
Abstract
The neurorestorative effect of the parenchymal transplantation of olfactory ensheathing cells (OECs) for cord trauma remains clinically controversial. The aim of this article is to study the long-term result of OECs for patients with complete chronic spinal cord injury (SCI). One hundred and eight patients suffered from complete chronic SCI were followed up successfully within the period of 3.47 ± 1.12 years after OEC therapy. They were divided into two groups based on the quality and quantity of their rehabilitative training: group A (n = 79) in sufficient rehabilitation (or active movement-target enhancement-neurorehabilitation therapy, AMTENT) and group B (n = 29) in insufficient rehabilitation. All patients were assessed by using the American Spinal Injury Association (ASIA) standard and the International Association of Neurorestoratology Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS). Thirty-one patients were evaluated by the tests of magnetic resonance imaging (MRI), electromyography (EMG), and paravertebral sensory evoked potential (PVSEP). We found the following. 1) According to ASIA and IANR-SCIFRS assessment for all 108 patients, averaged motor scores increased from 37.79 ± 18.45 to 41.25 ± 18.18 (p <0.01), light touch scores from 50.32 ± 24.71 to 55.90 ± 24.46 (p < 0.01), pin prick scores from 50.53 ± 24.92 to 54.53 ± 24.62 (p <0.01); IANR-SCIFRS scores increased from 19.32 ± 9.98 to 23.12 ± 10.30 (p <0.01). 2) The score changes in terms of motor, light touch, pin prick, and IANR-SCIFRS in group A were remarkably different (all p < 0.01). The score changes in group B were remarkably different in terms of motor (p < 0.05) and IANR-SCIFRS (p < 0.01), but not light touch or pin prick (p > 0.05). 3) Comparing group A with group B, the increased scores in terms of motor, light touch, and pin prick were remarkably different (all p < 0.01), but not IANR-SCIFRS (p > 0.05). 4) Fourteen of 108 patients (12.96%) became ASIA B from ASIA A; 18 of 108 (16.67%) became ASIA C from ASIA A. Nine of them (8.33%) improved their walk ability or made them rewalk by using a walker with or without assistance; 12 of 84 men (14.29%) improved their sex function. 5) MRI examinations were taken for 31 patients; there were no neoplasm, bleeding, swelling, cysts, neural tissue destruction or infection (abscess) or any other pathological changes in or around OEC transplant sites. 6) EMG examinations were done on 31 patients; 29 showed improvement and the remaining 2 had no change. PVSEP tests were performed in 31 patients; 28 showed improvements and the remaining 3 had no change. 7) No deterioration or complications were observed in our patients within the follow-up period. Our data suggest OEC therapy is safe and can improve neurological functions for patients with complete chronic SCI and ameliorate their quality of life; the AMTENT most likely plays a critical role in enhancing functional recovery after cell-based neurorestorotherapy.
Keywords
Introductions
Much important progress has been made in basic research for spinal cord injury (SCI) and diseases or damage of the central nervous system (CNS) during the past 30 years (1,5,8,9,16,20,23,24,26,29,31–37), especially the neurorestorative strategy of olfactory ensheathing cell (OEC) therapy, which has been shown to help neuroregeneration/sprouting, remyelination, neuroprotection, and functional recovery in SCI or other damage or diseases in numerous animal experimental studies (9,16,20,23,26,28–30,34,39,41). More recently, it was reported that OEC therapy has been clinically applied to treat the patients with chronic SCI and other diseases or damage in several clinical studies, the majority of patients showed partially functional recovery by the American Spinal Injury Association (ASIA) assessment standard (2) following OEC transplant (12,13,17–19,27,43). So far, however, the viewpoint is still widespread in the community of public medical physicians that the patients with complete chronic SCI cannot improve their neurological functions. Based on the previous short-term results and long-term safety reports of OEC therapy in patients with chronic SCI (6,7,12–15,17–19), this follow-up clinical study with a mean of over 3 years for a large sample with complete chronic SCI using ASIA assessment standard and the International Association of Neurorestoratology Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS, see Table 1) (22), magnetic resonance imaging (MRI), electromyography (EMG), and paravertebral sensory evoked potential (PVSEP) attempts to further elucidate the long-term safety and efficacy of OEC neurorestorotherapy.
