
Abstract
Conflicting results have been reported on the effectiveness of the two-layer method (TLM) compared with the University of Wisconsin (UW) method for preserving pancreata. The objective of this study was to compile the evidence for or against any difference in human islet yield and viability between these two. PubMed (January 2000 to May 2008) and Cochran Library searches were performed and 17 studies were included for the meta-analysis. Data on donor characteristics, preservation time, and outcomes were abstracted. Studies were subgrouped based on how TLM was used (UW + TLM or TLM alone), on mean cold ischemic time (CIT) (>20 h or <20 h), and on whether special chemical was used (yes or no). Meta-analysis of all studies and subgroups was performed and the pooled standardized mean differences (SMD) with 95% confidence intervals (CI) were reported. Overall, the use of TLM significantly increased islet yield [SMD, 0.74 (0.44–1.04)] and viability [SMD, 0.63 (0.14–1.12)]. The beneficial effects of TLM on islet yield were more evident when TLM was used following UW storage or when prolonged CIT was used. TLM used alone, shorter CIT, and no chemical use all resulted in similar islet viability between TLM and UW groups. Beneficial effects of TLM on islet viability were demonstrated only when TLM was used following UW storage, or with prolonged CIT, or with chemical use. In conclusion, the TLM was beneficial for prolonged pancreas preservation before human islet isolation; however, benefit of the TLM for short-term preservation was not clear.
Introduction
Islet transplantation has become a promising treatment for type 1 diabetic patients but still faces challenges (3). As with any transplant program, a limiting factor is the availability of eligible donor graft. This is particularly limiting in the case of islet transplantation because of strict donor selection criteria and the requirement for short cold ischemic time (CIT) (21). During organ removal blood supply and hence oxygen is interrupted. The graft experiences a progressive deterioration of cellular function over time. Prolonged cold storage before islet isolation significantly reduces recovery of viable islets (9). Multiple donors are often required for one recipient to achieve insulin independence. Therefore, the development of a preservation solution to prevent graft injury during static cold storage is a critical step toward a viable islet transplantation program. The two-layer method (TLM) was developed to address this need. TLM consists of the UW solution and oxygenated perfluorodecalin (PFD), known for its high oxygen solubility coefficient (11). Because PFD is hydrophobic and has a high density, the two solutions are clearly separated, allowing for the pancreas graft to float in between. As a result, the graft gets oxygenated by the oxygen-laden PFD and at the same time, the nutrient supply comes from the UW (11). There is direct evidence from the canine pancreas transplant model to show that ischemically damaged pancreata can be successfully resuscitated by TLM (5,8).
Recently, a number of studies on human pancreata also reported the beneficial effect of TLM on islet isolation outcomes (6,11–15,17,18,20,23–27). However, many of these studies have small sample sizes that limit the validity of the conclusion. In addition, two recent large-scale studies showed no beneficial effect of TLM compared with UW storage in islet transplantation (4,7). The conflicting results have motivated us to plan for the meta-analysis to compile the evidence for or against any difference in islet yield and viability between the two methods. Interestingly, two articles on the same topic were published after we finished the literature search (May 2008), including a meta-analysis by Agrawal's group (1) and a review article by Noguchi's group (16). Results were discussed in the light of those two articles.
Materials and Methods
Selection of Studies and Data Extraction
The guidelines by Stroup et al. (22) for the meta-analysis of observational studies were followed in the design and reporting of this meta-analysis. Electronic searches of the NCBI PubMed and Cochrane Library and manual searches of review references were performed to find all pertinent literature. The search was set up using these key words: human islet isolation, human pancreas preservation, islet transplantation, UW, University of Wisconsin solution, TLM, two-layer method. The search was limited to human studies published in English since the year 2000 and it was supplemented by a manual search of the reference lists of review articles.
Titles and abstracts identified in the literature search were assessed for potentially eligible studies. To be included in the review, the study must have met the inclusion criteria: 1) published in English from January 2000 to May 2008, 2) comparing either islet yield or viability or both from pancreata stored in UW alone with those stored in TLM either directly or following a period of time in UW, 3) islet yield should be reported in the unit of IE/g (islet equivalent per gram) instead of IE, 4) the TLM solution consisted of UW and perfluorodecalin (PFD), 5) the organ donors could be clinical grade, research grade, or marginal. Duplicate reports for the same cohort of subjects or studies that were published only as abstracts were excluded.
