
Abstract
Virtual reality (VR) gaming (VRG) captures, examines, analysis, and renders the game data virtually instead of the users’ devices over efficient networks. E.g., VR is crucial in visually guided surgery and manifold therapies. Video Quality Assessment (VQA) helps VRG software and devices execute high-quality inputs/outputs. This paper debates VRG processes, environments, VQA metrics, Quality of Experience (QoE), platforms, current methods, tools, use in medicine, existing operational gains/challenges, and highlights future directions.
Keywords
Introduction
Virtual Reality (VR) gaming (VRG) has become more popular lately with real sensing, simulating experiences like or fully unlike the Real World (RW) for entertainment, therapeutics, and learning [1, 2]. VR includes Augmented Reality (AR) and Mixed Reality (MR). The VRG niche grows fast compared to other VR products. Worldly, people play VRG to help with depression, physiotherapy, and leisure [3]. VR boomed in 2015/2016 with properly developed products like Sony PlayStation VR, etc. [4]. People reacted joyfully to realistic gaming in 2017 when companies threw gaming advances [5]. VR has opened up horizons for players and removed bounds with today’s VR are quite real. Quality of Experience (QoE) estimates clients’ Game Enjoyment (GE) or satisfaction level with the service provider, e.g., browsing, smartphones (SPs), TV broadcasts, etc. QoE fully caters to services, economics, cognition, behavior, science, and engineering, fixing human musts. It calculates all client fun stages with service delivery [6]in one of two ways: (i) Subjective QoE (SQoE) uses web surveys, interviews, and questionnaires; and (ii) Objective QoE (OQoE) relies on the Quality of Service (QoS) data. User’s QoE still has caveats from VR devices for service providers. Network parameters often affect graphics (CG), e.g., delay, reorder and packet loss, decreasing users’ GE levels [7]. Cost, devices, better CG quality, 2D/3D cloud experience, and better VRG methods vary in the market [1].
Serious games for healthcare are dissimilar from common entertainment games, based on real-world simulation added with motivation, also called serious purpose [8, 9]. The special games are designed and used in every area of professional fields such as healthcare, education, management, military, and other fields. Mainly the usage of SGs are increased in healthcare for diseases like Elm City stories [10], Wii for balance [11], Re-Mission for adolescents and young adults with cancers [12], and so on. SGs are utilized in several clinical trials as involvement and evidenced effectiveness in many diseases like mental disorders, asthma, and cancer. To test the impact of SGs, Bul et al. [13] applied a multisite randomized controlled trial of diseases like attention deficit and hyperactivity disorder (ADHD) in the everyday life abilities of children. The results proved that children’s health with ADHD disease is significantly improved compared to treatment-as-usual on functional outcomes in everyday life. The research proves that SGs are effective in medical education [14, 15] and also have other characteristics such as decreasing the problems of emotions [16], improving skill [17], changing behavior [18], improving the level of the knowledge [19] and so on. The main reason behind people’s attraction of all ages to SGs is that they have features such as immersion, identity, agency or control, feedback, and interaction [20].
VR/AR can aid patients, staff, and caregivers differently in the health domain with Serious Games (SGs) [21, 22]. These stakeholders (users) and their GEs are euphemisms for performing in a prudential setting. Bad streaming and network problems can impair videos and disturb specialists, who have great responsibilities and cannot negotiate a resolution, depth, color scale, and delay [23, 24]. Ideally, user behavior in healthcare must be probed without stressing the people involved to promote well-being. This paper addresses VRG, hi-tech QoE, differences between VR/AR, and how QoE helps VR GE assessment with these contributions:
VRG QoE models, QoE background, and role in assessing user’s satisfaction and GE levels. Differences between 2D/3D VR and AR. Reviews OQoE and SQoE actions and parameters for VRG comparisons and inspect caveats and future work. Distinguishes and talk about open issues for precise QoE estimation in VRG.
Section 2 Methodology, Section 3 depends upon QoE assessment and measurement. Section 4 concerned with VR and its works. Next, Virtual Worlds (VWs), VR, AR, and their uses appear. 2D/3D IFs are developed in Section 5. QoE for VRGs and MR is in Section 6. Section 7 has gauges, tests, gains, and open trials. Section 8 has conclusions.