International Association of Neurorestoratology Spinal Cord Injury Functional Rating Scale (IANR-SCIFRS)
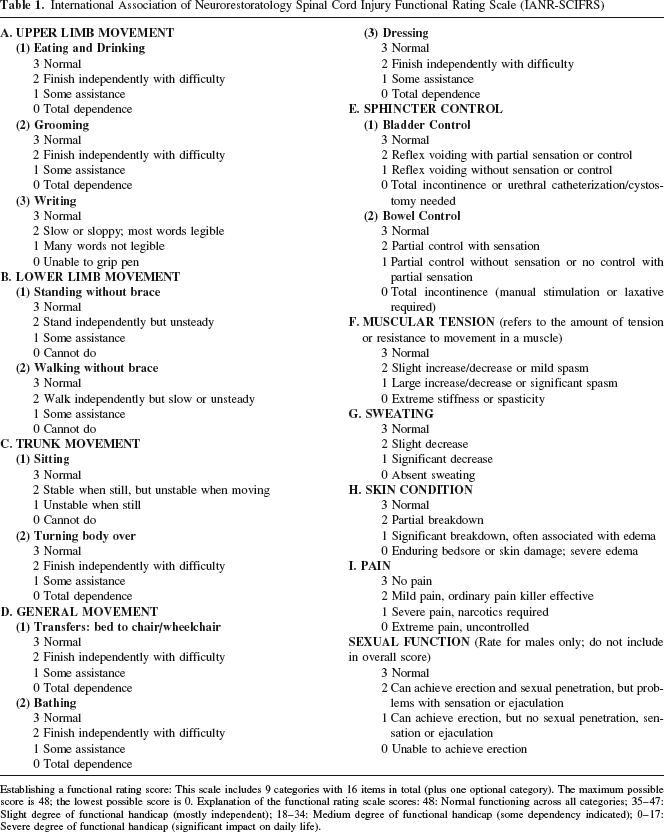
Establishing a functional rating score: This scale includes 9 categories with 16 items in total (plus one optional category). The maximum possible score is 48; the lowest possible score is 0. Explanation of the functional rating scale scores: 48: Normal functioning across all categories; 35–47: Slight degree of functional handicap (mostly independent); 18–34: Medium degree of functional handicap (some dependency indicated); 0–17: Severe degree of functional handicap (significant impact on daily life).
Materials and Methods
Subjects
One hundred and eight patients with complete chronic SCI were followed up successfully by physicians evaluating at our center and home visitations within the period of 1.0–5.3 (mean 3.47 ± 1.12) years after the OEC intraspinal cord transplantation, which has been described previously (13). Of them, 84 were men and 24 were women; their ages varied from 6 to 58 (average 34.29 ± 10.39) years; injury durations ranged from 0.5 to 30 (average 3.48 ± 4.73) years before OEC therapy. Lesion sites were located at the cervical segment (n = 51), thoracic segment (n = 42), or thoracolumbar junction (T12–L1) (n = 15), respectively.
The patients were divided into two groups according to the rehabilitation they performed: group A (n = 79) with sufficient rehabilitation (or active-movement target-enhancement neurorehabilitation therapy, AMTENT) and group B (n = 29) with insufficient rehabilitation. All patients were evaluated and reevaluated by the ASIA standards and the IANR-SCIFRS. Thirty-one patients returned to our center for follow-up and were reassessed by subsequent MRI, EMG, and PVSEP.
Statistical Analysis
The data are expressed as mean ± SD). Using SPSS 13.0 for Windows, paired samples t-tests were performed for the comparisons of the two states made prior to and after the OEC therapy in the two groups. Independent samples t-tests were carried out for the comparisons of increased scores between the two groups. A value of p < 0.05 was considered statistically significant difference.
Results
Functional Assessment
Results of all 108 patient scores between preoperation and follow-up by ASIA and IANR-SCIFRS assessment standard are shown in Table 2. The score changes by ASIA assessment were significant difference (motor, p < 0.01; light touch, p < 0.01; pin prick, p < 0.01). The score change by the IANR-SCIFRS assessment was significantly different (p < 0.01).
Comparison of all 108 Patients Scores Between Preoperation and Follow-up by American Spinal Injury Association (ASIA) and IANR-SCIFRS Assessment Standard (Paired Samples t-Test)

Results of patient scores in the two groups between preoperation and follow-up by ASIA and IANR-SCIFRS assessment standard are shown in Table 3. The score changes in group A by ASIA assessment were significantly different (motor, p < 0.01; light touch, p < 0.01; pin prick, p < 0.01). The score change by IANR-SCIFRS assessment was significantly different (p < 0.01). The score changes in group B by ASIA assessment were significantly different in motor (p < 0.05), but not in light touch (p > 0.5) and pin prick (p > 0.05). The score change by IANR-SCIFRS assessment was significantly different (p < 0.01).
