
Abstract
Stem cells isolated from amniotic fluid are known to be able to differentiate into different cells types, thus being considered as a powerful tool for cellular therapy of different human diseases. In the last 4 years, amniotic fluid-derived stem (AFS) cells have been shown to express embryonic and adult stem cell markers. These cells can be considered an intermediate stage between embryonic stem cells and adult stem cells. AFS cells can give rise to adipogenic, osteogenic, myogenic, endothelial, neurogenic, and hepatic lineages, inclusive of all embryonic germ layers. AFS cells have a high renewal capacity and can be expanded for over 250 doublings without any detectable loss of chromosomal telomere length. Taken together, all these data provide evidence that amniotic fluid represents a new and very promising source of stem cells for research, as well as clinical applications. Certainly stem cells from amniotic fluid will be useful both for a customized cell supply for newly born children and for banking cells to be used for therapeutic cell transplantation in immunogically matched recipients. Further investigations are also warranted to fully explore the amniotic cells' potential for adult human disorders.
Introduction
In recent years, accumulating evidence has demonstrated the ability of amniotic fluid-derived stem (AFS) cells to differentiate into multiple lineages (7,11,18,21,22,28,29). Indeed, the demonstration of the capacity of clonal AFS cells to produce cell types inclusive of all embryonic germ layers allowed the classification of these cells as pluripotent AFS cells (1,4,27). Human amniotic fluid (HAF) obtained during the process of amniocentesis contains a variety of AFS cells originating from embryonic and extra-embryonic tissues (21).
The types and properties of amniotic fluid cells vary with gestational age. When grown in culture, AFS cells can be separated into adhering and dividing colony-forming cells, and nonadhering cells. Based on their morphological and growth characteristics, amniotic fluid cells can be classified into three types: epitheloid E-type