This type of research is based on systematic reviews that are concerned with serious games for healthcare using virtual and augmented reality assessment. In this research, recent trends have been discussed, and a systematic literature review (SLR) and system mapping study (SMS) are involved.
Research questions
RQ1: What are the VRG QoE models?
Ans: Many researchers work on VRG models and assess those models via questionnaire study.
RQ2: What is the comparative analysis of VR and AR in the healthcare system?
Ans: Yes, the best comparison of VR and AR usage in the healthcare system and highlighted the drawbacks.
RQ3: What is the main purpose of the VR SG in the healthcare system?
Ans: The main purpose of VR SG in the healthcare system is to provide better cures to patients and analyze them with deep care.
RQ4: How does VR work in the healthcare system via serious games?
Ans: Yes, this type of question is well-described in subsection 3.1.
RQ5: What are the open research issues in VR SG healthcare systems?
Ans: Yes, this type of question is highlighted in Section 6, where the most important open research issues have been discussed.
Selection and non-selection criteria
Selection criteria for publication
Selection criteria for publication
This systematic review has targeted well-known journals and conferences published in the English language from 2013 to 2023. The acceptance and rejection of published articles for the SLR appear in Table 1.
Measurement factors of QoE
Published papers searched by these keywords “Virtual and Augmented reality,” “Serious Games,” “Healthcare Games,” “Digital Games,” “Serious games in Education,” “QoE Serious Games Assessment,” and “QoE Models for Serious Games.”
Review tips
Characteristics of published articles in the SLR process
Published articles extracted from the Google Scholar, Elsevier, and IEEE libraries. This SLR only chooses relevant content.
QoE portrays users’ service/application hopes and pleasure, aiding in evolving future performance advances. Academia and industry have recently grasped QoE’s value in applications’ performance and have gone from a purely QoS- to a QoE-based analysis [25, 26]. QoS offers technical measurements but does not handle users’ conduct and service view [27]. The user might still need to improve the performance. Instead, extreme resource allocation is reported, performing suitably at lower resources. So, to allot resources ably and ponder users’ service perception, the ongoing users’ service views must enhance QoE and QoS [28]. QoEAs entail seeing IFs servicing users’ perceptions. Streaming over has delays, packet losses, and jitter creating unique artifacts linked to network faults [29, 30]. So, QoE assessment (QoEA) helps know which damage caused which network artifact/loss. Also, video codecs’ glitches can affect users [31] with certain IFs’ alterations. QoEA practices hinge mostly on the application types. It is vital to consider video applications as Human Visual System (HVS) stimulators and any quality effect impacting vision. Hence, SQoE metrics may target humans and help test, develop, and benchmark services without disturbing people. SQoE needs surveys to get application feedback [32, 33]. Slow, hard, and costly conclusions require many subjects. Otherwise, OQoE uses algorithms that weigh quality via intensive data processing. Objective metrics are thorny and need subjective benchmarks [34].
This paper only studies subjective/objective Video Quality Assessment (VQA) policies. Consumer data aid designing offers and staying competitive. Suppliers rely on clients’ data to improve their services and interest. Many providers track user involvement to evaluate mood. Long-term users are often given similar advice to increase content/resource consumption [35]. Firms ‘revenues increase because users’ perceptions are included in use rather than old objective QoS indicators.
Similarly, QoE modeling aids users by raising their awareness of service quality and seeking market value [36]. A little user complaint or annoyance quickly reverberates across social networks, degrading service providers [37]. More service and market cost information are available thanks to platforms. Unhappy consumers may switch providers, fostering better services at cheaper rates. Many studies [38, 39] link QoE with QoS mathematically. Service providers must integrate SQoE to network-centric QoS to establish effective QoE control and treat all recognized IFs (i.e., QoS, human, contextual, and systemic), as in Table 2.