Comparison of Patients Scores in the Two Groups Between Preoperation and Follow-up by ASIA and IANR-SCIFRS Assessment Standard (Paired Samples t-Test)

Table 4 shows the comparison of increasing scores of group A with group B using ASIA and IANR-SCIFRS assessment standard. Motor (p < 0.01), light touch (p < 0.01), and pin prick (p < 0.01) were significant, but IANR-SCIFRS assessment was not statistically different (p > 0.05).
Comparison of Patient Increasing Scores Between the Two Groups by ASIA and the IANR-SCIFRS Assessment Standard (Paired Samples t-Test)

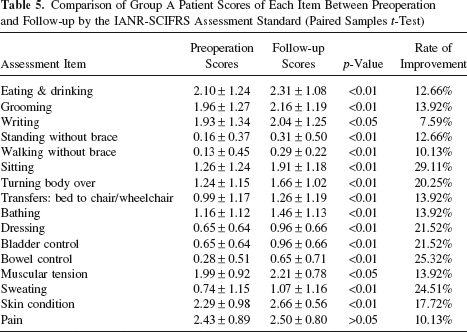
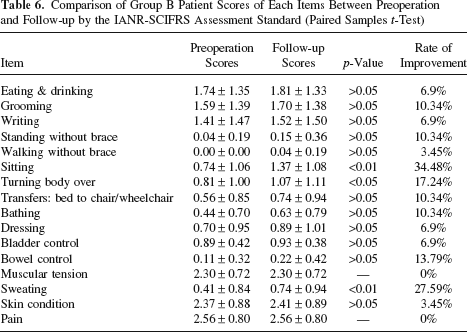
The scores of group A and group B by IANR-SCIFRS assessment standard between preoperation and follow-up are shown in Table 5 and Table 6.
Comparison of Group A Patient Scores of Each Item Between Preoperation and Follow-up by the IANR-SCIFRS Assessment Standard (Paired Samples t-Test)
Comparison of Group B Patient Scores of Each Items Between Preoperation and Follow-up by the IANR-SCIFRS Assessment Standard (Paired Samples t-Test)
Fourteen out of 108 patients (12.96%) became ASIA B from ASIA A; 18 of 108 (16.67%) became ASIA C from ASIA A. Nine of them (8.33%) improved their walk ability or were able to rewalk by using a walker with or without assistance; 12 of 84 men (14.29%) improved their sex function.
MRI, EMG, and PVSEP Test
Follow-up MRI scans were performed in 31 cases. Compared with preoperative MRI, the follow-up MRI showed no neoplasm, bleeding, swelling, cysts, neural tissue destruction or infection (abscesses), or any other pathological change in or around the OEC transplant area (Fig. 1). Follow-up EMG tests were taken in 31 cases. Compared to the preoperative EMG, 29 patients showed improvement and 2 had no change (Fig. 2). Follow-up PVSEP examinations were taken for 31 patients; 28 patients showed improvement and 3 had no change compared to the preoperative PVSEP (Fig. 3).

Comparison of the MRIs before (A) and 1.5 years after (B) olfactory ensheathing cell (OEC) therapy in one 18-year-old male patient with T12–L1 spinal cord injury shows no pathological findings.

Result of electromyography (EMG) test on Perone Long L muscle in the same patient as described in Figure 1 shows no motor unit potential (MUP) before the cell transplantation (A), but low amp MUP potentials at follow-up (B).

Findings of paravertebral sensory evoked potential (PVSEP) examination in the same patient as described in Figures 1 and 2 show stimulation location below S2 was not recorded (A), but the dermatome of S4 was recorded successfully at follow-up (B). Recordings at L3 (red in A, green in B), L5 (yellow in A, red in B), S2 (blue in A, yellow in B), and S4 (blue in B), respectively.
No deterioration or complications were found in any of the 108 patients within the follow-up duration.
