
Abstract
During the past 15 years, our research group has transplanted fetal/neonatal cardiomyocytes, mesenchymal stem cells, and embryonic stem cell-derived cardiomyocytes into infarcted myocardium in a rat myocardial infarction model. Our experimental data demonstrated that cell transplantation therapy provides a potential approach for the treatment of injured myocardium after myocardial infarction based on the reported positive effects upon histological appearance and left ventricular function. However, the underlying mechanisms of the benefits from cell transplantation therapy remain unclear and may involve replacement of scar tissue by transplanted cells, induced neoangiogenesis and paracrine effects of factors released by the transplanted cells. In this review, we summarize our experiences from experimental cell transplantation therapy in a rat myocardial infarction model and discuss the controversies and questions that need to be addressed in future studies.
Keywords
Introduction
Myocardium that is irreversibly damaged by ischemia is replaced by a collagenous scar. Cell transplantation therapy aims to replace myocardial scar tissue with viable myocardial cells. Hypothetically, the transplanted cells might integrate into the host cardiac cells, simultaneously beating and contributing to improvement of regional and global myocardial function. While this was the initial rationale behind the concept of cell therapy, the reality is that mechanisms are much more complicated as discussed below. Various cell sources have been used for cell transplantation therapy of myocardial infarction in experimental and clinical studies (5,14,20). This review will summarize various hypotheses tested in our laboratory dealing with the overall concept of experimental cell transplantation therapy (Fig. 1). Some of this information was presented at the Sixth International Conference on Cell Therapy for Cardiovascular Disease held in New York City, NY, on January 20–21, 2011.

A schematic representation of experimental cell transplantation therapy for repairing damaged myocardium in a rat myocardial infarction model in our laboratory.
Hypothesis 1. Transplanted Cells Can Survive and Form Sizable Grafts Within Infarcted Myocardial Tissue
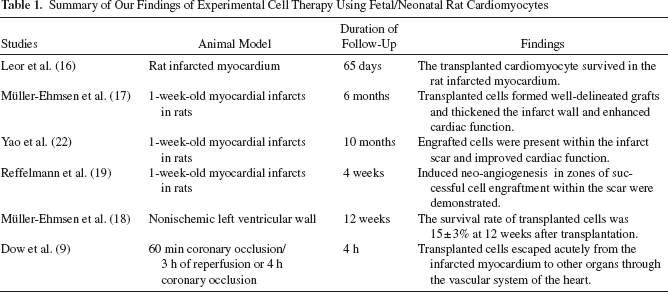
In 1996, Leor et al. (16) reported that transplanted fetal cardiomyocyte tissues, which were harvested from human fetal hearts (7–12 weeks of gestation) and fetal rat ventricles (14-day embryos), were able to survive in the infarcted rat myocardium (7- to 24-day-old myocardial infarctions) for 65 days after transplantation. In a long-term study, Müller-Ehmsen et al. (17) injected male neonatal cardiomyocytes (isolated from hearts of 1- to 2-day-old rats) into 1-week-old myocardial infarcts of adult syngeneic female Fischer 344 rats. At 6 months after cell transplantation, the implanted male neonatal cardiomyocytes were detected by TaqMan polymerase chain reaction (PCR) of the male-specific Sry gene and histology. Cardiac cell transplantation thickened the left ventricular (LV) infarct wall and enhanced ejection fraction (assessed by left ventriculography) and reduced paradoxical systolic bulging of the infarct wall. Well-delineated grafts of muscle could be identified within the infarct zone. Yao et al. (22) implanted male fetal cardiac cells into 1-week-old myocardial infarcts in adult female Fischer rats. Ten months later, PCR analysis of the Sry gene of the Y chromosome and histological analysis showed that engrafted cells were present within the infarct scar. Fetal cardiac cell transplantation was demonstrated to increase infarct wall thickness, reduce LV dilatation, and improve LV ejection fraction over the course of 10 months.