Proposed QoE framework for VR SG for healthcare
QoE proposed framework for VR SG for healthcare.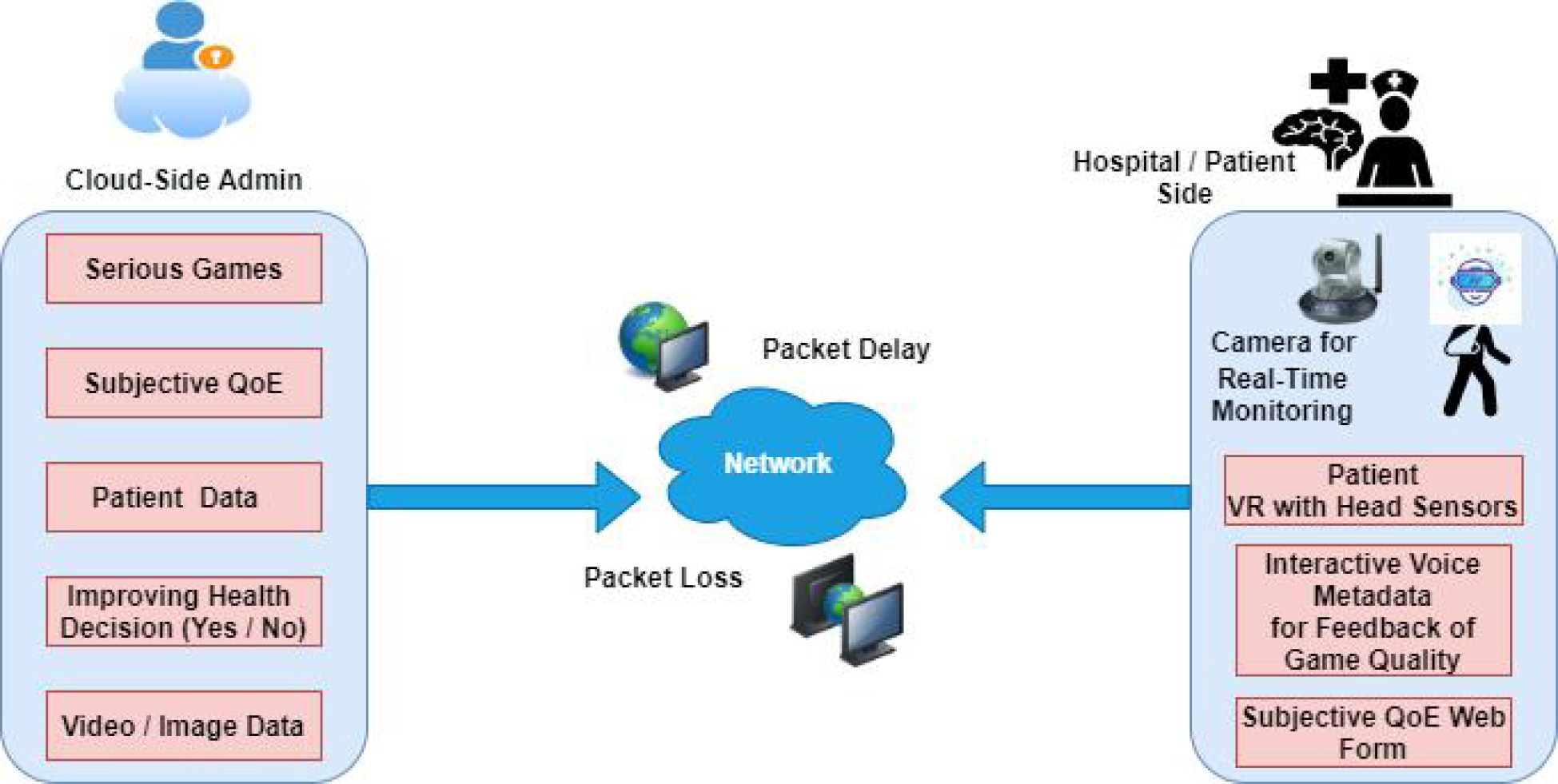
The QoE assessment is important for SG because patients play games from the cloud via the network, and maybe some patients have neurological issues and are color blind, so network delay and packet loss make distortion in SG received by patients and make them uncomfortable [40, 41]. The QoE feature is merged, and a new framework is proposed for the future use of VR for patient treatment via SG. In Fig. 1, QoE proposed framework for VR SG for healthcare is based on the cloud side administration and client-side/patient side. The cloud side contains components such as a serious games database of different games for patients who suffer from different diseases. The subjective QoE database is based on the patient’s feedback, which they give about the quality of SG they received properly; this is based on the ratings and audio and video interviews. An improved health section is added cloud side based on the patient health record and status, and an image/video section based on the data captured from patients’ living/hospital rooms.