cells, amniotic fluid-specific AF-type cells, and fibroblastic F-type cells (22). AF-type and E-type both appear at the beginning of cultivation. AF-type cells persist during the cultivation process, while E-type cells soon show a significant decrease. E-type cells have been thought to derive from fetal skin and urine, AF-type cells from fetal membranes and trophoblasts, and F-type cells from fibrous connective tissue and dermal fibroblasts. AF-type cells produce estrogen, human chorionic gonadotropin, and progesterone, which suggests that these cells originate from trophoblast tissue. Also, F-type cells are considered to originate from mesenchymal tissue. Approximately 1% of the cells in cultures of human amniocentesis specimens obtained for prenatal genetic diagnosis express the surface antigen c-Kit (CD117). This receptor protein is present on human ES cells, primordial germ cells, and many somatic stem cells.
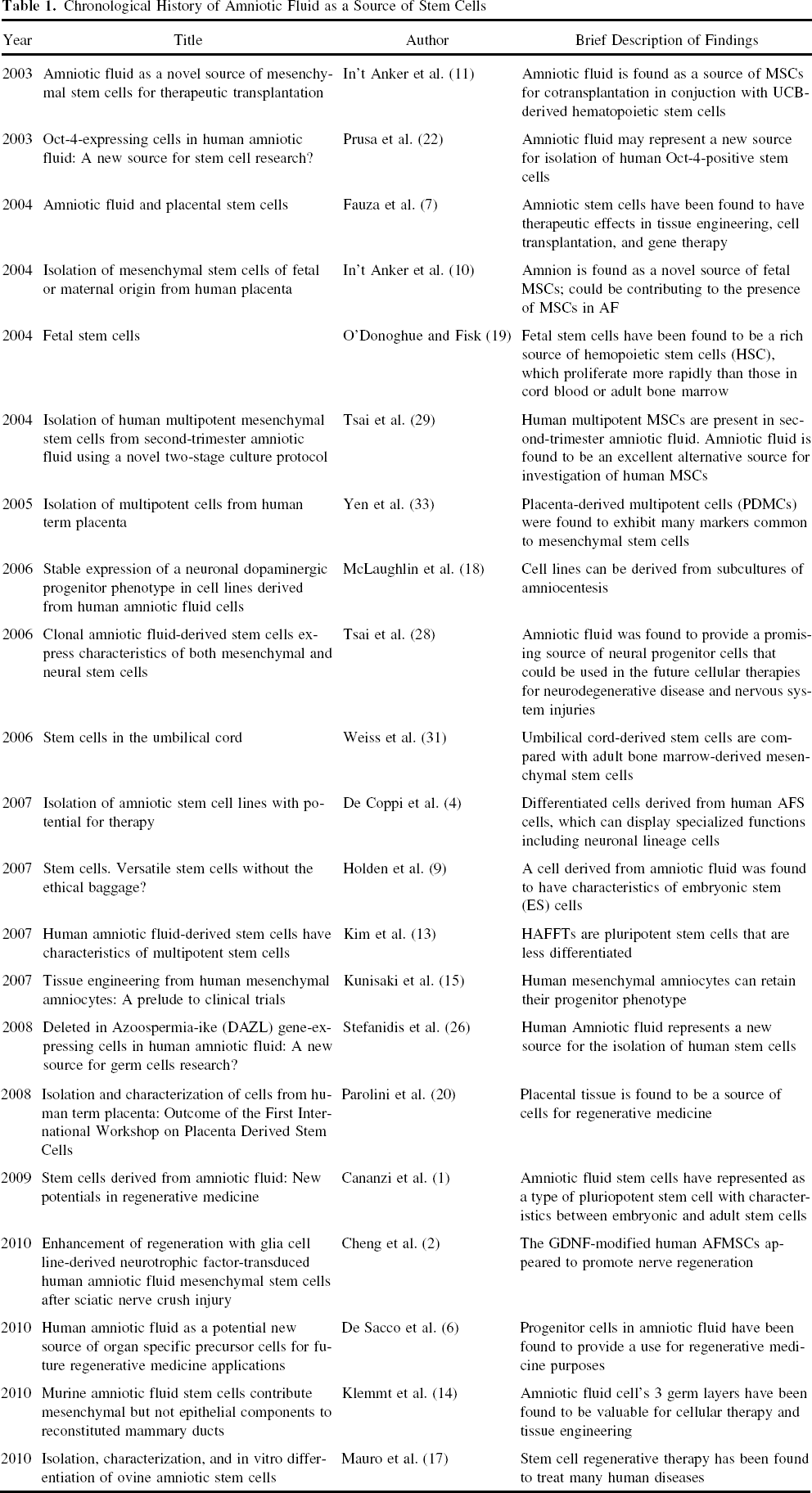
However, AFS cells are different both from pluripotential ES cells and from multipotential adult stem cells, and may represent a new class of AFS cells whose properties of plasticity exist somewhere between embryonic and adult stem cell types. Moreover, about 90% of AFS cells express the transcription factor Oct-4, known to be expressed in embryonic carcinoma cells, embryonic germ cells, and embryonic stem cells. For this reason, these cells represent an intermediate stage between embryonic and adult stem cells in terms of their versatility (4,17). In addition, AFS cells were also found to show the pluripotent stem cell marker TERT, and have the capability to differentiate in osteogenic and smooth muscle (17). Unlike embryonic stem cells obtained from the inner cell mass of blastocysts, however, AFS cells do not form tumors after transplantation in mice (4). As a consequence, amniotic fluid could represent a safe and easily available source of AFS cells to be used for therapeutic purposes, circumventing any ethical objection, given that amniocentesis is a widely accepted form of prenatal diagnostic testing (1,4,7,9) (Table 1).