Hypothesis 2. Improvement of Cardiac Function by Engrafted Cells May Be Due to the Induced Neoangiogenesis
The histological changes of implanted fetal cardiac cells within myocardial scar tissue were characterized. Etzion et al. (11) isolated fetal cardiac cells from 14- to 15-day-old rat embryos and labeled these cells with bromodeoxyuridine (BrdU) or the reporter gene LacZ. The fetal cardiac cells were injected into 1-week-old myocardial infarctions in female Sprague–Dawley rats. At 1, 4, and 8 weeks after transplantation, the engrafted cells were identified by X-gal staining, BrdU, and α-smooth muscle actin immunohistochemistry. Immunohistochemistry staining with primary antibodies against α-smooth muscle actin, connexin-43, fast and slow myosin heavy chain demonstrated that the engrafted cells were isolated from the host myocardium by scar tissue and kept their embryonic phenotype, did not differentiate into an adult phenotype at 2 months after transplantation. Whittaker et al. (21) injected male neonatal cardiac cells into normal and infarcted hearts in adult female rats. The hearts were examined at 0–1 days and 1–2, 4–6, and 12 weeks after transplantation in noninfarcted myocardium and 6 months later in the infarcted myocardium. Histological analysis showed that the transplanted cells had a rounded appearance and were disorganized and separated from the host muscle, although their nuclei increased in size. At 6 months after transplantation, the transplant cells' retardation of polarized light gradually increased to 81% of that of host cells and the collagen content in the transplant was 210–430% higher than in host myocardial tissue. Although transplanted cells were observed, improved function of the hearts described by these techniques may not be solely due to replacement of muscle—since the muscle was not entirely differentiated adult phenotypic cardiomyocytes. One other mechanism may be related to angiogenesis described below.
Transplantation of neonatal cardiomyocytes may induce neoangiogenesis in recipient hearts. Reffelmann et al. (19) induced myocardial infarction by left coronary artery ligation in rats. One week later, neonatal rat cardiomyocytes were intramyocardially injected into the scar area. At 4 weeks after transplantation, regional myocardial blood flow was evaluated by radioactive microspheres, and angiogenesis was examined by histology. Intramyocardial injection of cultured neonatal cardiomyocytes significantly improved regional myocardial blood flow and resulted in a high capillary density within clusters of engrafted cells in the scar area. This therapy also thickened the infarcted ventricular wall and lowered infarct expansion indices. Left ventriculography demonstrated that cell therapy improved cardiac function characterized by smaller diastolic and systolic left ventricular volumes. These data suggested that transplantation of neonatal cardiomyocytes enhanced myocardial tissue perfusion by neoangiogenesis in zones of successful cell engraftment within the scar.
Hypothesis 3. The Washout of the Transplanted Cells may Contribute to the Low Cell Survival Rates within Host Myocardium
Retention and long-term survival of transplanted cells is limited within host myocardium. Mμller-Ehmsen et al. (18) isolated male donor cardiomyocytes from neonatal Fischer 344 rats (1–2 days) and injected them into the nonischemic left ventricular wall of female syngeneic adult rats. Transplanted cell survival rates were assessed by quantitative real-time TaqMan PCR of the male-specific Sry gene. The survival rate of transplanted cells was 57 ± 9% at 0–1 h, 24 ± 6% at 24 h, 28 ± 11% at 7 days, 27 ± 3% at 14 days, 23 ± 8% at 4 weeks, and 15 ± 3% at 12 weeks after transplantation. The cell loss may not be due to apoptosis because caspase inhibitor AcYVADcmk did not improve transplanted cell survival at 24 h. Histology showed transplanted cells and their nuclei were smaller than those of host myocardium at 12 weeks after transplantation, although these cells became more elongated, developed cross-striations and bigger nuclei over time. The washout of the transplanted cells from the cardiac vasculature may play an important role in cell loss. Dow et al. (9) subjected female Fischer rats to 60 min of left coronary artery occlusion followed by 3 h of reperfusion (reperfusion group) or 4 h of permanent left coronary artery occlusion (nonreperfusion group). At either 15 min postreperfusion in the reperfusion group or 75 min after occlusion in the nonreperfusion group, male neonatal rat cardiac cells were injected directly into the left ventricular free wall. The transplanted cells were detected by PCR of the Sry gene and histology at the end of the protocol. Histology showed that round, immature cardiomyocytes appeared within the cardiac venules. Transplanted cardiomyocytes were found in 6.57 ± 1.33% fields in the nonreperfusion group, but only in 3.39 ± 0.69% fields in the reperfusion group, and the difference was significant (p < 0.05). PCR analysis found transplanted cells in the hearts and lungs of 100% of the rats (5 of 5) in both groups, in the liver and kidneys of 40% of the reperfusion group and 60% of the nonreperfusion group, and in the spleen of 40% of the nonreperfusion group. The results demonstrated that transplanted cells escaped acutely from the infarcted myocardium to other organs through the vascular system of the heart; reperfusion might promote the cell washout.