The data extracted included: year of publication, study design, donor condition, islet isolation method, sample size, donor pancreas characteristics [age, gender, body mass index (BMI), pancreas weight, and CIT], and outcomes (islet yield and viability). The data were reviewed three times by Huanying Qin to minimize errors. An effort was made to contact authors for missing information and such information was included in the analyses.
Statistical Methods
Student's t-tests were performed to assess the differences between the two groups (TLM and UW) in key study features including donor and organ characteristics. Cochran Q statistics was used to evaluate heterogeneity between the studies. Cochran Q test is computed by summing the squared deviations of each study's effect estimate from the overall effect estimate, weighting the contribution of each study by its inverse variance. The Q statistic follows a chi-square distribution with k – 1 degrees of freedom, with k being the number of studies. Not rejecting the homogeneity hypothesis usually leads the meta-analyst to adopt a fixed-effects model because it is assumed that the estimated effect sizes only differ by sampling error. In contrast, rejecting the homogeneity assumption can lead to applying a random-effects model that includes both within- and between-studies variability (10). For each primary study, standardized mean difference (SMD) was calculated. SMD is defined as the mean difference between TLM and UW groups divided by the standard deviation of the difference. The pooled SMD was computed by summing the SMD of each study, weighting the contribution of each study by its inverse variance (10). Random effects model results were reported. Subgrouping analyses were performed based on study variations.
Results were considered significant for a value of p < 0.05. SAS 9.1.3 (SAS Institute, Cary, NC) was used for the statistical analysis. Meta-analysis was performed using Comprehensive Meta-analysis software 2.0.
Results
Literature Search
The result of literature search and study selection process was recorded in Figure 1. The search yielded 33 articles (30 from PubMed and 3 from references). Twenty of those were not included for the review because they were animal studies, review articles, partially duplicate reports, or reporting islet yield in different unit. The rest of the 13 articles were reviewed as full. Of the 13 articles, 3 reported results for subgroups (4,6,12) and each of the subgroups was considered as separate study. Two articles involved three-group comparison: UW alone, TLM alone, and TLM following UW storage (13,17). For both articles, the TLM following UW group had about two to three times longer CIT than UW group (15.6 and 26.6 vs. 8.4 and 8.9); however, TLM alone group and UW group had comparable CIT (8.8 and 11.0 vs. 8.4 and 8.9). Therefore, the UW + TLM versus UW comparison was excluded from analysis for both articles. In addition, one article reported islet yield in the unit of IE (islet equivalent) instead of IE/g and was excluded for the analysis on islet yield, but it was used for the analysis of viability (7). As a result, a total of 17 studies involving 799 pancreata were included in the meta-analysis, 16 for islet yield and 12 for viability.

Flow chart of study selection.
Study Characteristics
Missing data on donor characteristics remained unavailable after contacting the authors. Each study compared two preservation methods and involved two participant groups. Statistical tests revealed no significant difference between the two groups in any of the donor pancreas characteristics (Table 1).
Between-Group Summary Statistics of Donor Characteristics: Islet Yield and Viability

TLM, two-layer method; UW, University of Wisconsin; CIT, cold ischemic time; BMI, body mass index.
Cross-study variations were observed in implementing pancreas preservation and islet isolation methods: islet yield was reported either as one of prepurified, postpurified, postcultured, or as various combinations. Postpurified yield was used in the analysis whenever it was available. Eight studies in 6 articles (4,7,13,15,17,26) reported TLM being implemented immediately after organ procurement, and the remaining 9 studies in 7 articles (6,12,14,18,24,25,27) reported pancreata transferred into TLM after UW storage for various lengths of time. Two studies (12,14) had prolonged CIT (mean CIT >20 h) for both TLM and UW groups, the rest of 15 studies (4,6,7,12,13,15,17,18,24–27) had mean CIT <20 h for both groups, including 3 studies (4) that only reported the range of CIT with the maximum to be 18 h. Three studies were designed to test the effect of trypsin inhibitor (Pefabloc) (14) or cytoprotective factor (nicotinamide) (6) during islet isolation process. Subgrouping analyses were performed based on these variations.