Chronological History of Amniotic Fluid as a Source of Stem Cells
Amniotic Fluid-Derived Mesenchymal Stromal Cells
Multipotent mesenchymal stromal cells (MSCs) possess the ability to regenerate and differentiate into specific functional cells, making them promising cell graft sources for tissue engineering and cell-based therapeutics. In addition, human amniotic fluid-derived mesenchymal stromal cells (AFMSCs) have been demonstrated to aid in peripheral nerve regeneration and local delivery of neurotrophic factors (2). AFMSCs can be isolated from second-trimester amniotic fluid without interfering with the process of fetal karyotyping. AFMSCs have phenotypic characteristics similar to those of MSCs derived from other sources such as umbilical cord, blood, and bone marrow; all are positive for mesenchymal markers such as CD90, CD105, CD73, CD166, but negative for the hematopoietic markers such as CD45, CD34, and CD14 (25). A quantity of 2 ml amniotic fluid is sufficient to culture these cells. Most importantly, AFMSCs express Oct-4 mRNA and protein, a transcription factor expressed in embryonic carcinoma cells, embryonic stem cells, and embryonic germ cells (22,29).
A variety of protocols have been used for the isolation of AFMSCs and their differentiation into several cell lineages, including the use of the immunoselection with c-Kit-specific antibodies in order to isolate AFS cells starting from confluent human amniocentesis cultures (4). On the other hand, other groups directly cultured amniotic fluid cells in media allowing the proliferation of AFMSCs, and subsequently induced their differentiation (7,10,21,29). However, because studies have recently reported that c-Kit-selected cells from human amniotic fluid can produce abnormal cell differentiation and host immune response after transplantation in rat myocardium (3), a protocol based on the direct culture of amniotic fluid cells without any selection could provide a better chance for homing and differentiation after transplant.
AFS cells have a high renewal capacity and can be expanded for over 250 doublings without any detectable loss of chromosomal telomere length (4). Nevertheless, under specific inducing conditions AFS cells are able to produce lineages representative of the three embryonic germ layers. These cells can become nestin-positive neural stem cells, and then dopaminergic and glutamate-responsive neurons. In appropriate medium, AFMSCs also form functional osteoblasts that produce mineralized calcium. Furthermore, hepatic lineage cells obtained by differentiation of AFMSCs are able to secrete high levels of urea and express liver proteins such as albumin, α-fetoprotein, hepatocyte nuclear factor, and growth factor (4,27).
Gene Expression Profiles of Afmscs
AFMSCs possess immunophenotypes and gene expression profiles that are largely characteristic of undifferentiated cells (13). RT-PCR analysis showed that AFMSCs express genes for Rex-1, SCF, GATA-4, vimentin, CK18, HLA ABC, and FGF-5 throughout the culture period, and they express genes for BMP-4, nestin, AFP, and HNF-4α. These proteins are expressed in different tissues. Desmin is well known to play an important role in cardiac and skeletal muscle function. GATA-4 is a cardiac-specific member of the GATA family of zinc-finger transcription factors. FGF-5 regulates neuron differentiation and survival. Nestin, a specific marker for neural stem cells, is also found in other differentiating cells, including muscle and myocardium, and BMP-4 appears to play a role in chondrogenesis and articular cartilage repair as well as in bone formation. These expression profiles suggest that AFMSCs have the potential to differentiate into cardiomyocytes, as well as other mesodermal derivatives, in addition to neural cells (2,4). These results show that AFMSCs are able to differentiate into adipocytes, osteocytes, chondrocytes, and neuronal cells, can express many pluripotent stem cell-specific genes, and proliferate well during ex vivo expansion.
Flow Cytometry of Afmscs
AFMSCs are positive for class I major histocompatibility (MHC) antigens (HLA-ABC), and some cells are weakly positive for MHC class II (HLA-DR). They also are positive for stage-specific embryonic antigen (SSEA), a marker expressed by ES cells, but generally not by adult stem cells. However, the AFS cells do not express other surface markers characteristic of ES and embryonic germ (EG) cells; few are weakly positive for Tra-1 (4). Furthermore, AFMSCs express collagen types I, II, III, IV, and XII, fibronectin, CD44 (homing cell adhesion molecule, HCAM), CD54 (intercellular cell adhesion molecule-1, ICAM-1), CD31 (platelet/endotheliala dhesion molecule-1, PECAM-1), CD106 (vascular cell adhesion molecule-1, VCAM-1), α-SMA (α-smooth muscle actin), CK18, desmin, vimentin, vWF, FSP proteins (13). There are no differences in antigen expression based on gestational age or the type of culture medium used (15). Flow cytometric analysis demonstrated the presence of DAZL and C-kit-expressing cells in amniotic fluid cell populations (26). DAZL proteins are germ cell-specific, RNA-binding proteins essential for gametogenesis. This expression profile is of interest because it demonstrates the expression in the AFMSCs of some key markers of the embryonic germ cell (12).
