich) or 1 μM phenobarbital (PB; Sigma-Aldrich) for CYP 3A4, or 0.1% dimethyl sulfoxide (DMSO; Sigma-Aldrich) as vehicle control with replenishment every 24 h as previously described (16). Methods to assess ammonia, 7-ethoxyresorufin metabolism, resorufin conjugation, media, and culture conditions were performed as previously described (11). Additional cell-based assays for specific CYPs (1A2, 2C9, 3A7, 3A4) were used according to the manufacturer's instructions with minor modification. Briefly, 3 × 104 hepatocytes were added to a 96-well white plate (Thermo Scientific, Waltham, MA, USA) and incubated for 30 min at 37°C with proluminogenic compounds for specific CYPs (CYP-Glo™, Promega Corporation, Madison, WI, USA). Each assay was performed in triplicates. The luminogenic product was detected with a luciferin detection reagent, and after incubation for 30 min at room temperature luminescence was read directly in a white plate in a luminometer (Synergy HT, BioTek Instruments, Winooski, VT, USA) with an integration time of 1 s per well. The luminescence produced is proportional to CYP activity. Results were expressed as luminescence counting units (LCU)/min and normalized to double-stranded DNA (dsDNA) content.
Double-Stranded DNA Quantification
Quant-iT™ PicoGreen® dsDNA kit was used according to the manufacturer's instructions (Molecular Probes, Invitrogen, Camarillo, CA, USA) to quantify dsDNA. Quant-iT™ PicoGreen® in tris-ethylenediaminetetraacetic acid (EDTA) (TE; home-made from Sigma-Aldrich products) buffer was added to 96 wells and the fluorescence intensity was read on a fluorescence spectrometer (Synergy HT) at an excitation wavelength of 485 nm and an emission wavelength of 520 nm. A fresh standard curve of lambda DNA was analyzed for each assay and results are expressed as micrograms per milliliter.
Terminal Deoxynucleotidyl Transferase dUTP Nick End Labeling (TUNEL) Staining
To detect apoptotic hepatocytes, ApopTag® Peroxidase In Situ Apoptosis Detection Kit (Millipore, Solna, Sweden) was used according to the manufacturer's instructions for both liver tissue sections and cytospinned hepatocytes. Liver tissue sections were deparaffinized and hydrated. Slides of isolated hepatocytes were prepared by fixing hepatocytes for 5 min in 4% buffered formaldehyde (Histolab, Göteborg, Sweden) and washed three times in PBS. Hepatocytes were attached to glass slides (Superfrost Plus, Menzel-Gläser, Braunschweig, Germany) with a cytospin centrifuge (Thermo Shandon, Astmoor, Cheshire, UK). Glass slides were stored at −20°C until further processing. Next, cytospin slides and liver tissue sections were treated with proteinase K (Thermo Scientific) and hydrogen peroxide (Sigma-Aldrich). Equilibration buffer was added before incubation with TdT enzyme at 37°C for 1 h. Stop/wash buffer was applied and slides were incubated with anti-digoxigenin conjugate for 30 min in a humidified chamber. After washing with PBS, slides were developed by incubating with 3,3′-diaminobenzidine (DAB; Vector Laboratories, Burlingame, CA, USA) for 10 min. The slides were then washed, counterstained with hematoxylin (Histolab), dehydrated, mounted, and examined under the microscope (Olympus, Shinjiuko, Tokyo). More than 1,000 hepatocytes per slide were counted. Results are expressed as percentage of TUNEL-positive hepatocytes of the total number of hepatocytes.
Caspase-3/7 Activity
Caspase-3 and caspase-7 were measured with a luminescent assay, Caspase-Glo® 3/7 (Promega Corporation), according to the manufacturer's instructions with some minor modifications. Briefly, 3 × 104 hepatocytes were seeded in three wells of a 96-well white plate and incubated at 37oC for 30 min. Subsequently, an equal volume of Caspase-Glo™ reagent was added to each well and mixed by gently tapping the plate. After 30 min of incubation at room temperature, luminescence was read directly from a white plate in a luminometer with an integration time of 1 s per well. Luminescence produced by the assay is proportional to the amount of caspase activity present in the cell sample. Results are expressed as LCU per minute and normalized to a million viable cells.
Statistical Analysis
Experiments were performed in triplicates. Results are expressed as mean ± standard error of the mean (SEM). Statistical analysis between two groups was carried out by paired t test. Analysis of variance (ANOVA) was used to determine statistical differences, and Tukey's multiple comparison test was performed comparing three groups. Values of p < 0.05 were considered significant. Data were analyzed by GraphPad Prism software version 5.01 (San Diego, CA, USA).