Discussion
The results of this long-term clinical study show the benefits of OEC therapy for chronic complete spinal cord injury. Recently, rapid accumulating preclinical evidence has shown that neurorestoration of the central nervous system (CNS) is feasible (1,8,9,16,20,23,26, 29,32–36,42). The traditional conception in clinics, however, remains invariable in that the neurological dysfunction caused by neural degeneration or damage to the CNS cannot be restored, even partially (3). Since 2001, our series of clinical research and other studies (6,11) show that OEC transplantation appears to play a positive and exciting role towards changing this traditional viewpoint. The treatment results reveal a fact that the dream of neurorestoration for patients with neurodegeneration or lesions in the CNS can partially come true (6,7,10,11,14,15).
Possible Mechanism of OEC Therapy
The majority of research indicates that OECs may cause neuroprotection, axon remyelination, and axon regeneration or sprouting (9,16,20,23,26,29,34). Thus, it is easy to explain the mechanism of our long-term results by OEC therapy; but this cannot explain the rapid recovery of partial neurological functions observed in some patients soon after surgery. In fact, even in patients with complete chronic cord lesions where clinical functions are entirely lost, some of the axons or neurons are possibly alive but silent or with no functional expression, a state known as nerve hibernation; most of their spinal cord may still be anatomically continuous to various degrees. As we mentioned previously (17,18), we presume that the short-term positive results of OEC transplant are probably due to the unmasking of the quiescent axons or neurons, neuromodulation, or signal repair through the pivotal biochemical or growth factors produced and/or secreted by these cells and recover some lost functions.
Relationship Between Neurorestoration and Neurorehabilitation
OEC transplant and step training enhance hindlimb stepping ability in adult spinal transected rats (25). In clinical research, Constraint-Induced Movement therapy has also proved beneficial in improving the functions of disabled limbs (40). Single behavior therapy cannot cure the disability but it plays an important role in a patient's functional improvement. With the development of regeneration neuroscience, physical therapy will be a significant compensation to the recovery of neural deficits (4). Our results also demonstrate that patients with sufficient rehabilitation (or AMTENT) achieved more benefits after OEC therapy. Patients with insufficient rehabilitation after OEC therapy also had some functional restoration and improvement in their quality of life, but further analysis found a very interesting phenomenon. Some of their improvement in function had a close relationship to daily life, which included sitting and the ability to turn their body over. This means that no matter whether they do rehabilitation training or not, daily life activities are similar to some of the rehabilitation training exercises. Hence, all patients need to be encouraged to do AMTENT in order to obtain more neurological functional restoration and improve their quality of life following OEC therapy.
Relationship Between Neurological Functional Restoration and Quality of Life Improvement
The recovery of the ability to walk normally is usually considered as a major goal for SCI treatment. However, this aim for complete chronic SCI sufferers is not achievable in the present or the foreseeable future. Some of our patients' functions were good enough to be able to restand or rewalk by using a walker with or without assistance after OEC therapy with complementary AMTENT; so it is no longer a dream for these patients to restand or rewalk to some extent. Actually for all patients with complete chronic SCI, any motor functional recovery besides the ability to walk normally is greatly significant to their quality of life (21). In 2002, Raisman stated, “Currently, no forms of spinal injury can be repaired and understanding how to make nerve fibers regrow is, I would say, maybe a thousand years away.” He stresses that if transplant of OECs does result in patients regaining some function—bladder or bowel control, for example—this would be a major advance. “Even if we don't understand exactly how it is happening, this would possibly be the most significant advance in the history of neurology,” Raisman concluded (38). Therefore, even though there is really no motor function improvement, if nonmotor functions improve, such as muscular tension, sweat, rectum control, and bladder control, and pain relief such as our patients exhibited, this is a meaningful result nevertheless leading to an improvement in the patients' quality of life for complete chronic SCI sufferers.
Taken together, the data show that OEC transplantation is a safe alternative therapy, which has the capability of improving neurological functions for complete chronic spinal cord injured patients and ameliorating their quality of life; the AMTENT appears to enhance functional recovery strongly after cellular neurorestorotherapy. Future studies include further exploration of more effective comprehensive therapeutic strategies (second generation of regime), including neurorestorosurgery, combination transplantation of various cells, neurorestorative pharmacotherapy, neuromodulation stimulation therapy, physiotherapy, tissue engineering therapy, bioengineering therapy, Chinese traditional therapy, and so forth.
Footnotes
Acknowledgments
We thank Dr. Changman Zhou for his helpful discussions and revising, and Mr. John Heilman for his assistance with the English grammar revision. The authors declare no conflict of interest.