Hypothesis 4. Transplanted Bone Marrow-Derived Mesenchymal Stem Cells May Transiently Improve Cardiac Function Through an Early Paracrine Effect
Mesenchymal stem cells (MSCs) have been considered potential cell sources for cardiac cell therapy (for review, see refs. 7,15). Dai et al. (6) injected MSCs, which were isolated from the femoral and tibial bones of donor ACI rats and labeled with DiI, into 1-week-old myocardial infarctions in female Fischer CDF rats. Histological examination showed that DiI-positive cells were observed at 2 weeks and at 3 and 6 months. At 2 weeks after transplantation, DiI-positive cells did not express muscle-specific markers α-actinin, myosin heavy chain, phospholamban, and tropomyosin. However, at 3 and 6 months after transplantation, the above muscle-specific markers did express in DiI-positive cells; but these DiI-positive cells did not fully evolve into an adult cardiac phenotype. Endothelial cell marker von Willebrand factor was expressed in some of the DiI-positive cells. LV ventriculography showed that MSC therapy improved global LV function at 4 weeks; however, these benefits of MSC treatment were lost at 6 months. The results suggest that MSC treatment improves cardiac function perhaps by an early paracrine effect. In another study, Dai et al. (4) cultured MSCs in fresh medium. Four days later, cultured medium containing soluble factors secreted by cultured MSCs was collected. Fischer rats were subjected to left coronary ligation. One week later, the rats received saline, fresh medium, cultured medium, or 2 million MSCs in fresh medium by direct intramyocardial injection. At 4 weeks after treatment, left ventriculography showed that LV ejection fraction was better in the fresh medium, cultured medium, and MSC groups than in the saline group. Heart rate, blood pressure, postmortem LV volume, infarct size, or septum thickness were comparable among the groups; only MSCs significantly increased wall thickness compared to the other three groups. The roles of the soluble factors released by MSCs in the cultured medium might be masked, because the fresh culture medium contains nutrients and bovine serum. Therefore, the paracrine effects of transplanted MSCs need further investigation.
Hypothesis 5. Delivery Vehicle and Routing May Influence the Distribution of Transplanted Cells
Injectable biomaterials can be used as delivery vehicle for cell transplantation to increase the transplanted cell retention and survival. Dai et al. (3) mixed bone marrow-derived rat MSCs (labeled with isotopic colloidal nanoparticles containing europium) with collagen matrix and injected this mixture into a 1-week-old myocardial infarction in rats. Four weeks later, tissues from the infarcted myocardium, noninfarcted myocardium, lung, liver, spleen, and kidney were sampled. Labeled cells (expressed as cell number/g tissue weight) were quantitatively analyzed by measuring the nanoparticle radioactivity in these tissues. Compared to saline as delivery vehicle, collagen matrix as a delivery vehicle significantly reduced the relocation of transplanted MSCs to remote organs and noninfarcted myocardium.
Transplanted cells can be delivered to infarcted myocardium by injecting them directly into the cardiac muscle or by the systemic vasculature system with the idea that the stem cells can home to injured myocardium. In a rat myocardial infarction model with 45 min of left coronary artery occlusion followed by 7 days of reperfusion, Hale et al. (12) directly injected MSCs (labeled with europium) into the ischemic region of the heart or intravenously injected MSCs before coronary artery reperfusion. One week later, tissues were sampled from heart, liver, spleen, and lung and engrafted labeled MSCs were quantitatively analyzed by measuring the nanoparticle radioactivity. Fifteen percent of transplanted cells were retained in the hearts receiving cells by direct intramyocardial injection, while no MSCs were detected in the hearts receiving cells by intravenous administration. The distribution of transplanted MSCs in liver, spleen, and lung were not affected by the route of administration. The results demonstrate that only a small proportion of the transplanted cells are retained in the heart with direct intramyocardial injection, and in this study transplanted cells did not “home” to the damaged heart with intravenous injection.
