
Abstract
BACKGROUND:
Magnetic resonance imaging (MRI) is the preferred examination approach for patients with suspected cervical spondylotic myelopathy (CSM).
OBJECTIVE:
To investigate the predictive value of MRI spinal cord swelling on the prognosis of decompression surgery in patients with CSM.
METHODS:
A retrospective analysis of 115 patients with CSM who underwent decompression surgery was performed. According to whether cervical MRI showed spinal cord swelling, they were divided into a spinal cord swelling group and non-swelling group. The Modified Japanese Orthopaedic Association (MJOA) score, MJOA improvement rate and abnormal spinal cord enhancement rate in the two groups were compared before and after surgery. Multiple linear regression was used to analyse the influencing factors of the MJOA improvement rate.
RESULTS:
The time from symptom onset to operation (
CONCLUSION:
Patients with CSM with spinal cord swelling have less time from symptoms to surgery, and the degree of preoperative neurological deterioration is more obvious. Spinal cord swelling is an independent predictor of surgical prognosis in patients with CSM.
Introduction
Cervical spondylotic myelopathy (CSM) is caused by the degeneration of the cervical intervertebral junction structure, such as disc herniation, posterior vertebral spurs, uncovertebral joint hyperplasia, ossification of the posterior longitudinal ligament, hypertrophy or calcification of the ligamentum flavum, resulting in compression or ischaemia of the spinal cord, followed by spinal cord dysfunction [1]. The annual hospitalisation rate for CSM and related conditions is approximately 4.04 per 100,000 admissions, a figure that has increased approximately 1-fold in the last decade, with a 7-fold increase in the number of patients undergoing surgery each year [2]. Magnetic resonance imaging (MRI) is superior to computed tomography in revealing intervertebral discs, ligaments, subarachnoid space, and spinal cord and epidural compression and is the preferred examination approach for patients with suspected CSM [3, 4]. Studies have suggested that MRI intraspinal signal changes have some significance in predicting postoperative recovery in patients with CSM [5]. Although CSM is the most common form of chronic spinal cord injury, the predominant imaging presentation is limited to high signal T2-weighted imaging (T2WI) at one or more disc levels within the cervical medulla; spinal cord swelling occurs rarely. Spinal cord swelling often occurs in patients with acute spinal cord injury, intramedullary tumours and inflammatory lesions of the spinal cord but is rarely seen in patients with CSM [6, 7, 8], resulting in a lack of clinical understanding of the imaging and clinical features of spinal cord swelling in patients with CSM. Moreover, the high incidence of complications and low accuracy of pathological diagnosis of spinal cord puncture biopsy have limited its application [6], leading to delays in the correct treatment of these patients as a result of misdiagnosis [7]. Previous studies on patients with CSM presenting with spinal cord swelling are mainly case reports [9]. Therefore, in this study, we retrospectively analysed the MRI and clinical features of patients with CSM with spinal cord swelling to evaluate the predictive value of this indicator for the prognosis of these patients.
Materials and methods
General information
A total of 115 patients diagnosed with CSM and treated surgically at our hospital between September 2020 and September 2021 were retrospectively analysed. The patients were divided into a spinal cord swelling group and a non-swelling group depending on whether spinal cord swelling was present on cervical MRI scans. The spinal cord swelling group was further divided into an enhanced group and non-enhanced group according to whether there was definite high signal intensity after an intraspinal injection of contrast agent in T1-weighted imaging (T1WI). Informed consent was obtained from the patients and their families. This study was approved by the Ethics Committee of the Third Hospital of Hebei Medical University (No. W2022-027-1).
Inclusion criteria
2.2.1 Inclusion criteria for patients with CSM: (1) Presence of typical clinical manifestations of CSM; (2) presence of spinal stenosis with various causes on MRI of the cervical spine; (3) presence of spinal high signal T2WI at the location of spinal stenosis.
Exclusion criteria: (1) History of external cervical trauma; (2) other types of cervical spondylosis; (3) lack of imaging data; (4) combination of spinal tumours, acute inflammation or infection and other diseases.