Meta-Analysis of Islet Yield
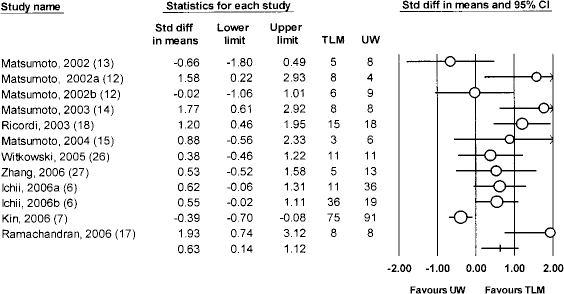
A total of 633 pancreata were included in the meta-analysis of islet yield, 370 stored in UW alone and 263 stored in TLM alone or in TLM following a period of time in UW (Fig. 2). Heterogeneity was significant with p = 0.001. The result showed a significant beneficial effect with TLM as measured by weighted SMD [0.74 (0.44–1.04)] (Fig. 2).

Forest plots for meta-analysis of islet yield comparing TLM with UW using all studies. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar. The test for heterogeneity across all studies was significant (Q15 = 37.6, p = 0.001).
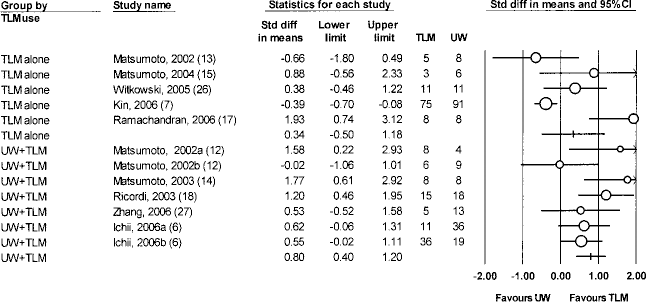
Meta-analysis was performed on subgroups based on the feature of TLM use, length of CIT, and chemical use (Figs. 3, 4, 5). All subgroups yielded significant differences in favor of TLM: 9 studies with TLM used following a period of UW storage [UW + TLM, 0.82 (0.57–1.07)], and 7 with the use of TLM alone [0.56 (0.05–1.07)]; 2 studies with prolonged CIT [>20 h, 1.38 (0.54–2.22)], and 14 shorter CIT [<20 h, 0.68 (0.37–0.98)]; 3 studies with use of chemical [0.58 (0.17–0.98)], and 13 with no use of chemical [0.79 (0.42–1.16)].

Forest plots for subgrouping analysis of islet yield comparing TLM with UW. Studies were grouped by TLM use: UW + TLM—TLM used following a period of storage in UW solution, TLM alone—TLM used immediately after organ procurement. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.

Forest plots for subgrouping analysis of islet yield comparing TLM with UW. Studies were grouped by CIT: <20 h—studies with mean CIT <20 h for both TLM (TLM alone or UW + TLM) and UW groups, >20 h—studies with mean CIT >20 h for both TLM (TLM alone or UW + TLM) and UW groups. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.

Forest plots for subgrouping analysis of islet yield comparing TLM with UW. Studies were grouped by chemical use: Yes—special chemical (Pefabloc or nicotinamide) was used during islet isolation process, No—no use of special chemical. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.
Meta-Analysis of Islet Viability
Twelve studies reported islet viability and a total of 422 pancreata were included in the meta-analysis, 231 stored in UW alone and 191 stored in TLM alone or in TLM following prestorage in UW (Fig. 6). Heterogeneity was significant with p < 0.0001. The use of TLM significantly increased islet viability [0.63 (0.14–1.12)].
Forest plots for meta-analysis of islet viability comparing TLM with UW using all studies. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar. The test for heterogeneity across all studies was significant (Q11 = 46.9, p < 0.0001).
