
Abstract
Neurorestoratology is a newborn and emerging distinct discipline in the neuroscience family. Its establishment will definitely speed up the advance of this promising frontier realm. A worldwide association for Neurorestoratology and several official journals covering this discipline have recently been set up. Clinical practice has demonstrated that the sequelae of damages and diseases of the CNS can be functionally restored to some degree. Obstacles that hinder the promising methods of Neurorestoratology to be translated from the bench to the bedside include political, governmental, religious, ethical, economic, and scientific factors or in most instances they work in combination. Falsehoods against the recognition of neurorestoratology include: 1) no therapeutic method is currently available that suggests that it is possible to repair, even partially, neurological functions; 2) according to the media, a cure will be very soon found for patients with severe spinal cord injury, brain trauma, and progressively deteriorated CNS degenerative diseases; 3) randomizing double blind control designed studies are the only gold standard for clinical study; self-comparison designed studies should be ignored and neglected. Future directions for neurorestoratology include the comparison and integration of current and upcoming available neurorestoration methods to look for the optimization regimes, and edit and publish clinical neurorestoratology treatment guidelines.
Introduction
Neurorestoratology is a newborn and emerging distinct discipline of the neuroscience family (5,20). It has been developing rapidly and has made great progress, especially in cell-based neurorestorative therapy from the lab to the clinic. However, there are still many obstacles for its development, such as falsehoods for its recognition. What is it really doing? How will it grow further? What is its main aim?
Achievements
Background and Process of Establishing Neurorestoratology
As depicted in Figure 1 (15), there are no truly effective interventions available for the treatment of many central nervous system (CNS) functional impairments and structural damages or their sequelae in the clinical practice of neurology, neurosurgery, neurorehabilitation, and all related disciplines.

Distribution of disease treated by clinical disciplines of neuroscience and relevant cross-disciplines.
We can see clearly that there is a question mark in Figure 1, which is similar to the original Dmitri Mendeleev periodic table where there were a number of blank boxes that remained to be filled with newly discovered elements later. Obviously, people all know that prolonging and improving a human's quality of life is the eternal desire, so it is inappropriate for physicians to always claim that there are no ways currently available to help patients with those disorders. The question is: Which discipline should replace the question mark in Figure 1?
Although several scientific terms related to neurorestoration have been forwarded, such as Restorative Neurology, Restorative Neurosurgery, Neurorestorative Surgery, and so on (15), all of them were considered as a branch of neurology or neurosurgery rather than an independent discipline.
These branches belong to various sections of clinical neurology or neurosurgery but they share similar interventions that include cell and/or tissue transplantation, neurostimulation and/or neuromodulation, bioengineering and/or tissue engineering and drugs. Given that each is not sufficient by itself to represent the whole neurorestoration field, the new term of Neurorestoratology was logically created, which fully reflects the context of neurorestoration and its name can be more easily recognized as a discipline in parallel with neurology, neurosurgery and neurorehabilitation as a member of the neuroscience family.
Therefore, establishing Neurorestoratology as a discipline is necessary for the rapid development of this advanced realm and we propose that Neurorestoratology deserves to replace the question mark in Figure 1.
As a matter of fact, neurorestoration is an integral part of many disciplines, as shown in Figure 2, and is the natural meeting point for all, but isolation in different disciplines had deprived them of a common platform for scientific exchanges until the independent discipline of Neurorestoratology was established. From then on, Neurorestoratology has successfully provided all neurorestoration basic scientists and clinicians with such a consolidated platform to effectively communicate with each other (Fig. 3). Meanwhile, they should keep working in the disciplines where they come from.
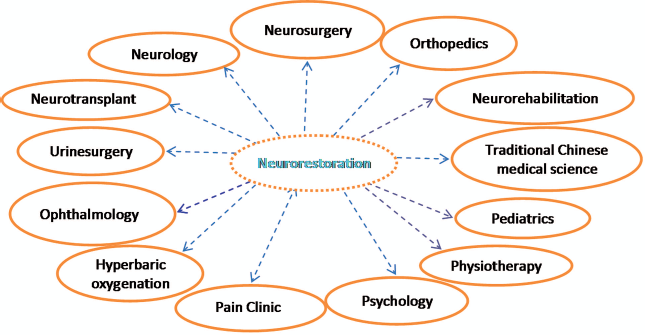
Neurorestoration is cross-point of all related disciplines.

Neurorestoratology plays a core platform and bridge for related disciplines with neurorestoration.
