
Abstract
Breast cancer has been a worldwide burden of women’s health. Although concerns have been raised for early diagnosis and timely treatment, the efforts are still needed for precision medicine and individualized treatment. Radiomics is a new technology with immense potential to obtain mineable data to provide rich information about the diagnosis and prognosis of breast cancer. In our study, we introduced the workflow and application of radiomics as well as its outlook and challenges based on published studies. Radiomics has the potential ability to differentiate between malignant and benign breast lesions, predict axillary lymph node status, molecular subtypes of breast cancer, tumor response to chemotherapy, and survival outcomes. Our study aimed to help clinicians and radiologists to know the basic information of radiomics and encourage cooperation with scientists to mine data for better application in clinical practice.
Introduction
Breast cancer has been a worldwide burden of women’s health, with an increasing trend in incidence in recent decades. 1 As the concerns of breast cancer have been raised to improve primary and secondary prevention, 5-year survival of breast cancer has increased steadily in most developed countries. 2 However, the efforts for early diagnosis and timely treatment are still warranted to reduce mortality. The concept of Breast Imaging Reporting and Data System has been proposed and widely used for more clear and uniform communication of clinicians and radiologists based on radiographic features to evaluate the classification and gradation of tumors. This classification remains limitations, as it greatly depends on the experience of radiologists. Patients with a suspected breast lesion are suggested to take a biopsy to confirm the tumor nature before the surgery. Although biopsy can provide gold standard of suspicious breast lesions, it still has some limitations. As it is invasive and could not reflect the heterogeneity of the whole tumor that may provide uncertain information of lesions if the tumor size is too large.
Image technologies are the most direct and convenient tools to reflect the size, morphology, and radiographic characteristics of tumors that can be utilized to diagnosis, treatment, prognosis assessment, and so on. New technologies based on different imaging modalities have emerged for precision medicine and individualized treatment of patients with cancer. Since 2012, the concept of “radiomics” was firstly proposed by a Dutch researcher and interpreted as “the extraction of numerous features from radiographic imaging by a high-throughput approach.” 3 Radiomics is a noninvasive imaging technology and has immense potential to obtain mineable data and evaluate whole tumor features of imaging. 4,5 The information hidden from the assessment of human eyes can be used to build predictive models of clinical outcomes and provide a noninvasive and complementary method for tumor genotype. Radiomics has shown promise to be an imaging biomarker of different tumors in clinical practice.
Ultrasound (US), mammography, and magnetic resonance imaging (MRI) are the most common tools for breast examination in clinical practice. In our study, we only focused on the role of MRI in the application of radiomics. The Pubmed, Web of Science, and Embase were searched up to April 2019 by using search strategies. We used Mesh terms (Medical subject heading) “breast cancer” and “magnetic resonance imaging” and “radiomics” or “texture analyses” or “quantitative analyses,” as well as adding free words in different combination for avoiding the omission of the related literatures. In this study, we aimed to provide a comprehensive review which focused on basic information and the application of radiomics for oncologists. In addition, we concluded the major characteristics, such as study design, the number of patients, MRI modality, magnetic field, radiomics features, and outcomes to provide information of the studies which evaluated various clinical applications (Tables 1-5).
Studies on Differentiating Between Malignant and Benign Breast Lesions.

Abbreviations: ADC, apparent diffusion coefficient; AUC, area under the curve; BI-RADS, Breast Imaging Reporting and Data System; ceMRI, contrast enhanced magnetic resonance imaging; GLCM, gray-level co-occurrence matrix; MRI-DCE, dynamic contrast-enhanced; DWI, diffusion-weighted imaging; DWIBS, DWI with background suppression; MRI, magnetic resonance imaging; ROC, receive operating characteristics; T2WI, T2-weighted image; ueMRI, unenhanced magnetic resonanc imaging; 3D-SPGR (RF-FAST), 3-dimensional SPGR(RF-FAST).
Studies on Prediction of Axillary Lymph Node Metastasis.

Abbreviations: ALN, axillary lymph node; AUC, area under the curve; CE2, second postcontrast phase; DCE, dynamic contrast-enhanced; DWI, diffusion-weighted imaging; GLCM, gray-level co-occurrence matrix; GLRLM, gray-level run length matrix; LNs, lymph nodes; MRI, magnetic resonance imaging; SVM, support vector machine; T1WI, T1-weighted image; T2-FS, T2-weighted fat suppression; T2WI, T2-weighted image; NGLDM, Neighboring Gray-Level Dependence Matrix; GLGCM, Gray Level-Gradient Co-occurrence Matrix.