2.2.2 Inclusion criteria for patients with CSM in the spinal cord swelling group: (1) high signal in the cervical medulla in sagittal T2WI in more than one vertebra; (2) the high signal border in T2WI was blurred or faint; (3) the anteroposterior diameter of the sagittal spinal cord at the location of the high signal in the T2WI was larger than that at the location without a high signal, as shown in Fig. 1. The remaining patients who did not meet the inclusion criteria of the CSM spinal cord swelling group were classified as the CSM non-spinal cord swelling group.
T2WI image of cervical spine with spinal cord swelling. Male patient, 56 years old, mainly admitted with numbness and weakness in both upper limbs for 4 months. T2WI of the cervical spine showed a long T2 signal visible at the level of cervical 6-thoracic 1 of the spinal cord, with a lesion extending over more than one vertebral body, with blurred borders and a lesion location larger than normal in diameter. 
2.2.3 Inclusion criteria for patients with CSM in the spinal cord swelling enhancement group: a clear high signal was revealed after the intraspinal cord contrast injection on the T1WI, as shown in Fig. 2A–D. The remaining patients who did not meet the inclusion criteria of the CSM spinal cord swelling enhancement group were classified as the CSM spinal cord swelling non-enhancement group.
Abnormal enhancement signal in the spinal cord of CSM patients in the spinal cord swelling group. Female patient, 65 years old, admitted to the hospital mainly due to upper extremity numbness and lower extremity weakness for more than 10 days. A is a conventional sagittal T1WI image of the patient with no clear abnormal signal in the spinal cord. B is a sagittal T2WI image with spinal cord swelling visible at the cervical 5–7 level. C is a sagittal T1WI compression lipid image of the patient before enhancement with no clear abnormal signal in the cervical medulla. D is a sagittal T1WI compression lipid image after enhancement, which shows significant abnormal enhancement within the spinal cord at the cervical 5–6 level.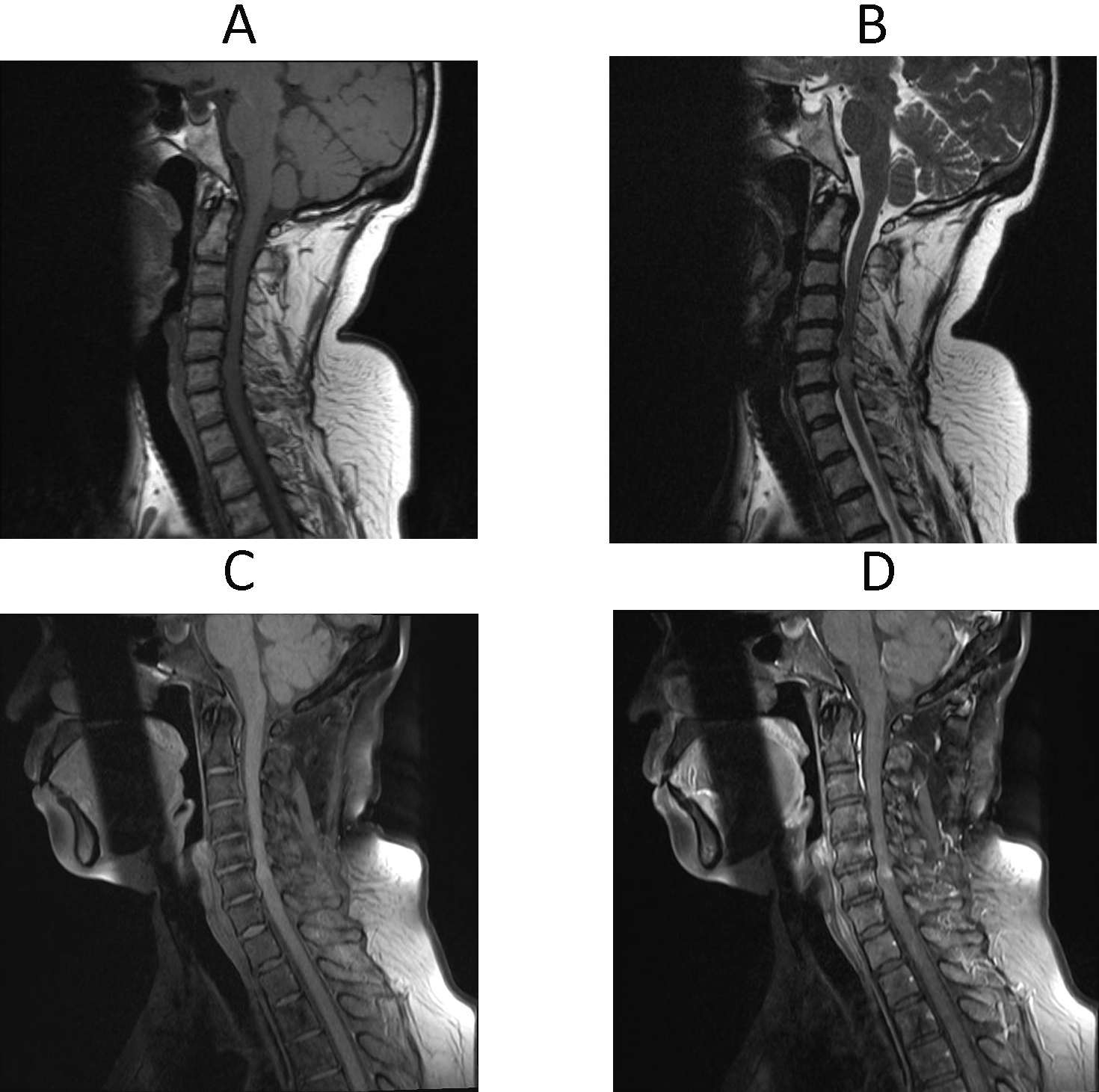