Main Achievements in the Renaissance of Neurorestoratology
Since an international scientific society, the International Association of Neurorestoratology (IANR), was established at Hong Kong in 2007 (http://www.ianr.org.cn/English/jianjie.asp?id=66,131), it has attracted members from over 40 countries and regions worldwide. Collaborating with other societies, the IANR publishes in three official journals: Cell Transplantation, Frontiers in Neurorestoratology, and American Journal of Neuroprotection and Neuroregeneration. The IANR has so far successfully held four annual conferences, especially the IANR IV and 8th GCNN combined conference at Amman of Jordan in 2011 after collaborating with the Global College of Neuroprotection and Neuroregeneration (GCNN) and American Society of Neural Therapy and Repair (ASNTR). So the IANR conference is becoming one of the best authority platforms for scientific exchange in Neurorestoratology. The textbook of Neurorestoratology is being edited by IANR members and will be published by American Scientific Publishing later this year.
The concept of Neurorestoratology was clearly defined by the Beijing Declaration of IANR, which was adopted at the 2nd IANR Annual Conference in 2009 (20). The draft of the declaration was endorsed by 32 leaders in Neurorestoratology from 18 countries and regions. Its innovative intervention strategies include cell or tissue transplantation, tissue engineering or bioengineering, neuromodulation by electromagnetic stimulation, pharmaceutical or chemical therapies. Its scope of study and treatment includes neurotrauma, neurodegeneration, cerebrovascular anoxia or ischemia, edema, demyelination, sensory and motor disorders, and neuropathic pain, as well as neural damage resulting from toxic, physical, and chemical factors, immune, infectious, inflammatory, hereditary, congenital, developmental, and other neural injuries (20).
To clearly make the study aim of Neurorestoratology; that is, to ensure that patients obtain increasing benefits through the enhancement of the translation between basic research and clinical application. Current cell-based combination therapeutic strategies in Neurorestoratology highlight the view of translational medicine (15) and the principle of the Declaration of Helsinki such as: “In the treatment of a patient, where proven prophylactic, diagnostic and therapeutic methods do not exist or have been ineffective, the physician, with informed consent from the patient, must be free to use unproven or new prophylactic, diagnostic and therapeutic measures, if in the physician's judgment it offers hope of saving life, re-establishing health or alleviating suffering. Where possible, these measures should be made the object of research, designed to evaluate their safety and efficacy. In all cases, new information should be recorded and, where appropriate, published” (http://www.wma.net/en/30publications/10policies/b3/index.html).
The clinical results of cell-based Neurorestoratology treatment definitely support the conclusion that sequelae of damages and diseases of the CNS can be functionally restored to a certain extent (3,15). The far-reaching significance of these achievements is that it begins to change the traditional clinical misperception that it is impossible to restore the damaged structures and functions of the CNS.
Clinical Cell-Based Therapy
Over 30 different types of cells have been studied in basic neurorestoration research, among them olfactory ensheathing cells (OECs), umbilical cord stromal cells, Schwann cells, neural stem/progenitor cells, and bone marrow stromal cells, etc., and they are starting to be tested in patients. Many publications have demonstrated that cellular therapeutic strategies of Neurorestoratology are safe and feasible in the treatment of human CNS lesions. Thousands of patients with CNS impairments have received varied cellular treatment and the majority of them successfully achieved a degree of neurological and functional recovery along with an improvement in the quality of life. The mechanisms of cell therapy include neuroregeneration and axon sprouting, neurogenesis and angiogenesis, neurorepair or remyelination, neural circuit or network reconstruction, neuroplasticity and neurosynapsis, neuroreplacement, neuroprotection by neurotrophins and immune or inflammatory modulation, neuromodulation or unmasking, and signaling repair by changing the microenvironment (15,22,26,27). Herein we briefly summarize some important achievements.
Spinal Cord Injury
Huang et al. in 2002, 2003, and 2009 (16,18,19) reported the transplantation of fetal OECs for patients with chronic spinal cord injury (SCI). The results showed that most patients improved their motor sensory and autonomic functions. Rabinovich et al. in 2003 (37), Mackay-Sim and colleagues in 2005 (12), and Lima et al. in 2006 (27) also implanted allogenic, autologous OECs, or olfactory mucosa respectively as clinical applications for spinal cord injury. The results of Rabinovich et al. and Lima et al. showed functional improvement; however, the results of Mackay-Sim et al. of three cases (30) showed that transplantation was safe but no functional improvement was observed, except in one out of the three patients whose level of sensation was increased. Actually, it is indeed hard to compare the results of different medical centers because of differences between cell culture, cell preparation, cell implant operation, etc. For example, Mackay-Sim's and colleagues' injection volume and cell amount was 150 μl/12 million, 300 μl/ 24 million, and 350 μl/28 million (80,000/μl) in the three participants (12). We wonder if the larger volume, especially 300 and 350 μl, might injure the spinal cord and depress the results of OEC transplantation. Many researchers (7,8,13,24,33–35,40,43,45) have reported on bone marrow stromal cell transplantation for patients with chronic SCI and most of the patients exhibited some degree of functional improvement. The California-based biopharmaceutical companies Geron and Stem Cells Inc. have received approval for Phase I clinical trials using embryonic stem cell-derived oligodendrocyte precursor cells and neural stem cells for the treatment of spinal cord injury in the US and Switzerland, respectively (29).