Studies on Predicting Molecular Subtypes of Breast Cancer.

Abbreviations: AUC, area under the curve; CI, confidence interval; DCE, dynamic contrast-enhanced; DWI, diffusion-weighted imaging; ER+, positive estrogen receptor; ER−, negative estrogen receptor; GLCM, gray-level co-occurrence matrix; HER-2+, positive human epidermal growth factor receptor 2; HER-2+, negative human epidermal growth factor receptor 2; MRI, magnetic resonance imaging; PR+, positive progesterone receptor; PR−, negative progesterone receptor; T2-FS, T2-weighted fat suppression; T2WI, T2-weighted image; TN, triple negative; TTP, time to peak.
Studies on Prediction of Tumor Response to Chemotherapy in Breast Cancer.

Abbreviations: ADC, apparent diffusion coefficient; AUC, area under the curve; CoLlAGe, Co-occurrence of Local Anisotropic Gradient Orientations; DCE, dynamic contrast-enhanced; DWI, diffusion-weighted imaging; ER, estrogen receptor; HER-2, human epidermal growth factor receptor 2; MRI, magnetic resonance imaging; NAC, neoadjuvant chemotherapy; NAT, neoadjuvant therapy; pCR, pathological complete response; PR, progesterone receptor; ROC, receive operating characteristics; TN, triple negative; T1WI, T1-weighted image; T2WI, T2-weighted image; HR+: hormone receptor postive; LOOCV, leave-one-out cross-validation; TNBC, triple negative breast cancer; GLN, Gray-Level Nonuniformity; LRHGE, Long Run High Gray-Level Emphasis; LABC, locally advanced breast cancer.
Studies on Prediction of Survival Outcomes in Patients With Breast Cancer.
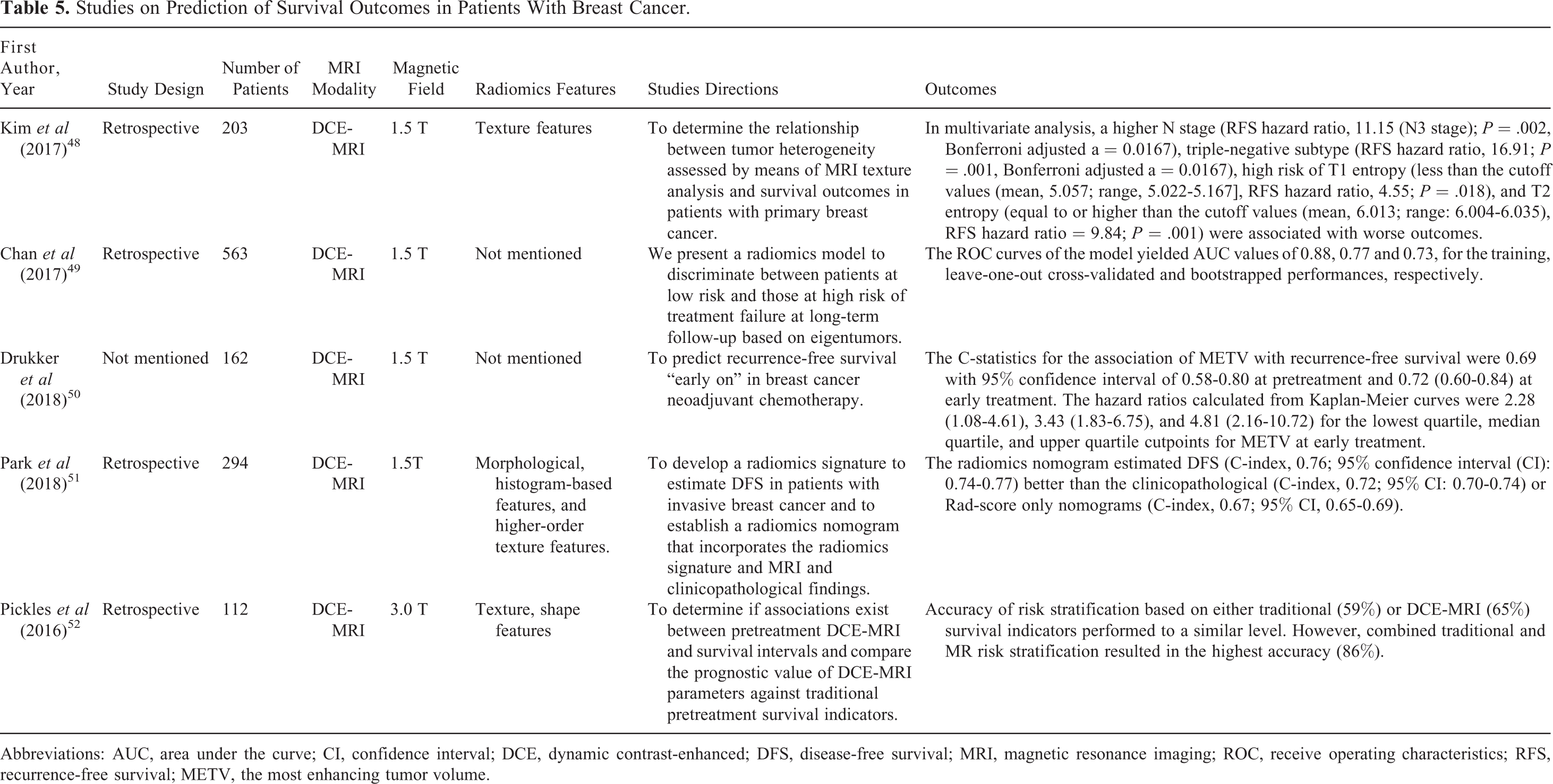
Abbreviations: AUC, area under the curve; CI, confidence interval; DCE, dynamic contrast-enhanced; DFS, disease-free survival; MRI, magnetic resonance imaging; ROC, receive operating characteristics; RFS, recurrence-free survival; METV, the most enhancing tumor volume.
The Workflow of Radiomics
Images from US, computed tomography (CT), MRI, and positron emission tomography (PET) have been widely used for radiomics analysis in scientific fields. Ultrasound and CT provide structural features of tumors, while PET and MRI provide functional and molecular information. Computed tomography was firstly applied in radiomics and then MRI was the second, and these technologies were also the most common modalities in radiomics. 3,4 As the Quantitative Imaging Network guidelines were established by the National Cancer Institute in 2012, the workflow of radiomics included: (1) image acquisition and reconstruction, (2) lesion segmentation, (3) feature extraction, and (4) data analysis. 53
The first step of radiomics analysis is the assessment of high quality and normalized images. Most data of published studies were retrospectively extracted from hospital-based imaging database. It is worth noting that images with different modalities, protocols, and reconstructions from various hospital databases may contribute to some differences in radiomics models. 54 Then the delineation of the lesion is conducted based on standard-of-care images. The whole tumor is segmented by manual, semimanual, and automatic methods. 53 The process of segmentation should be accurate, reproducible, and reliable. Manual segmentation by experienced radiologists is expected to be “gold standard,” however, it is quite time-consuming and not applicable in a large database. 55 Automatic and semiautomatic methods performed better when there are great differences between the lesion and background, and both methods have been developed to improve the accuracy in recent decades. 56