Results
Hepatocytes were isolated from 21 different hepatic tissues. Table 1 shows a summary of the demographics. The donors included 8 females and 13 males, and age ranged from 1 to 85 years. The majority of liver tissue was obtained from patients undergoing liver resection due to primary or secondary malignancy (n = 13); five liver tissues were obtained from explanted livers of patients undergoing liver transplantation and three livers were from deceased multiorgan donors.
After procurement, liver tissue was dissected into two pieces of similar size (Fig. 1). From one piece, hepatocytes were isolated and analyzed directly (fresh) or analyzed after 48 h of cold storage in UW (UW cells). A third group called “UW tissue cells” consisted of hepatocytes isolated from the second piece of liver tissue after 48 h of cold storage of the tissue in UW (Fig. 1)
Hepatocyte Viability
Freshly isolated hepatocytes showed a mean viability of 79 ± 2%. After 48 h of cold storage (UW cells), hepatocyte viability decreased significantly to 54 ± 4% (p < 0.001). In comparison, hepatocytes isolated after 48 h of cold storage from liver tissue of the same donor (UW tissue cells) displayed a significantly higher mean viability of 71 ± 3% compared to UW cells (p < 0.001) (Fig. 2A).

Human hepatocyte viability and plating efficiency. (A) Hepatocyte viability (B) and plating efficiency for freshly isolated hepatocytes, UW cells, and UW tissue cells. Bars show mean and standard error. (C) Phase contrast photographs of human hepatocytes cultured on collagen. Representative photographs for freshly isolated hepatocytes, UW cells, and UW tissue cells taken after 1 day in culture. Scale bar: 100 μm.
Plating Efficiency
The ability of hepatocytes to attach to a cell culture plate coated with extracellular matrix requires viable cells expressing functioning cell adhesion molecules (25). Plating efficiency is suggested to be a marker for engraftment ability and thus is an important quality to retain in hepatocyte transplantation (11). Plating efficiency significantly decreased after cold storage from 62 ± 6% in freshly isolated hepatocytes to 40 ± 6% in UW cells (p < 0.01). However, UW tissue cells showed a significantly higher plating efficiency (55 ± 5%; p < 0.05) without a significant difference from the fresh group (Fig. 2B).
Drug Metabolism Studies
CYP450 activity was evaluated for CYP 1A2, 2C9, 3A7, and 3A4. Fresh cells showed a significantly higher CYP 1A2, 2C9, and 3A4 activity compared to UW cells, whereas no significant difference could be seen when compared to UW tissue cells. UW tissue cells showed a tendency toward higher CYP 1A2 and CYP 2C9 activities compared to UW cells. CYP 3A7 is a member of the CYP3A family. CYP 3A7 is expressed at the highest levels in fetal liver and its expression gradually declines over the neonatal and pediatric life (13). As expected, hepatocytes obtained from patients ≤ 1 year of age showed higher CYP 3A7 activity compared to hepatocytes from older donors (Fig. 3D). After 5 days of culture, all groups showed a robust specific in vitro induction of CYP 1A1/2 and CYP 3A4 (Fig. 4A, B).

CYP450 activity of human hepatocytes. (A) CYP450 family 1 subfamily A polypeptide 1/2 (CYP 1A1/2) measured by luciferin-6-methyl ether (ME), (B) CYP 2C9 measured by luciferin-6×-chloroethyl ether (CEE), (C) CYP 3A4 by luciferin-isopropyl acetal (IPA), and (D) CYP 3A7 measured by luciferin-6-pentafluoro-benzyl ether (PFBE). Values are luminescence counting units per minute per microgram of DNA. Bars show mean and standard error.

CYP450 activity, phase II activity, and ammonia metabolism in long-term human hepatocyte cultures. In a subset of livers (n = 6), we measured specific (A) CYP 1A1/2 by ethoxyresorufin-O-deethylase (EROD), (B) CYP 3A4 activities after 72-h exposure to prototypical inducers [β-naphthoflavone (BNF) for 1A1/2, phenobarbital (PB), and rifampicin (Rif) for 3A4] and in total after 5 days in culture. (C) Resorufin conjugation as measurement for phase II activity and (D) ammonia metabolism were performed both with hepatocytes in suspension and with hepatocytes in culture. Bars show mean and standard error.
Resorufin conjugation was evaluated for both hepatocytes in suspension directly after isolation and for hepatocytes in culture attached to collagen-coated wells. Although no statistical difference could be observed within the three groups, UW cells displayed a lower capacity to conjugate resorufin compared to both fresh and UW tissue cells. However, this function was restored in long-term culture (Fig. 4C).