Participants underwent routine and enhanced MRI of the cervical spine using Siemens 3.0T superconducting magnetic resonance Verio. The use of contrast enhancement in patients with spinal cord swelling is a means of differential diagnosis. The enhancement of the spinal cord often represents a poor prognosis. This study grouped the patients with spinal cord swelling to determine whether enhancement of the spinal cord in these patients has different effects on the prognosis and judgement value. Assessments were completed by two associate chief physicians in spinal surgery and two associate chief radiologists. None of the physicians were aware of patient group assignment. The plain scan sequences included sagittal turbo-spin echo (TSE) T1WI (repetition time (TR): 530 ms, echo time: (TE) 11 ms), TSE T2WI (TR: 3,000 ms, TE: 105 ms), T2 inversion recovery sequence (TR: 3,400 ms, TE: 102 ms, inversion time: 200 ms, field of view (FOV): 280
Subsequently, 0.2 mmol/kg of gadoterate meglumine, a contrast agent, was injected by hand through the cubital vein at a flow rate of 2 mL/s. Axial (TR: 711 ms, TE: 12 ms), coronal (TR: 606 ms, TE: 11 ms) and sagittal (TR: 600 ms, TE: 12 ms) TSE T1 fat-suppressed sequences were performed, and enhanced scans were performed with a slice thickness of 3 mm and interslice distance of 0.3 mm. Specific indexes: (1) anteroposterior diameter of the narrowest spinal canal measured in sagittal T2WI; (2) C2–C7 cobb angle; (3) T1 slope; (4) cross-sectional area of the narrowest spinal canal measured on transaxial T2WI. These data were measured three times and averaged [10], as shown in Figs 3–6.
Measurement of the anterior and posterior diameters at the sagittal stenosis of the cervical spine in patients with CSM.