Multiple Sclerosis
Farge et al. (10) reported that autologous hematopoietic stem cell transplantation is capable of inducing sustained remissions for more than 5 years in patients with severe autoimmune diseases [primarily multiple sclerosis MS)], with similar results being shown in other studies (4,11,18,37,41,42). Although not a cure, the therapy may lead to prolong stabilization and change the aggressive course of MS.
Sequelae of Stroke
Bone marrow mesenchymal stromal (stem) cells (2, 25,39), neural stem/progenitor cells (23,38), or OECs (18,36) are some of the different cell types that have been transplanted for treating chronic stroke. All of the above-mentioned studies showed that the cells were safe and the majority demonstrated positive results. The UK stem cell company ReNeuron has received UK approval for a Phase I clinical trial of their immortalized neural stem cells in the treatment of stroke (29).
Amyotrophic Lateral Sclerosis
Currently most people still believe that there is no effective therapy that can stabilize or slow down the rate of clinical progression for amyotrophic lateral sclerosis (ALS). However, some recent studies showed that patients had benefited from various cell treatments including mesenchymal stem cells and olfactory ensheathing cells (9,17,18,30,31). The Maryland bio-therapeutics company NeuralStem has approval for a Phase I clinical trial using their neural stem cells for the treatment of ALS (29).
Cerebral Palsy and other Disorders
Accumulating evidence suggests that cell therapy such as OECs, neural stem/progenitor cells, and umbilical cord blood stem cells may also have a positive role to play in improving neurological function and the quality of life for patients with cerebral palsy, dementia, multiple system atrophy (MSA), ataxia, global brain ischemia, and Parkinson's disease (6,18,27,28,32). In 2010, Jozwiak et al. (21) and Yang et al. (44) also reported on the safe transplantation of umbilical cord blood-derived cells in patients with brain ischemic injury, MSA, and ataxia.
As to the technique of transplantation, cells can be transplanted into the parenchyma of the brain or spinal cord, the ventricle or subarachnoid space, or blood vessels (veins or arteries) (15). Even with different administration routes, research has shown varied degrees of functional improvement. Thus, it is reasonable to combine all these ways, and the principle of clinical cell therapy is most likely to be recommended as “MMMCs,” (i.e., multiple cells, multiple routes, multiple courses, and combined strategies). The development of optimized combination therapeutic strategies relies on the exploration of vast basic and clinical translation studies.
Obstacles
Even though cell-based therapeutic strategies in Neurorestoratology have been developing rapidly around the world, they have met and faced many obstacles in the past. These obstacles still do exist and will continue in the future. A great deal of promising neurorestorative methods often find difficulty translating from the bench to bedside. In the last 20 years, more than 1,000 basic research papers have been published that have demonstrated some degree of successful functional neurorestoration of CNS impairments in animal models, case studies, and small clinical trials. Simultaneously, thousands of review papers about these therapies that were forecasted to be promising in the clinic have been published, but most of the practical applications of these therapies existed only in these papers at that time. What are the obstacles that hinder the translation of neurorestorative medicine?
Politics, laws, or governmental regulatory rules, or a politician's viewpoint can greatly affect the developing direction of this field. The best example of this occurred in the US, where President Bush and the following President Obama have different opinions about cell therapy, especially embryonic stem cell research. Cell-based Neurorestoratology in the US could have a different fate between the two presidents. President Bush pushed laws and governmental rules to limit embryonic stem cell research, but President Obama is trying to readdress these limitations. Obviously the direction or developing speed of cell-based Neurorestoratology in the US has been influenced by such laws or governmental rules.
We understand that some religions reject the idea of allowing abortions. But no matter whether people are willing or not, abortion, or rather miscarriages, can spontaneously occur. The core issue is whether humans should use the aborted or miscarriaged tissue after it has already happened, especially when people know that the tissue could potentially help others to improve their function and improve their quality of life. Logically everyone's answer to the question of using the tissue once it becomes available should be “yes,” rather than burning or discarding the tissue regardless of their religious beliefs.