Neurogenic Cells in Human Afs Cells
AFS cells express neuronal marker genes (such as CD133, nestin, neurofilament, CNPase, p75, BDNF, and neurotophin-3) (21). The presence of many dopaminergic markers (TGF-β3, FGF8, Shh, and β-catenin) in AFS cells demonstrates the existence of committed neuronal progenitor cells that corresponds to a highly transcriptional profile similar to mesencephalic dopaminergic neurons (2,18). AFS cells can survive, migrate along significant distances, and differentiate when transplanted into adult rat brain (4,8). Moreover, AF-MSCs obtained from amniotic fluid cells after 3 weeks of culture have been transplanted into normal and cerebral ischemic rat brains and revealed that the transplanted cells were able to migrate from the injection site, both at short and long distances along the corpus callosum, and to gain access to multiple brain regions. The positive effects obtained by transplantations of MSCs may be ascribed to the production of trophic factors and cytokines by these cells as well as to the increase in the levels of neurotrophic factors within the ischemic region in response to the administration of MSCs. Nevertheless, further studies are required to evaluate the histopathological ischemic changes in the brain related to the effect of treatment with AFS cells.
Possible Treatment Options with Afs Cells
Studies have also turned toward using AFS cells to treat various ailments. One such study showed AFS cells for support in mammary gland regeneration (14). Further studies have shown that differentiation aids in muscular and cardiac diseases such as an ischemic heart disorder (5,17). In addition, AFS cells have also been shown to have multiple applications in cellular therapy and tissue engineering (1,6,14,32). These exciting cell-based treatment options could lead to further remedies against human and veterinary disorders (30) (Table 2).
Diseases Targeted by Stem Cell Therapy Using Amnion Cells

Review article.
Advantages of Afs Cells
Much of the recent excitement surrounding human progenitor cells and AFS cells is due to their potential use in replacing dysfunctional cells within a tissue. As ethical and logistic issues appear to limit the use of embryonic cells (ESCs), special attention has been recently paid to the use of alternative sources of stem cells, such as mesenchymal cells from bone marrow (BM), amniotic fluid, placenta, and umbilical cord (19). Adult BM is the common source of MSCs used in clinical settings. However, the use of adult BM has some limitations. First, the frequency of MSCs in adult BM is low. Second, harvesting BM from a patient is an invasive procedure. Therefore, the search for alternative sources of MSCs useful for clinical application is important (11). Currently, the presence of MSCs in umbilical cord blood is still contested, coupled with reports showing that isolation of such cells is difficult, resulting in low yield and interindividual variations (24,31).
Amniotic fluid contains a heterogeneous population of cells that originate from fetal tissues, and recently this also has been suggested to be a novel source of stem cells. Amniotic fluid is easily collected by ultrasound-guided transabdominal puncture. Compared to embryonic stem cells, amniotic stem cells can be obtained without destroying human embryos, thus alleviating much of the ethical controversy. Furthermore, they are easily retrieved during routine prenatal testing, and they can be isolated and grown in laboratory dishes. The expansion potential of AFMSCs exceeds that of BM-derived MSCs (11). Also, amniotic fluid-derived stem cells express embryonic and adult stem cell markers and expand extensively without feeder cells. The presence of certain markers of undifferentiated cells shows that AFMSCs may be less differentiated than most BM-MSCs, and may more closely resemble pluripotent ES cells; thus, more possibilities lie with these cells. Expression profiles suggest that AFS cells have the potential to differentiate into cardiomyocytes as well as other mesodermal derivatives, in addition to neural cells (4).