The same sets of subgrouping analysis were performed on islet viability as islet yield: 7 UW + TLM studies [0.80 (0.40–1.20)] and 5 TLM alone studies [0.34 (-0.50–1.18)]; 2 with prolonged CIT [1.69 (0.81–2.57)] and 10 with shorter CIT [0.46 (-0.03–0.94)]; 3 with chemical use [0.81 (0.22–1.39)], and 9 with no chemical use [0.54 (–0.08–1.16)] (Fig. 7, 8, 9).
Forest plots for subgrouping analysis of islet viability comparing TLM with UW. Studies were grouped by TLM use: UW + TLM—TLM used following a period of storage in UW solution, TLM alone—TLM used immediately after organ procurement. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.

Forest plots for subgrouping analysis of islet viability comparing TLM with UW. Studies were grouped by CIT: <20 h—studies with mean CIT <20 h for both TLM (TLM alone or UW + TLM) and UW groups, >20 h—studies with mean CIT >20 h for both TLM (TLM alone or UW + TLM) and UW groups. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.

Forest plots for subgrouping analysis of islet viability comparing TLM with UW. Studies were grouped by chemical use: Yes—special chemical (Pefabloc or nicotinamide) was used during islet isolation process, No—no use of special chemical. Area of the symbol for each primary study (circle) is proportional to study weight. The pooled standardized mean difference (random effects) and 95% confidence intervals are represented by the bar.
Discussion
Islet yield and viability were chosen as the outcomes for the analysis because they are both key quality indicators for islet transplantation (21). The current islet isolation techniques allow recovery of less than 500,000 IE viable islets from a pancreas stored in UW solution. For a recipient who weighs more than 50 kg, more than one donor would be required to provide enough islets for transplantation. UW solution has been effective in pancreas preservation in the case of whole-pancreas transplantation, where the human pancreas can be preserved by UW for more than 24 h (2). However, prolonged cold storage in UW significantly reduced the yield of viable islets. The optimal and maximum cold storage time in UW was considered to be up to 8 and 18 h (9,19), respectively. Unfortunately, efforts to transport the pancreas graft to the center of islet transplantation within 8 h add considerable expense and logistical challenges.
The high-oxygen solubility in PFD made it promising to prolong the effective cold storage time in TLM. However, conflicting results have been reported on the effectiveness of TLM (4,7). In addition, Agrawal et al. reported meta-analysis of the TLM and they concluded there were no clear benefits of the TLM before human islet isolation and possible benefit of the TLM for marginal donors (old donor or prolonged preservation) (1). Compared to Agrawal et al.'s meta-analysis, we have performed more subgrouping analyses. Across the studies we used for the meta-analysis, there existed a large amount of variation and the heterogeneity test was significant for both outcomes. Three main sources of variation (immediacy of TLM, length of CIT, and use of chemicals) were identified and subgroup analyses were performed accordingly.
The results of all subgrouping analyses consistently showed that TLM was superior to UW in islet yield. In terms of immediacy of TLM, the subgrouping analyses in Agrawal et al.'s (1) and our study both suggested that the beneficial effect of TLM over UW was more evident with UW + TLM than TLM alone. However, this was conflicting with the result of UW + TLM versus TLM alone comparison in Agrawal et al.'s study, where UW + TLM resulted in significantly lower yield than TLM alone. The advantage of TLM alone is avoiding UW storage-related cold ischemic injury. In order to perform TLM alone, TLM needs to be initiated at procurement sites. For this purpose, oxygen static charged TLM is usually used because continuous oxygenation is very difficult and sometimes impossible during transportation from procurement sites to islet isolation laboratory (13). However, oxygen static charged TLM needs precaution to confirm PFD is fully oxygenated before use and the pancreas is adequately immersed in PFD (16). This seems the reason oxygen static charged TLM is beneficial only when islet specialists can participate in pancreas procurement as indicated by Noguchi et al.'s study (16). On the contrary, the advantage of TLM following UW is no need of specialists for pancreas procurement and no difficulty for full oxygenation of PFD using continuous oxygen supply. Therefore, if islet isolation laboratory members are not familiar with the TLM technique or pancreas procurement, TLM following UW should be a better choice. In the meta-analysis by Agrawal et al., only one study was used for UW + TLM versus TLM comparison. Hopefully, more studies will be available in the near future and better evidence can be compiled for UW + TLM versus TLM comparison.