Measurement of the cross-sectional area of the spinal canal at the axial stenosis of the cervical spine in patients with CSM.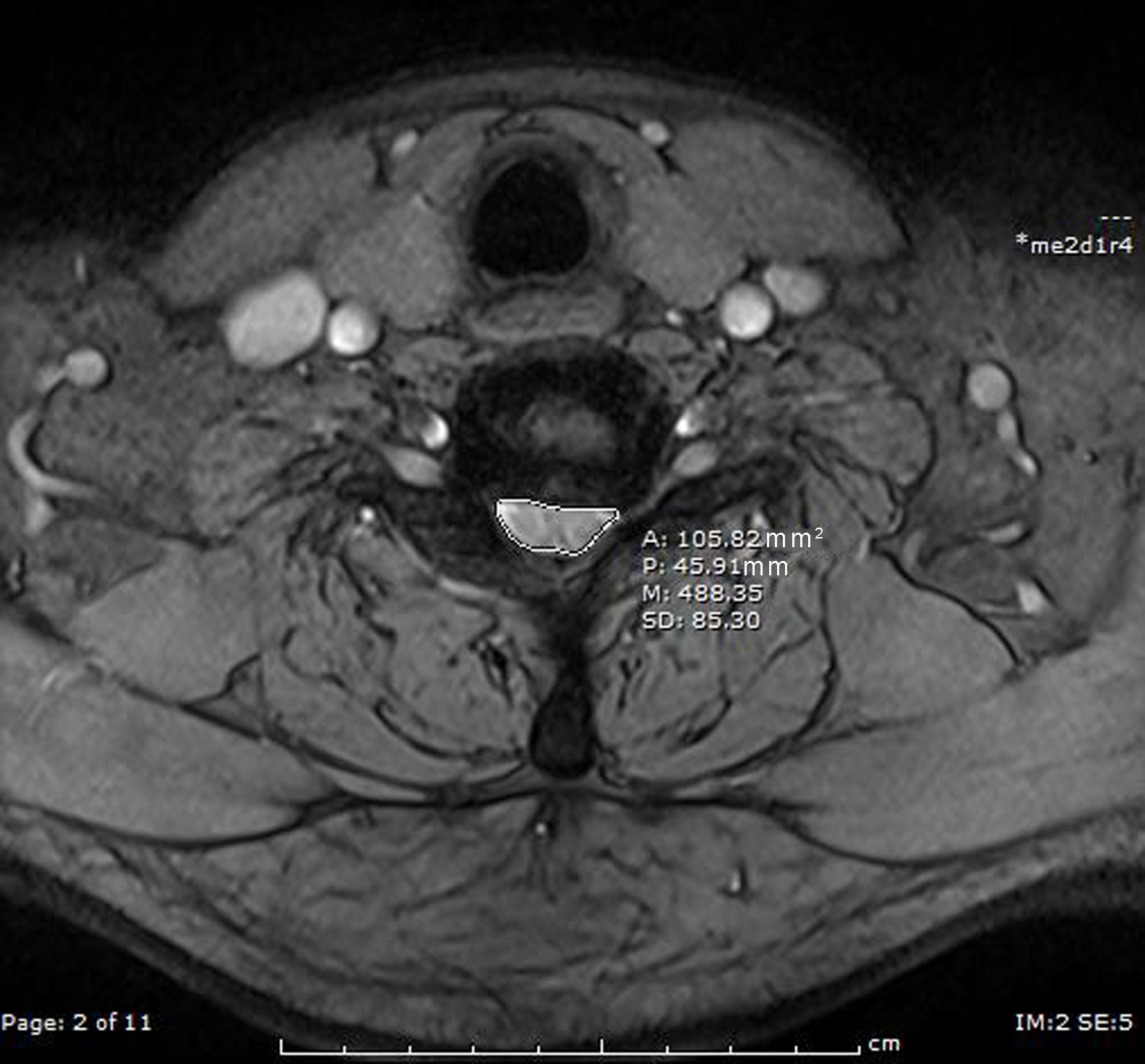
Cervical sagittal C2-C7 cobb angle measurement in CSM patients. The first line is parallel to the end plate of C2; the second line is parallel to the end plate of C7. The angle made by the vertical line of the two is the C2-C7cobb angle (the vertical line is omitted here). 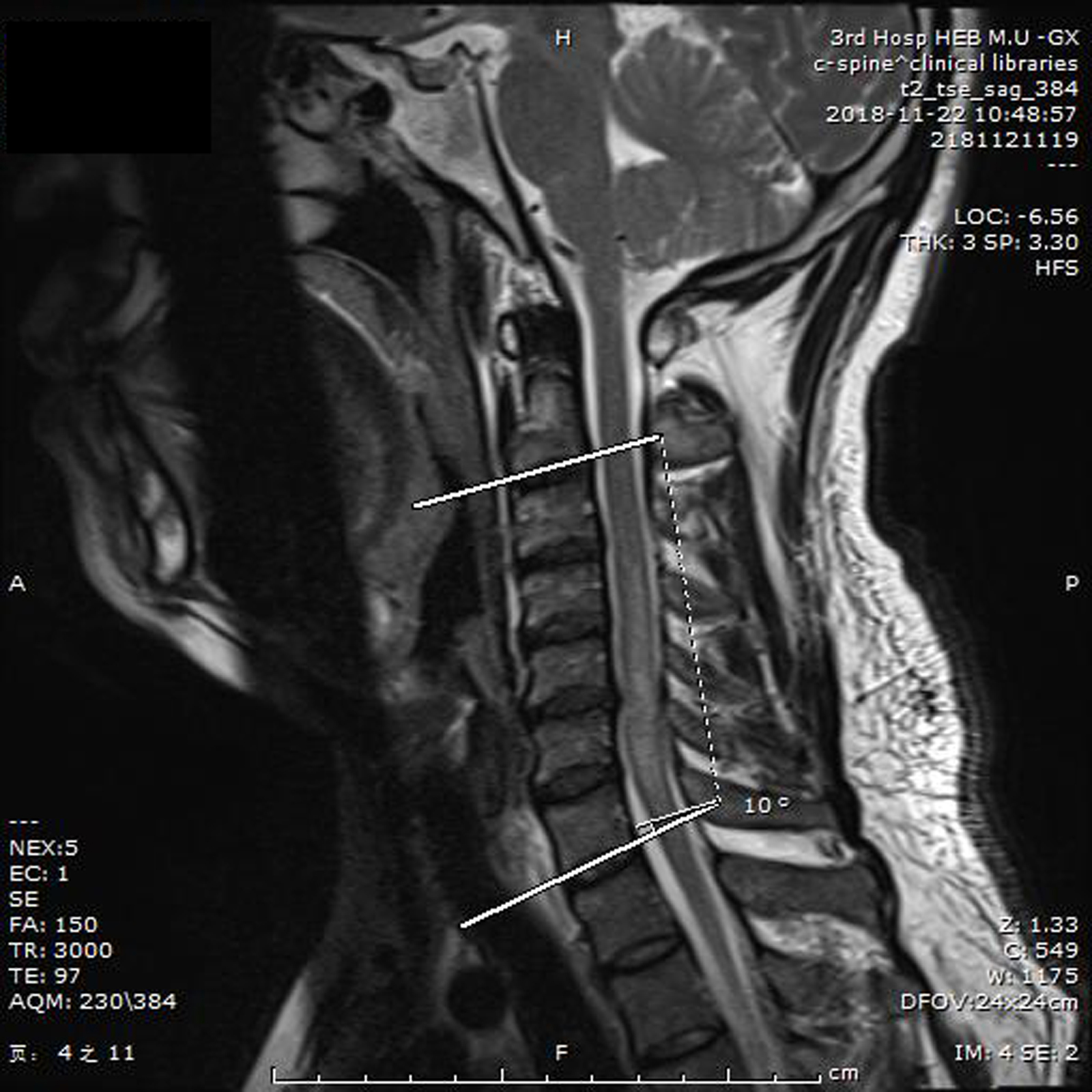
Measurement of T1 slope angle in the sagittal position of the cervical spine in patients with CSM. Chest 1 slope angle refers to the angle between the horizontal line and the upper end plate of chest 1.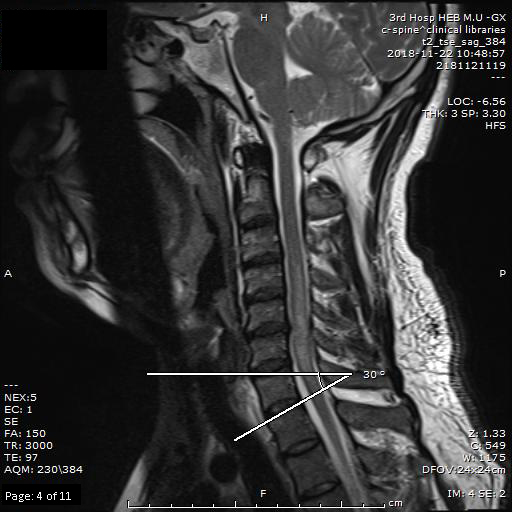
All patients underwent anterior cervical discectomy, decompression and fusion as well as posterior cervical open-door laminoplasty after MRI examination according to the compression location, level and postoperative spinal stability. After surgery, the patient was confined to bed rest and closely monitored to observe for neck haematoma, larynx oedema and dyspnoea, and symptomatic treatment such as for detumescence, infection prevention, pain relief and trophic nerve was administered. The patient wore a cervical collar 1 d after surgery and performed ambulation appropriately according to their personal condition; the drainage tube was removed within 2 d of surgery. The cervical collar was worn for a total of 6–8 weeks, and early rehabilitation was performed under the guidance of a rehabilitation physician to promote functional recovery, reduce postoperative complications and reduce hospital stays.