Studies with the transplantation therapy of human embryonic stem cells are also hampered by possible immunological rejection and tumorigenicity. As noted above, unlike embryonic stem cells obtained from the inner cell mass of blastocysts, AFS cells are not tumorigenic after transplantation in mice (4). The placenta is an additional source for MSCs. The human placenta is a feto-maternal organ, formed by both fetal and maternal tissue. This organ is discarded postpartum, after having performed its necessary function of supporting the embryo and fetus. Stem cells isolated from term postpartum placenta have a variety of advantages. Cells derived from the placenta are still of fetal origin and may be superior to adult stem cells in many aspects. No invasive procedure is necessary to obtain the organ, because the placenta is expelled after the birth of the neonate. Furthermore, there are no ethical concerns generated, because the organ would have been discarded otherwise (7,11,20,33). The detection of ESCs surface markers on placenta-derived MSCs (PDMCs) suggests that these may be very primitive cells. If this is correct, the renewal and differentiation capacity may be more extensive than the adult stem cell. Although some of the PDMCs cultures have been passaged over 15 times (approximately 50 population doublings), the immortality of these cells remains to be demonstrated.
Limitations of Afs Cells
AFS cell cost is much higher than many other variations of stem cells. Because the membrane is nonspecific, comparisons between different tests will be difficult (23). Although generally considered as an immune-incompetent graft source, owing largely to their immature immune system, AFS cells' immunogenic properties and phenotypic instability lead to problems with in vivo transplantation (3). Studies have also shown that placenta-derived stem cells lack morphogenetic development due to absence of spatial signals (16). This may cause problems during cell growth, where an over-accumulation of cells could lead to spontaneous differentiation. In addition, investigations are warranted to reveal evidence of any unregulated meiotic divisions in these placenta-derived stem cells. These unregulated divisions not only may lead to the possibility of malignant tumors but also may result in cellular defects. These adverse side effects, among others, should be examined to reveal the safety profile of AFS cells along with efficacy outcome parameters.
Conclusion
The isolation, expansion, and transplantation of stem cells derived from the amniotic fluid have raised great interest due to: a) the large accessibility of these cells by means of routinely amniocentesis; b) their ability of differentiate in several cell lineages; and c) the absence of tumorigenicity and the lack of ethical problems related to their use. Amniotic fluid can be considered as a powerful source of cells to be used for cell therapy in several human diseases (2,4). Of all the many sources of MSCs described to date, amniotic fluid has been increasingly accepted as the ideal one for cellular therapy of different human diseases. AFMSCs can be isolated relatively easily, proliferate quickly under standard culture conditions, and have a remarkable multilineage potential. In addition, and perhaps more importantly, a diagnostic amniocentesis is routinely offered to any mother with advanced age or with a fetus in whom a congenital anomaly has been suggested by prenatal imaging or serological tests on peripheral blood. Moreover, only a small quantity of amniotic fluid is sufficient enough to culture these cells. An equally rich source of MSCs is the placenta, a strategically related membrane organ to amniotic fluid. Whereas the proliferation capability of the placenta remains to be characterized, AFS cells have already been shown to possess a high renewal capacity (1,4). Nonetheless, both AFS cells and placenta cells would require further examinations to better understand their precise stemness properties and their potential clinical applications (11). Taken together, these data provide evidence that amniotic fluid represents a new and very promising source of engraftable stem cells for treating human disorders.
Footnotes
Acknowledgments
C.V.B. is funded by SanBio Inc., Celgene Therapeutics, Inc., Neuralstem Inc., and James and Esther King Biomedical Research Programs 09KB-01-23123 and 1KG01-33966. C.V.B. serves as consultant to stem cell-based companies and holds patent applications on stem cell-related technologies.