Radiomics features extracted from images are divided into shape, intensity, texture, gradient, wavelet features, and many more. We introduced the most common features that applied in study researches. Shape features are based on the reconstructed 3-dimensional images to assess the geometric characteristics. 55 Parameters from these features include volume, the surface-to-volume ratio, shape, and compactness which are regarded as vital features to evaluate the characteristics of tumors. 57 For example, with the same volume, a speculated lesion has a higher surface-to-volume ratio compared to a round one, which is more probably to be malignant. 57 Although shape can be transformed into a quantitative feature, it is not a specific indicator to distinguish the malignant lesions from benign ones. First-order statistics are dependent on a single-pixel intensity value rather than relationship between neighboring pixels. Tumor intensity histogram-based features are known as the first-order features which include mean, median, standard deviation, kurtosis, skewness, energy, entropy, uniformity, and variance. 57 These features are used to predict the prognosis in the machine learning framework. For example, kurtosis is a measure of whether data are distributed normally. Invasive tumors are composed of more heterogenous tissues that might be reflected by pixel values. 22 Texture-based features are known as second-order statistics and used widely in radiomics analysis to evaluate the intertumoral heterogeneity. It has the ability to distinguish the pixels at different spacing and angles at adjacent or nearest-neighbor pixels calculated by using spatial gray-level dependence matrices. 36 Considering spatial relationships, texture features are divided into gray-level co-occurrence matrix (GLCM), 58 gray-level run length matrix, 59 gray-level size zone matrix, 60 and the neighborhood gray-level size zone matrix. 61 Wavelet features are filter transforms containing the intensity and textural information and regarded as higher order statistic. 62 It shows the spatial relationship among 3 or more pixels. For example, Gabor and Fourier extract spatial or spatial-temporal features, while Co-occurrence of Local Anisotropic Gradient Orientations extract the image voxel an entropy value related to the co-occurrence matrix of gradient orientations. 63,56 Some of these features extracted from region of interst (ROI) may be redundant for a specific task, therefore selecting useful information by using machine algorithms is important in radiomics analysis. Machine learning algorithms include decision trees and random forests, support vector machines, deep neural networks, and so on. 56 Then the selected features, with reproductive, informative, and nonredundant characteristics, are used to evaluate the associations with clinical outcomes.