Research methodology
Relevant data on the patients consisting of height, weight, age, sex, time from symptom onset to surgical treatment (time of illness), preoperative MRI findings, preoperative Modified Japanese Orthopaedic Association (MJOA) score and postoperative MJOA score was collected through the hospital electronic medical record management system. Patient body mass index (BMI) was calculated as follows: BMI
Statistical methods
Statistical analysis was performed using SPSS version 26.0. A t-test was performed for age, BMI, time from symptom onset to surgery, preoperative MJOA score and postoperative improvement rate, anteroposterior diameter of the spinal canal, cross-sectional area, C2-C7 Cobb angle and T1 slope angle in the spinal cord swelling and non-swelling groups. A chi-square test was performed to assess the proportion of men and women in the spinal cord swelling and non-swelling groups and the proportion of spinal cord enhancement. A t-test was performed for each of the above statistics for the enhancement and non-enhancement subgroups within the spinal cord swelling group, and a chi-square test was performed for the male to female ratio. Multiple linear regression analysis was used to observe the effect of spinal cord swelling on the postoperative MJOA score improvement rate A value of
Results
General characteristics of study participants
The study involved 115 patients, with 51 patients in the spinal cord swelling group and 64 in the non-swelling group. No significant difference in sex between the two groups was detected (
Comparison of general characteristics between two groups of patients
Comparison of general characteristics between two groups of patients
The spinal cord swelling group was younger than the non-swelling group (49.9
Comparison of magnetic resonance and clinical features between the spinal cord swelling and non-swelling groups
Comparison of magnetic resonance and clinical features between the spinal cord swelling and non-swelling groups
The age of the spinal cord swelling enhancement group and non-enhancement group was 51.1
Comparison of magnetic resonance and clinical features between the enhancement and non-enhancement subgroups of the spinal cord swelling group
Comparison of magnetic resonance and clinical features between the enhancement and non-enhancement subgroups of the spinal cord swelling group
The correlation between the MJOA score improvement rate and age, BMI, anteroposterior diameter of the narrowest spinal canal, cross-sectional area, time from symptoms to surgery, C2–C7 Cobb angle and T1 slope was analysed using a Pearson correlation analysis. Age (
Relationship between MJOA score improvement rate and other factors
Relationship between MJOA score improvement rate and other factors
Age, time from symptoms to surgery, T1 slope, sex and spinal cord swelling were used as independent variables. Multiple linear regression analysis was performed using the MJOA score improvement rate as a dependent variable. The
Multiple linear regression
In this study, we analysed the MRI and clinical characteristics of patients with CSM who had spinal cord swelling and those without, revealing that patients with CSM with spinal cord swelling were younger and had a higher BMI. The anteroposterior diameter and cross-sectional area of patients with CSM with spinal cord swelling were greater than those of patients with CSM without spinal cord swelling. The time from onset to preoperative surgery was shorter and the preoperative MJOA score higher in the spinal cord swelling group, and the postoperative MJOA of patients with CSM with spinal cord swelling was not significantly different from that of patients with CSM without swelling; however, the postoperative MJOA improvement rate was more significant.
In this study, patients with CSM with spinal cord swelling were younger and had a higher BMI, suggesting that the pathophysiology of the spinal cord swelling group was different from that of typical CSM. Little is known about the pathophysiological basis of spinal cord swelling in patients with CSM, but some studies have suggested an association with venous hypertension caused by disturbances in spinal venous circulation [8]. An elevated BMI often indicates the presence of higher lipid levels in patients, and several clinical trials have confirmed that the development of CSM is associated with elevated lipid levels in patients [12], which is presumed to mainly result from a more pronounced obstruction of spinal venous return caused by high blood lipids [13]. Others have suggested that disturbances in cerebrospinal fluid circulation may play a role in the development of spinal oedema [14]. Previous studies have found that the narrowing of the anterior and posterior diameters of the spinal canal and a smaller cross-sectional area lead to impaired cerebrospinal fluid circulation [15]. This study found that the anteroposterior diameter and cross-sectional area were larger in the group of patients with CSM with spinal cord swelling than in the group of patients with CSM without spinal cord swelling. Thus, the role of impaired cerebrospinal fluid circulation in the development of spinal cord swelling remains uncertain, and further studies are needed to confirm this. In addition, mechanical stress caused by cervical motion may be associated with the development of spinal cord swelling. Three cases reported by Sasamori et al. [16] suggest that the development of spinal cord swelling is associated with transient and constantly repeated spinal cord compression. Previous studies have found that the cervical spinal cord can be repeatedly compressed during dynamic changes in the cervical spine and that cervical curvature is directly related to the degree of dynamic changes in the cervical spine [17]. This study identified no difference in the C2–C7 Cobb angle and T1 slope angle for evaluating cervical curvature between the spinal cord swelling group and the non-spinal cord swelling group of patients with CSM, which does not support the theory that cervical motion causes spinal cord swelling. This is consistent with the findings of Chen et al. [18].