Regarding to the length of CIT, in contrary to the common view that prolonged CIT would have negative effect on islet outcomes, stronger beneficial effect was demonstrated by two studies from Matsumoto's group with prolonged CIT (>20 h) than those with shorter CIT (<20 h). Because TLM contains PFD, which has high oxygen solubility and enables pancreas to generate ATP for up to 96 h, it can protect pancreas from swelling more effectively than UW solution. Over prolonged CIT, the beneficial effect of TLM over UW would be magnified. It was also important to note that one of the two studies (14) used trypsin inhibitor Pefabloc during islet isolation process and it was suggested that inhibiting trypsin could increase islet yield by reducing trypsin-mediated destruction of liberated islet and therefore allow longer preservation time (14).
When we analyzed based on viability, although the pooled result from all studies showed a beneficial effect of TLM on viability, the results for each subgroup varied. The use of TLM alone, short CIT, or no chemical use all yielded similar result between TLM and UW groups, but UW + TLM, long CIT, or use of chemical all significantly improved islet viability (Figs. 6–9). Again the benefit of oxygenation of pancreas by the TLM for islet viability over UW would be magnified after prolonged preservation. Pefabloc and nicotinamide increased islet outcomes in both TLM and UW groups in 3 studies. Our meta-analysis demonstrated that the use of these chemicals did not affect TLM versus UW comparison in islet yield (Fig. 5), but did magnify the beneficial effect of TLM on viability. Of the 3 studies of chemical use, the one by Matsumoto et al. (14) using trypsin inhibitor contributed the most to the positive effect of TLM.
TLM seems beneficial over UW for pancreas preservation before islet isolation; however, it should be pointed out that there were limitations in this meta-analysis. The missing data on donor characteristics made it impossible to accurately evaluate the balance between the UW and TLM groups. Another limitation lies in the fact that several subgroups had very small sample sizes (n = 2 for prolonged CIT group and n = 3 for chemical use group), which resulted in wide confidence intervals for the pooled estimates. Lastly, subgroup analyses were performed on three sources of variation (TLM use, CIT, and chemical use) identified from the data. We are aware that other factors relating to techniques of handling pancreata in the operation room and/or in the lab might also contribute significantly to the variation in the outcomes; however, not enough detail was provided in primary studies and the description of the methods was inconsistent across studies in terms of trimming of pancreata. Therefore, we could not use that as a grouping factor.
Despite the limitations, this meta-analysis clearly demonstrated the beneficial effect of TLM on islet yield compared with UW. Three studies were excluded from the analysis of islet yield because the outcome was reported in the unit of IE instead of IE/g. However, a closer look at each individual study revealed that all three studies reported beneficial effects of TLM over UW method in islet yield. Therefore, including them should not change the direction of the comparison, but would rather enhance the results we had. The various subgrouping analyses also provided some guidelines on how and when to implement the TLM method. Preservation of pancreata in TLM following UW resulted in even greater beneficial effect than in TLM alone when islet isolation members are not familiar with the TLM technique and pancreas procurement. In conclusion, TLM was beneficial for both islet yield and viability when prolonged cold storage time was involved; however, the benefit was not clear when short-term cold storage time was involved.
Footnotes
Acknowledgments
Author contributions: H.Q. had full access to all of the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis; Study concept and design (S.M., H.Q., E.B.D); Acquisition of data (H.Q.); Analysis and interpretation of data (H.Q., E.B.D., S.M.); Drafting of the manuscript (H.Q., E.B.D.); Critical revision of the manuscript for important intellectual content (E.B.D., S.M., G.B.K.); Statistical analysis (H.Q., E.B.D.); Obtained funding (E.B.D.); Administrative, technical, or material support (E.B.D., G.B.K.); Study supervision (E.B.D.). This work was supported by Baylor Health Care System intramural funds. The funding source for this study played no role in the design and conduct of the study; in the collection, management, analysis, and interpretation of the data; or in the preparation of the manuscript. The funding source did not review the manuscript. We thank Kathleen Richter, MS, MFA, ELS, medical writer from Institute for Health Care Research and Improvement, Baylor Health Care System for assistance with formatting the manuscript for submission.