The Application of Radiomics
Role of MRI
Magnetic resonance imaging of breast is widely applied in screening in high risk women, staging, evaluating curative effect, monitoring recurrence, especially providing complementary information for uncertain findings on mammography and ultrasonography. In recent years, diffusion-weighted imaging (DWI) and dynamic contrast-enhanced (DCE) have been used to provide functional features of breast lesions to assess precise diagnosis. Diffusion-weighted imaging, known as a contrast-free protocol, has been shown promise in the diagnosis of breast cancer. 64 It can reflect tissue microenvironment and membrane integrity through depicting the diffusivity of the tissues. 65 Changes of water diffusion in tissues are associated with pathological processes that can be calculated as apparent diffusion coefficient (ADC). 66 Previous studies have investigated that DWI hold potentials to improve the detection and biological characterization of breast cancer. 67 -69 Based on DWI, several advanced modelling approaches have been evaluated to characterize structural anisotropy (diffusion tensor imaging [DTI]), microvascularity (intravoxel incoherent motion [IVIM]), and microstructural complexity (diffusion kurtosis imaging) for better diagnosis of breast cancer. 66 Diffusion kurtosis imaging extends standard DWI to assess anisotropic details of water diffusion. 70 Mean diffusivity and fractional anisotropy are parameters of DTI to reflect the average anisotropy and the degree of anisotropy. 71 Intravoxel incoherent motion aims to evaluate tissue diffusivity and tissue microcapillary perfusion at once based on biexponential model. 72 The following parameters are commonly used: true molecular diffusion (D or Dt), perfusion-elated diffusion (D*, Dp, or Df), and perfusion fraction (f, fp, or fIVIM). 73 Diffusion kurtosis imaging quantifies non-Gaussianity of the water displacement distribution 66 and has a higher sensitivity and specificity in cancer detection than ADCs. 65 DCE is a contrast-enhanced protocol with excellent sensitivity for the detection of breast cancer and provides functional information about neoangiogenesis as a specific feature of tumor. 74 The sensitivities of detecting invasive cancers by using DCE-MRI are more than 90%, while the specificities range from 20% to 100%. 75,76 In addition, the enhancement patterns of benign lesions were overlapped with malignant lesions. 77 By using conventional imaging technologies, the diagnostic value is mostly depended on experienced radiologists. Thus radiomics with high diagnostic accuracy and applicable value deserves to be evaluated.
Compared to mammography and US, MRI plays an important role in the diagnosis of breast cancer. First, MRI has a higher resolution of soft tissues, which is more sensitive to detect masses. 78 Second, MRI can provide information about the anatomy of the bilateral breast, the relationship between the tumor and surrounding tissue, and lymph node (LN) status. Third, different sequences of MRI could provide functional information of tumors, such as blood flow and breast density, and find the heterogeneity of tumor microenvironments. Fourth, due to the technological limitation of mammography, MRI improves the variations in breast symmetry and masking effect to detect cancer in dense breasts. By using hand-held US, the image quality is mostly dependent on skilled and qualified doctors, while MRI could provide more standard and comprehensive images.