Hypothesis 6. Human Embryonic Stem Cell-Derived Cardiomyocytes Are a Promising Cell Source for Cardiac Repair
Although our experimental fetal/neonatal cardiac cell transplantation studies showed that this approach is promising for repairing of damaged myocardium and improving cardiac function after acute myocardial infarction, its clinical use is limited due to the difficulties of large-scale availability of human fetal/neonatal cardiac cells, as well as the concern that allogenic cardiomyocytes transplantation can cause an immunorejection in recipient hearts. Cultured human embryonic stem cells are capable of self-renewal in an unlimited fashion and can differentiate into cardiomyocytes with the structural and functional properties of early-stage cardiomyocyte. Human embryonic stem cell-derived cardiomyocytes (hESC-CMs) can be produced in large scale and may serve as an ideal cell source for cell transplantation therapy (8). Dai et al. (2) injected green fluorescent protein (GFP)-expressing hESC-CMs into the left ventricular wall subjected to ischemia/ reperfusion (15 min of left coronary artery occlusion followed by reperfusion) in athymic nude rats and immune competent Sprague–Dawley rats. hESC-CMs were injected directly into the myocardium within the ischemic risk area 5 min after left coronary artery occlusion. At 4 weeks after transplantation, engrafted hESC-CMs formed sizable grafts within the host nude rat hearts. The engrafted cells demonstrated both GFP epifluorescence and positive staining (co-localized) muscle marker α-actinin and exhibited cross striations (sarcomeres). These cells were well interspersed with the endogenous myocardium shown by connexin 43 positive staining. hESC-CMs did not induce immunorejection in nude rats as determined by inspection for lymphocytic infiltrate and/or giant cells; however, evidence of rejection was observed in immune competent Sprague–Dawley rats demonstrated by an overt lymphocytic infiltrate. In a preliminary report from our group with Mary Kearns-Jonker, we injected hESC-CMs into the myocardial infarct area at 1 week after infarction induced by permanent coronary occlusion in nude rats and observed that hESC-CMs improved cardiac function at 4 weeks after cell transplantation therapy (13).
Hypothesis 7. Cardiac Fibroblasts Can Be Reprogrammed and Used for Cell Transplantation
Reprogramming cardiac fibroblasts to prompt myogenesis provides a potential source of autologous myogenic cells for transplantation therapy. Etzion et al. (10) isolated rat fibroblasts from 7-day-old infarcted myocardium or normal pericardium. Cultured cardiac fibroblasts were transfected by an E1/E3-deleted adenoviral vector carrying both a human myogenic differentiation (MyoD) cDNA driven by a cytomegalovirus (CMV) promoter and a GFP reporter gene driven by a second CMV promoter. Cultured fibroblasts expressed muscle-specific MyoD family of transcription factors and underwent myogenic conversion. These cells appeared elongated and fused into multinucleated myotubes. Typical cross striation was identified by electron microscopy, and these cells were positive for sarcomeric actin, fast myosin heavy chain (fast-MHC), and actinin immunostaining. The myogenic cells were injected into 1-week-old rat infarcted myocardium. One month later, the transplanted converted fibroblasts formed a cluster of myogenic cells with positive immunostaining for the myogenic proteins fast-MHC and sarcomeric actin. The gap junction protein connexin 43 was expressed in a disorganized manner in a few transplanted cells. The results suggest that activating myogenesis of cardiac fibroblasts by MyoD in vitro could create a vast source of autologous myogenic cells for cardiac repair.
Summary
Our experimental studies in a rat myocardial infarction model demonstrated that cell transplantation therapy is a promising treatment after myocardial infarction based on the reported positive effects upon histological appearance, as well as a modest increase in left ventricular function (summarized in Tables 1–3), which is consistent with the findings reported in a recent large meta-analysis of bone marrow cell therapy for myocardial infarction (1). Cell therapy increased the thickness of the infarct wall, improved left ventricular stroke volume, decreased LV end-systolic volume, increased LV ejection fraction, and induced neoangiogenesis. Cell therapy did replace infarcted myocardium to some extent but did not always replace it with fully mature normal looking cardiomyocytes. The clinical application of cell therapy still faces many challenges and unanswered questions. For example, what is the best way to increase retention and long-term survival of engrafted cells? How should we induce the engrafted cells to truly differentiate into mature adult cardiac cells, become well interspersed with host cardiac cells, and simultaneously contract with host myocardium? What kind and how many cells should be injected? What is the optional route of delivery? When should the cells be transplanted after myocardial infarction? What kind of patient is best suited for cell therapy? To answer these questions, further basic, preclinical translational, and clinical translational investigations are needed.
Summary of Our Findings of Experimental Cell Therapy Using Fetal/Neonatal Rat Cardiomyocytes
Summary of Our Findings of Experimental Cell Therapy Using Mesenchymal Stem Cells (MSCs)

Summary of Our Findings of Experimental Cell Therapy Using Human Embryonic Stem Cell-Derived Cardiomyocytes (hESC-CMs)

Footnotes
Acknowledgments
This study was supported in part by the Los Angeles Thoracic and Cardiovascular Foundation and various grants from the NHLBI. The authors declare no conflict of interest.