A comparable ammonia metabolism was observed in all groups, both in suspension directly after isolation and after 5 days of culture (Fig. 4D).
Analysis of Hepatocyte Apoptosis in Isolated Hepatocytes and Liver Tissue
TUNEL staining was performed on liver tissue directly after procurement (fresh) and after cold storage of liver tissue for 48 h in UW (UW tissue). No significant difference in the rate of TUNEL-positive hepatocytes between fresh and UW tissue could be seen (4.6 ± 1.3% vs. 6.3 ± 2.0%, p = 0.2) (Fig. 5A).

Apoptosis in liver tissue and isolated hepatocytes. (A) Terminal deoxynucleotidyl transferase dUTP nick end labeling (TUNEL) staining was performed on liver tissue obtained directly after procurement (Fresh) and after storage of liver tissue for 48 h in UW (UW tissue). (B) TUNEL staining and (C) caspase-3/7 activity was performed on hepatocytes directly after isolation (Fresh), after storage of isolated hepatocytes in UW (UW cells), and after repeated hepatocyte isolation (UW tissue cells). Bars represent mean and standard error. Scale bars: 50 μm.
In contrast, isolated cells showed an increased TUNEL staining after 48 h of cold storage in UW, whereas cells isolated following cold storage of the tissue did not show increased TUNEL staining compared to freshly isolated cells (12.0 ± 5.9% vs. 1.0 ± 0.3% and 1.3 ± 0.5%, respectively; p < 0.05 and p < 0.05) (Fig. 5B).
These results were further confirmed when measuring caspase-3 and caspase-7 activities. A significantly higher caspase activity was detected in UW cells compared to fresh and UW tissue cells (p < 0.05) (Fig. 5C).
Discussion
Hepatocyte transplantation is a promising therapy for patients with metabolic liver diseases. However, outcome is hampered by the limitation of cell dose that can be administered in one infusion due to the risk of portal hypertension and portal thrombosis (3). Accordingly, clinical protocols have implemented repeated infusions in order to increase engraftment rates and clinical outcome. The amount of hepatocytes given at one occasion is usually limited to 2 × 108/kg body weight. This cell dose is given in separate infusions of 1 × 108–10 × 108 hepatocytes over 30–60 min (5,7). During and after infusion, portal pressure and flow are monitored regularly and infusion is postponed or stopped if portal pressure or flow reaches critical levels. Initially, portal pressure decreases rapidly after infusion has been stopped. With increasing cell numbers infused, the time period needed to decrease portal pressure increases substantially. As a result, isolated hepatocytes have to be stored over hours and days until transplantation (7,23). Current research protocols include pretreatment of the recipient, for example, hepatic radiation or hepatic resection, further delaying the time from hepatocyte isolation to transplantation (8,19). During that time, isolated hepatocytes are cold preserved (2–8°C) until needed. However, it is well known that isolated hepatocytes undergo progressive damage and subsequent cell death during cold storage (1,9,18,21). Although hypothermia slows cell metabolism, the low temperature causes cell damage by increasing the intracellular chelatable iron pool and generating reactive oxygen species (20). Increased rates of hepatocyte apoptosis and necrosis have been reported during cold storage (17,27). Recently, Smets et al. described the mechanism called anoikis, a form of apoptosis due to lack of cell anchorage, induced already 15 min after hepatocyte isolation (21).
In this study, we investigated if hepatocyte quality could be better preserved by storing liver tissue rather than isolated cells and performing repeated isolations, avoiding the detrimental effect of cold storage and loss of cell anchorage. Our results show that hypothermic storage of liver tissue and repeated hepatocyte isolations yields hepatocytes of higher viability and function compared to hypothermic storage of isolated hepatocytes. Cells isolated after storage of tissue (UW tissue cells) showed a significantly higher viability and plating efficiency compared to cells stored in UW (71% vs. 54 %, 55% vs. 40%). Mean viability and mean plating efficiency are slightly lower than our experience with hepatocyte isolations for clinical transplantations (Ellis, E., unpublished data) (11). However, this can be explained by the fact that these are not transplant-grade livers but livers donated for research, and we did not exclude any liver donors but have included a number of livers from older donors and donors with high-grade steatosis. These two factors are associated with lower hepatocyte viability and yield. Thus, this should be taken into consideration when extrapolating to clinical-grade hepatocyte isolations. The results should be confirmed with clinical-grade livers from donors with lower age and less degree of steatosis. However, our results regarding hepatocyte viability and plating efficiency are well in line with other reports (2,4,14).