Reliable Differentiation Between Malignant and Benign Breast Lesions
Precise diagnosis for differentiating between malignant and benign breast lesions is necessary for follow-up treatment options. The treatment decisions make a little different, with follow-up for likely benign lesions or surgery for likely malignant lesions. Recent studies suggested that radiomics analysis could provide promising conclusions for the diagnosis of breast cancer and a better discrimination ability than conventional parameters (Table 1). 6 -15 From the included studies in Table 1, area under the curve (AUC) of radiomics models could achieve 0.79 to 0.92, with good performance in differentiating malignant lesions from benign ones. DCE and DWI are the most common modalities for radiomics analysis. Bickelhaupt et al 7 conducted a retrospective study extracting first-order statistics, volume, shape, and texture features from DWI-MRI imaging and suggested that the radiomics model (AUC = 0.91) performed better than other models, including ADC median (AUC = 0.84) and apparent kurtosis coefficient median (AUC = 0.87), moreover greatly increased the sensitivity and specificity of differentiating the malignant lesions from benign ones. However, another study further compared the diagnostic accuracy between radiomics and experienced radiologists. 8 The results showed that by using unconstrained and constrained MRI, expert radiologists (AUC = 0.959/0.959) performed better than radiomics models (AUC = 0.842/0.851). The performance of radiomics was desirable to reach highly experienced radiologists in further studies. Holli et al 9 investigated the texture features to distinguish healthy breast tissue and breast cancer through DCE-MRI. The image selection of DCE-MRI was from T1-weighted precontrast, 2 contrast-enhanced series (contrast first and contrast last) and their subtraction series (subtraction first and subtraction last). The classification accuracy of different breast tissues by using texture features from subtracted images was 100%. Another interesting study based on DCE extracted features from initial enhancement, postinitial enhancement, and signal enhancement ratio (SER) parametric maps for texture analysis. 12 Compared to the initial enhancement map (AUC = 0.767), the SER map (AUC = 0.92) and postinitial enhancement map (AUC = 0.906) achieved better performance. Based on DCE and DWI modalities, Xinhua Jiang et al 11 found the multivariate models, combining morphological and kinetic parameters and ADC values, increased the overall accuracy to 0.90. Some researchers found that background parenchymal enhancement (BPE), which was known as normal breast tissue enhancement on DCE-MRI, could negatively affect the impact of a correct radiological diagnosis in MRI. It might cause increased omission diagnostic rate by obscuring malignancy or increased false-positive rates by mimicking the appearance of breast cancer. 79,80 However, L. Losurdo et al 81 explored some statistical measurements based on full automatized analysis to identify abnormal breast tissue based on BPE to improve diagnostic accuracy for radiologists. In conclusion, radiomics performed high value on the differentiation between malignant and benign breast lesions and increased the sensitivity and specificity of disease diagnosis. In addition, microcalcification is regarded as one of the main indirect signs of malignant lesions. 82 Multiscale texture analysis for microcalcification diagnosis on mammography to distinguish normal/abnormal (AUC = 98.46%) and benign/malignant (AUC = 94.19%) achieved excellent results. 83 However, studies of radiomics focused on microcalcification of MRI need to be evaluated in further research.