Previous studies have shown that approximately 10% of patients with CSM develop enhanced signals in the spinal cord [10]. In this study, 7.8% of patients in the non-spinal cord swelling group exhibited enhancement, which is similar to previous studies [19], whereas the percentage of patients in the spinal cord swelling group with enhancement was significantly higher (31.4%). The pathological basis of spinal cord enhancement in CSM may be related to the local disruption of the blood–spinal cord barrier, local neovascularisation and aggregation of inflammatory cells. All of these processes lead to the increased permeability of the blood-spinal cord barrier, resulting in an abnormal enhancement of the spinal cord [20]. Spinal venous hypertension has also been demonstrated to lead to the increased permeability of the blood–spinal cord barrier [21]. The results of this study also support this theory, with spinal venous hypertension serving as a common pathophysiological basis for spinal cord swelling and spinal cord strengthening; the percentage of patients with CSM who developed spinal cord enhancement was significantly higher in the spinal cord swelling group.
In this study, patients in the spinal cord swelling group had a shorter time between onset and surgery and high preoperative MJOA scores, which is the same as in previous studies [20]. This suggests that the presence of spinal cord swelling in patients with CSM represents a significant short-term deterioration in neurological function. Although there was no difference in postoperative MJOA scores between the two groups, the postoperative MJOA improvement rate in the spinal cord swelling group was significantly higher than that in the non-spinal cord swelling group, which provided a basis for a clinical evaluation of the prognosis of patients with CSM with spinal cord swelling; thus, although the postoperative efficacy of such patients was not significantly different from that of typical patients with CSM, timely surgery significantly contributed to the improvement of their symptoms. This is consistent with the findings of Aditya et al., who found the duration of symptoms to be an important indicator of patient outcome [22]. The only difference between the enhanced and non-enhanced subgroups in the spinal cord swelling group was the MJOA improvement rate after surgery, suggesting that patients with CSM with spinal cord swelling and abnormal spinal cord enhancement should be operated on more promptly to relieve their pain.
The limitation of this study is that the number of patients with CSM included in this study was 115, including 51 cases in the spinal cord swelling group, which is a small sample size; there are therefore inconsistencies with previous studies. In future studies, the sample size and sample source should be expanded to achieve a more diverse study population to further explore the predictive value of MRI spinal cord swelling indicators on the prognosis of patients with CSM. In addition, the improvement rate is a calculated statistical indicator; conducting a multiple linear regression analysis as a dependent variable is not appropriate. If a prognostic factor analysis is needed, the dependent variable needs to be reconsidered. This will be addressed in our next study.
Conclusion
In this study, patients with CSM with spinal cord swelling experienced a shorter time from symptom onset to surgical treatment, more significant preoperative neurological deterioration and more significant postoperative symptom improvement. These findings demonstrate that spinal cord swelling is a reliable imaging indicator for predicting the prognosis of patients with CSM.
Ethics statement
The study was conducted in accordance with the Declaration of Helsinki. The study was conducted with approval from the Ethics Committee of The First Hospital of Hebei Medical University. Written informed consent was obtained from all participants.
Competing interests
The authors declare that they have no competing interests.
Funding
No funding or sponsorship was received for the study or publication of the article.
Author contributions
Conception and design: TXN; Administrative support: ZL; Provision of study materials or patients: LHR and ZXS; Collection and assembly of data: SYC; Data analysis and interpretation: WY; Manuscript writing: All authors; Final approval of manuscript: All authors.
Availability of data and materials
All data generated or analyzed during this study are included in this published article.