Hepatocyte isolation is performed by cannulating and perfusing the major hepatic vessels with a collagenase solution. Usually, portal vein and liver vein branches are used for perfusion. An important factor for the quality and yield of the isolation is that vessels covering the entire piece of liver tissue can be found. Dividing the liver into several tissue pieces may jeopardize the vascular tree, resulting in damage or loss of hepatic vessels needed for perfusion. Consequently, liver tissue cannot be adequately perfused, which often leads to a decrease in both hepatocyte viability and yield of viable hepatocytes per gram of liver tissue. Although we used liver tissue smaller than one liver segment weighing less than 40 g, good perfusions could be performed using smaller sized catheters. Hepatocyte yield ranged from 0.2 × 106 to 17 × 106 per gram of wet tissue and did not differ between freshly isolated and stored liver tissue (data not shown). In our experience, hepatocyte yield is usually higher from a single segment when compared to a whole lobe of a liver. Repeated hepatocyte isolations increase the cost of the procedure. However, as hepatocyte quality is significantly improved by storing liver tissue and performing repeated hepatocyte isolations, this factor outweighs the increased costs. As a result of this study, we have changed the policy in our clinical hepatocyte transplantation program and perform repeated hepatocyte isolations if splitting the tissue is possible and a prolonged hepatocyte suspension time can be expected.
Hepatocyte viability differed significantly between livers, resulting in rather large standard errors. However, this is not surprising, as liver donors differed in age ranging from 1 to 85 years, underlying diagnosis, neoadjuvant chemotherapy, and degree of steatosis. These are all factors known to affect hepatocyte quality (2,4,14). Despite the variation, significant differences could be shown for viability, plating efficiency, CYP activity, and apoptosis. The strength of this study is that liver tissue and hepatocytes from the same donor are compared. No significant difference could be shown for phase I and II activities and ammonia metabolism as analysis was only performed for six liver donors.
In this study, we chose UW as preservation solution, although several other commercially available preservation solutions, cell media, or salt solutions are available and have been used for cold storage of human hepatocytes. We chose UW as it is superior in preserving human hepatocytes compared to other organ preservation solutions and as it is used in our and most other clinical hepatocyte transplantation programs (1,8). Recently, Pless et al. showed significant improvements in the cold storage of hepatocytes (17). Human hepatocytes plated on collagen could be stored for up to 2 weeks with minimal loss of viability by using a modified HTK preservation solution with increased chloride and potassium content (pH 7.0). They also showed that adding iron chelators deferoxamine and LK614 to UW solution improved cold storage of collagen-coated human hepatocytes. In another study, the same group improved the cold storage of isolated rat hepatocytes using chloride-poor solutions with addition of iron chelators as well as glycine and l-alanine (18). Fisher et al. demonstrated that addition of adenosine to 5% dextrose lactated Ringer solution as a preservation solution improved hepatocyte viability and decreased hepatocyte apoptosis in hepatocytes from steatotic livers (6). The results of our and their studies are not comparable, as different methods, setups, and species of liver donors were used. Furthermore, these solutions are not approved for clinical organ transplantation. Nevertheless, it certainly would be interesting to test these modified solutions in our system in future studies.
Our study did not address cryopreservation as another possible way of storing isolated hepatocytes until transplantation. The major advantage of cryopreservation is that hepatocytes can be stored for longer time periods. Hepatocyte transplantation can be scheduled and more extensive quality testing can be performed. However, present cryopreservation protocols cause severe hepatocyte damage due to intracellular ice crystal formation and osmotic stress. Cryopreserved hepatocytes show impaired plating efficiency, CYP activity, and protein synthesis (10,24,26) significantly inferior compared to freshly isolated hepatocytes.
In summary, this study shows that although preservation of isolated hepatocytes in UW solution maintains hepatocyte function, cold storage of liver tissue and repeated hepatocyte isolations is often superior to cold storage of isolated hepatocytes in preserving hepatocyte viability and plating efficiency and decreases induction of apoptosis. As a result, we have changed the protocol in our clinical hepatocyte transplantation program. Depending on the size of the recipient, and thus the needed cell dose, we consider dividing the liver tissue if it is of adequate size and if adequate perfusion of the pieces is not hampered. Furthermore, the results of this study suggest that not only cold ischemia time of the liver graft but also “hepatocyte suspension time” is a significant factor for the outcome, which should be taken into account in clinical hepatocyte transplantation.
Footnotes
Acknowledgments
This study was supported by grants from the Research Strategy Committee, Karolinska Institutet, the Stockholm County Council (“Forskar ST”), and the regional agreement on medical training and clinical research (ALF) between Stockholm County Council and Karolinska Institutet. We thank Isabell Steger for excellent graphic design. The authors declare no conflict of interest.