Prediction of Axillary Lymph Node Metastasis
The status of axillary LN of patients with breast cancer remains an important role for staging and prognosis. Accurate diagnosis of axillary lymph node metastasis (ALNM) can provide vital information for clinicians to make follow-up treatment plans. The gold standard of confirming ALNM status in breast cancer cases is axillary lymph node dissection (ALND) that is regarded as a surgical process to assess ALN status. 84 According to the American Society for Clinical Oncology guidelines and another randomized clinical trial reports, early stage breast cancer with 1 or 2 sentinels lymph node metastasis (LNM) should not take ALND that may cause a significant overtreatment. 85,86 The sentinel LN is the first site to receive lymphatic drainage from primary tumors, thus sentinel LN biopsy (SLNB) can provide valuable information to guide the follow-up treatment. Therefore, SLNB is used as an alternative method of ALND for patients with early stage breast cancer to predict LNM status with high accuracy. However, both SLNB and ALND are invasive method that may cause potential complications, such as lymphedema, dysfunction of sense, pain, nerve injury, and so on. 84
Conventional imaging examinations to predict LNM is a helpful method to improve accuracy, however, their abilities are limited still with a high false-negative rate. Recent studies investigated that radiomics features to predict LNM greatly improved the accuracy and AUC (Table 2). 16 -21 From the included studies in Table 2, AUC of radiomics models could achieve 0.74 to 0.91, with good performance in predicting LN status. Adding clinical features to the radiomics models, the diagnostic value and AUC of combined models could increase a lot. 19,20 Chai et al 16 compared 4 different sequences of MRI including T1-weighted image (T1WI), T2-weighted image (T2WI), DCE-MRI, and DWI-MRI to find out the best modalities in predicting LN status for clinical practice. The results showed based on morphological and texture features, the second postcontrast phase (CE2) of DCE and the contrast enhancement kinetic features achieved a better performance than others (AUC = 0.91), while radiomics features extracted from other sequence did not outperform the combined models (AUCT1WI = 0.87, AUCCE2 = 0.85, AUCT2WI = 0.79, AUCDWI = 0.85). It is interesting to find that all the features combined from 4 sequences adding kinetics, the diagnostic performance was not differentiated (P = .48). While Dong et al 18 compared 2 radiomics models based on T2-weighted fat suppression (T2-FS) and DWI, the performance to distinguish LNM status of both models was satisfied and the diagnostic value was not different between 2 models (for training set: AUCT2-FS = 0.847, AUCDWI = 0.847; for validation set: AUCT2-FS = 0.770, AUCDWI = 0.787). Most studies concentrated on intratumoral regions, however, peritumoral features have also showed an association with LN status in the predictive models. 20 Further researches focused on the value of peritumoral features should be evaluated. Radiomics was used as a noninvasive and highly accurate method based on mathematical models to predict ALNM and help clinicians to make therapeutic regimens for patients.
Predicting Molecular Subtypes of Breast Cancer
Molecular subtypes of breast cancer were divided into 4 categories based on hormone status by immunohistochemical (IHC) analyses: luminal A, luminal B, human epidermal growth factor receptor 2 (HER2) overexpressing, and triple negative (TN). Cases with positive estrogen receptor (ER+) and/or positive progesterone receptor (PR+), negative expression of HER2, and Ki67 <14% were categorized as luminal A breast cancer, which has a best prognosis. 87 -89 Cases with ER (+) and/or PR (+), HER-2 (−), and Ki67 ≥ 14% or ER (+) and/or PR (+), HER2 (+) were categorized as luminal B breast cancer, which had high-grade tumors and higher proliferation. 87,89 Cases with ER (−), PR (−), and HER2 (+) were classified as HER2-overexpressing breast cancer, which has a poorer prognosis than luminal breast cancers. 87 -89 Cases with ER (−), PR (−), and HER2 (−) were classified as TN breast cancer, which has the poorest survival rate and is related to LN involvement. 87,89,90 The various subtypes have been widely used and involved in treatment planning. However, the molecular subtype is confirmed by IHC analyses on sample tissues that may not reflect the complexity and heterogeneity of whole tumor. Previous studies evaluated the association between MRI features with molecular subtypes, however, the results have not come to a consistent conclusion. 91,92 Different subtypes of breast cancer have their own biological characteristics that can be reflected on the image. For example, HER2-overexpressing subtype was associated with an overexpression of vascular endothelial growth factor, which can increase angiogenesis. 93 HER2-overexpressing breast cancer had a higher enhancement value than other subtypes that could be assessed from radiomic features. In recent years, radiomics analyses have been used to predict the molecular subtypes of breast cancer in many studies, and it can be used as a potential biomarker to differentiate the subtypes of breast cancer with good performance (AUC = 0.74 − 0.92; Table 3) 22 -35 . Fan et al 24 obtained radiomics features and dynamic features from DCE-MRI as well as 2 clinical information to get a predictive model to distinguish luminal A, luminal B, HER2-overexpressing, and TN. By using 24 features, the AUC values were 0.867, 0.786, 0.888, and 0.923, respectively. In this study, the luminal A cancer had low kurtosis and skewness that were related to heterogeneity. High values of these features were also found to be associated with the poor response of treatment in other types of tumors. 93 -95 It was consistent with another study that high-ki67 lesions tended to have higher kinetics. 30 Another study found that texture features extracted from a quantitative ADC map and DCE maps (washin and washout) had the ability to identify triple negtavie breast cancer (TNBC) based on histogram analysis. 35 The models achieved an AUC of 0.710 (TNBC vs luminal A), 0.763 (TNBC vs HER2 positive), and 0.683 (TNBC vs non-TNBC). Intratumoral necrosis was dominant in TNBC, therefore the parameters related to washin were significantly lower compared to other types.