Ethics is very complicated issue. It is currently believed that new clinical trials or experimental treatments should not start until they have been approved by a scientific and ethical committee. While donating, people and patients should sign a consent document that informs them of all potential benefits and risks. These are the issues that should be truly paid attention to in view of ethics. Unfortunately, some people confuse political, lawful, or religious issues with ethical issues. The most extreme view is that someone rejects use of the aborted or miscarriaged tissue under an ethical pretense. Upon their viewpoint, they don't care whether the tissue is burned or thrown away, they are obstinate that it is ethically wrong to use the tissue, even if there is the potential to help restore other patients' functions or improve their quality of life. Is this viewpoint correct? Of course not. We should openly and strongly condemn this ethic viewpoint because it neglects living patients over discarded tissue. Some people don't know why they reject the use of the tissue, but just follow other people's opinion and really misunderstand what exactly they are rejecting. It puzzles us why tissue that is to be discarded or burned cannot be used. Whose ethic is it against if it is are used? Our opinion is that the inhuman ethic is to prefer burning or discarding tissue; the more human ethic is to use the tissue, rather than burning or throwing it away because it could potentially be used to save other people's lives or improve their quality of life. At that point in time the tissue is no longer viable as a human once an abortion or miscarriage has occurred.
Money is not everything, but without financial support, the study of cell-based Neurorestoratology cannot be carried out. Fortunately, now attention is being paid to Neurorestoratology and it is supported by the governments of developing countries and fast developing countries, charitable organizations, and personal donations.
Some scientists or physicians reject translation of some promising methods because they state that those methods are still immature. In fact, clinical practice is the only way to determine whether those methods are going to be effective or not for patients.
Falsehoods
Some people hold the following falsehoods for real-life Neurorestoratology. We summarize these below.
There are currently no known therapeutic methods to restore, even partially, neurological function (1). Conversely, patients who suffer severe spinal cord injury, traumatic brain injury, and progressive CNS degenerative disorders believe that they are going to be cured almost immediately because of exaggeration by some companies or the media that purposely overstate that stem cells can easily and very soon solve all problems. Meanwhile, the current level of achieved neurorestoration is believed to be too small and limited for them to necessarily undertake it. Patients with such devastating illnesses who always dream of a cure naturally tend to accept the higher expectation rather than the lower. These unrealistic hopes for a cure have driven people away from the real world and made them neglect functional recoveries that are already available with the current technologies of Neurorestoratology. Each specialist in this field knows that any progress may not be implemented easily but a little improvement is better than none, because small recoveries may be extremely important for patients' survival and health. So we should inform patients with CNS lesions and diseases to highly value practical neurorestoration that can be obtained today and, subsequently, hope to be improved tomorrow.
Paying too much attention to structural neuroregeneration or neuroreplacement. In fact, there are many alternative mechanisms for functional neurorestoration as listed above, especially signal modulation or plasticity, in which some of them may be mainly mechanisms of current achieved neurorestoration.
Randomizing double blind control studies is the only assessment method for top clinical study; self-comparison cannot be used as an assessment method for clinical study. Recently, however, Rama et al.'s clinical study with a self-comparison design was published (38). This marks the beginning of a new trend for clinical studies and its importance has been emphasized, especially in translational medicine. Self-comparison is sometimes a better option for some special clinical conditions. Its value is fully recognized and accepted for clinical studies of some incurable diseases, such as: heart, kidney, liver, and cornea transplant, and lesions that require surgical intervention (14). The place of sham-operation is questionable and ethical as it inflicts unnecessary harm on the controls.
Future Directions
The future progression of Neurorestoratology may embrace six different phases.
Phase 1: The concept changing period already finished, in which the aim is to explore if functional neurorestoration in CNS is achievable.
Phase 2: The therapeutic exploring period is in progress, in which the goal is to explore the therapeutic effect of various methods though clinical trials or experimental treatments.
Phase 3: The comparing and integrating period is ready to begin, in which the objective is to explore the more effective comprehensive therapeutic methods with evidence-based medicine.
Phase 4: The standardizing treatment period will hopefully not be too far into the future, in which the target is to establish and improve the clinical therapeutic guidelines.
Phase 5: The popularizing and raising period is likely to be a very long future process, in which the object is to extensively popularize it as a clinical routine treatment, continually studying the mechanisms, constantly increasing restorative methods, and continuously raise the effective degree of neurorestoration.
Phase 6: The clinical cure period may possibly come true in the far future, in which physicians will totally understand the nature of diseases and can manage them, make personal treatments, and make clinical cure.
We suggest that the following should be done now and in the near future.
Compare and integrate available neurorestoration methods to look for the optimizational regimes, and edit and publish clinical neurorestoratology treatment guidelines.
Combine Neurorestoratology with active movement-target enhancement neurorehabilitation to optimize functional recovery.
Push for more physicians, more medicinal centers, and more countries globally to promote neurorestorative treatments.
Rapid translation of the potential methods that have been demonstrated in basic research into clinical trials and application.
Actively explore the new advanced methods and their mechanism of action.
In conclusion, at this very early stage of Neurorestoratology, its development and maturity will rely on wisdom, patience, and strenuous efforts of neurorestorative scientists and clinical physicians who dedicate themselves to it.
Footnotes
Acknowledgments
We thank Dr. Dajue Wang for his advice on this manuscript. The authors declare no conflicts of interest.