Although DCE-MRI has been used widely in the classification of breast cancer, a problem was found that a certain voxel may reflect various kinetics features due to biological characteristics. Previous studies evaluated the image decomposition methods to identify intratumoral vascular heterogeneity that was proved to be advantageous. 23,25,96,97 Recent studies also investigated intratumor imaging heterogeneity by using new algorithm to separate tumors with varied enhancement patterns for better classification of breast cancer. Fan et al 25 conducted a new algorithm (convex analysis of mixture) to separate tumors with varied enhancement patterns. The results found that analysis of subregions had an improved performance than the entire tumor. The present studies aimed to evaluate the potential association between molecular subtypes and radiomics features from MRI and we found the results were promising in the performance of classification. Further efforts are need before these radiomics models can be used to predict histopathological characteristics clinically.
Prediction of Tumor Response to Chemotherapy in Breast Cancer
Patients with advanced stage breast cancer are treated with neoadjuvant chemotherapy (NAC) to reduce the size of tumors before surgery in clinical practice. Considering the tumor response to NAC, breast-conserving surgery may replace mastectomy which can improve the life quality of patients. 98 However, the heterogeneity of tumors contributed to different responses to NAC, as some cases are insensitive to chemotherapy. 99 Pathological examinations were the gold standard for the assessment of treatment outcomes, and a pathological complete response (pCR) was associated with a long-time survival benefit. 100 Response Evaluation Criteria in Solid Tumors guidelines based on the measurements of tumor size from imaging data have been used widely to evaluate the efficiency of chemotherapy, however, it could not reflect the complexity of biological progress. 101 Therefore, a predictive and accurate marker is expected to be applied in adjusting therapeutic strategies for clinicians and avoiding unnecessary treatment and reducing economic burden for patients. In recent years, some studies reported that radiomics characteristics of MRI were associated with tumor response to chemotherapy and provided great clinical benefits (Table 4). 36 -47 In the included literatures, DCE had been used more frequently (9/12) than DWI (3/12) to assess response to NAC. Dynamic contrast-enhanced-MRI can provide the tumor’s kinetic characteristics of the contrast agent by producing pharmacokinetic maps. Based on quantitative, multiregion analysis that identified enhancement characteristics, the proposed imaging predictors achieved a better performance (AUC = 0.79) than conventional imaging predictors (AUC = 0.53) and texture features on whole tumor analysis (AUC = 0.65). 46 However, the problem that extracting postcontrast images at which time points remains ambiguous. Ahmed et al 36 found that more textural features were significantly different around the 1 to 3 minutes postcontrast time points between groups (based on response, nodal status, and TN groupings). More studies still need to verify the results for making uniform standards for DCE-MRI in the future. A certain category of radiomics features were also used to evaluate their predictive ability for chemotherapy response, such as Riesz wavelets, 47 entropy, 41 and the histogram features. 44 In addition, previous work was focused on intratumoral region to analyze the tumor’s physiological environment, however, peritumoral region surrounded the tumor lesion has also been found to be associated with outcomes. Braman et al 37 combined intratumoral and peritumoral radiomics feature for the evaluation of pCR, yielding a maximum AUC of 0.74 within the testing set. Combining intratumoral and peritumoral radiomics analysis seemed to be a more successful approach to predict NAC. All above studies were concentrated on radiomics features, the clinical information added to the radiomics features seemed to achieve a better performance for prediction. Liu et al 42 built a model named radiomics of multi-parametric magnetic resonance imaging (RMM) combining both multiparametric MRI and clinical information to predict pCR to NAC in patients with breast cancer. The RMM models improved prognostic accuracy than clinical models and radiomics signatures in the primary cohort and other 3 external validation cohort. 42 Quantitative analyses extracted from MRI provide a promising tool for predicting tumor response of patients with advanced breast cancer and show the potential and practical value in the clinic.
Prediction of Survival Outcomes in Patients With Breast Cancer
Survival outcome is one of the great concerns for patients with breast cancer. In previous studies, the characteristics of tumors, such as histological tumor grade, LN status, stage, and some biomarkers are common factors to evaluate the patients’ prognosis. Recently, some studies evaluated the association between survival outcomes of patients with breast cancer and texture features extracted from imaging (Table 5). 48 -52 Imaging features could reflect the whole tumor’s heterogeneity that may interpret differently with survival outcomes of patients having breast cancer with the same stage. For example, tumor with higher entropy and lower uniformity extracted from T2WI and with lower entropy and higher uniformity extracted from contrast-enhanced T1WI had poorer outcomes. 48 Park et al 51 found radiomics nomogram combining Rad-score and MRI and clinicopathological findings estimated disease-free survival better than clinicopathological models in patients with invasive breast cancer. Three GLCM-related features which had different mathematical definitions were selected. They measured various aspects of tumor texture heterogeneity. Previous studies have evaluated the association between imaging features and pCR, however, pCR is not an accurate surrogate end point for survival. Especially for those patients having early breast cancer with breast-conserving surgery, whether chemotherapy could bring patients more benefits for survival than adverse side effects. Chan et al 49 evaluated a radiomics model to distinguish between patients at high risk and low risk with a long-term follow-up based on eigentumor analysis. The eigentumors had potentials to stratify patient survival after 140 months with a hazard ratio of 4.31. 49 Radiomics features for assessing tumor heterogeneity could be regarded as a useful noninvasive biomarker to predict survival of patients with breast cancer and can provide a great benefit for clinical management.
Outlook and Challenges
Magnetic resonance imaging has been extensively used in the diagnosis of breast cancer, predicting malignancy of tumors, staging, evaluating the response to chemotherapy, biopsy guidance, and so on. As the high-throughput data extracted from imaging have conducted a number of “omics” researches. Radiomics of MRI imaging can provide large potential data to characterize the biological features of tumors for precision medicine. Therefore, the utilization of radiomics is hopeful to be an imaging biomarker and noninvasive tool for early diagnosis and evaluation of therapeutic effect in breast cancer. In recent years, genomics, transcriptomics, proteomics, and metabolomics are used to characterize molecular biology of tumors, which were helpful for personalized therapy. 102,103 Although lots of published studies have evaluated the application for years, the association between other omics technologies and radiomics in breast cancer is not very clear and need to be explored in further researches. Integrations of multi-omics studies can greatly increase the accuracy of diagnosis and provide individualized treatment for patients to prolong the survival time and improve the quality of life. Moreover, other new emerging MRI technologies, such as sodium imaging, 104 chemical exchange saturation transfer imaging, 105 blood oxygen level-dependent, 106 or arterial spin labeling MRI 107 are hopeful to provide high-quality imaging for feature extraction.
Radiomics has been applied in scientific research but no widely in the clinic. Some obstacles have existed and need to be improved by the perfection of technologies and methodology. First, the sample size of radiomics analyses plays an important role in predictive models, as the larger samples can increase prognostic accuracy. However, the samples of most published studies are not very large and the models should be validated in further research. Second, because of imaging acquisition from different machines, varied technical parameters and slice thickness, as well as diverse reconstruction algorithms, it is difficult to acquire consistent imaging and get uniform results that can be applied in the clinic. Third, image segmentation includes automatic, semiautomatic, and manual methods. Automatic and semiautomatic segmentation is more convenient for large data, however, the algorithms of segmentation remain to be evaluated. 108 Manual method is time-consuming and the results may be different because of inter- or intrareaders variability. 108
In conclusion, we investigated the workflow and clinical application of radiomics, as well as the outlook and challenges based on published studies. Radiomics has the potential ability of prediction in diagnosis between malignant and benign breast lesions, ALN status, molecular subtypes of breast cancer, tumor response to chemotherapy, and survival outcomes. Radiomics has been widely used in tumor diagnosis and prognosis, however, it is still in the research phase and many efforts should be taken for clinical translation. We also have discussed the limitations and promises of radiomics for improvement in further research. Our study aims are to help clinicians and radiologists to get to know the basic information of radiomics and encourage cooperation with scientists to mine data for a better application in clinical practice.
Footnotes
Abbreviations
Authors’ Note
Our study did not require an ethical board approval because it did not contain human or animal trials.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.