The patient/hospital side is based on the video camera, which records the patient’s activities when s/he plays SG via VR. VR patient headsets may be according to technology and vendor. The interactive voice/video section will allow patients to submit their health conditions on the cloud for the doctor to view and suggest further treatment. The web-based interface is also provided to patients to submit their feedback about the SG services from the cloud. The network is middle between the SG cloud service provider and the patient side; the packet delay and loss of service will be degraded in this section because of the dynamic nature of the network [42, 43].
VR means whatever exists but not in RW, and reality means anything that truly exists. An AW made by software (SW) halts beliefs to be taken as RW with VR technology dating back to 1968 [44, 45]. VR covers all that replaces reality but is made via games/fun and contains many other prospects. E.g., driving schools have used VR to train students for actual driving. The two VRG systems’ types appear below.
VR box gaming system
A user operates an SP VR box, Bluetooth controller, and headphones to play and experience the VRG. The player puts the mobile in the VR box and wears this box on the head like goggles. Two convex lenses help convert the SP display to 360-degree angle vision, and SP sensors detect the head’s motion to foster realistic GE and experience VWs [46].
VR studio gaming system
The VRG studio improves VR gaming, so players pay fees and enjoy new experiences. Some advantages of a VRG studio follow.
No wires
It supports 6 players, fully free to roam, so a player does not need to trip over wires [47].
Physicality
VRG uses animated game versions with hi-tech cameras/computers installed in rooms based on users’ height and weight. A robot/SG can interact precisely and reliantly through many areas and degrees of freedom while reproducing health specialists’ “gaming”.
No gamepad or joysticks
Most of the VRG in the studio system handles game players and controls. Players have motion-tracking sensors on their bodies. As they review the game, tracking sensors monitor their motions and computer commands for a real experience [48].
VR/AR tools attract and hold players’ attention. The VR game can be experienced or controlled by the body, letting one move around an Artificial World (AW). VRGs are threefold: Fully-, Semi-, and Non-Immersive. VR technology moves one between places in a believable, interactive 3D AW to explore that reality [2, 49]. VR simulates a 3D scene that lets users interact real or physically using special devices, e.g., a helmet with an inside fixed screen or gloves with sensors. VR devices can show 3600 images, and the user can see his left, right. Up, down and front images are like the RW [50]. After wearing a VR device, users can feel they belong to these movies, games, nature, and whatever they want, but the user is in the same place and going from RWs to VWs
How VR works
Natural reality vs. VR/AR.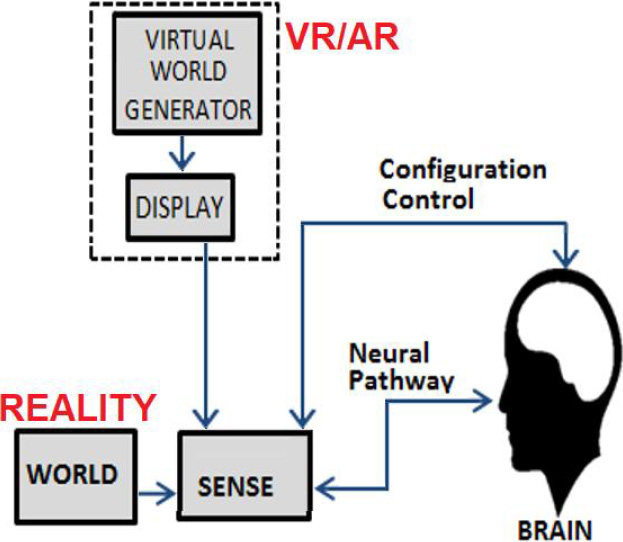
VR/AR in medicine.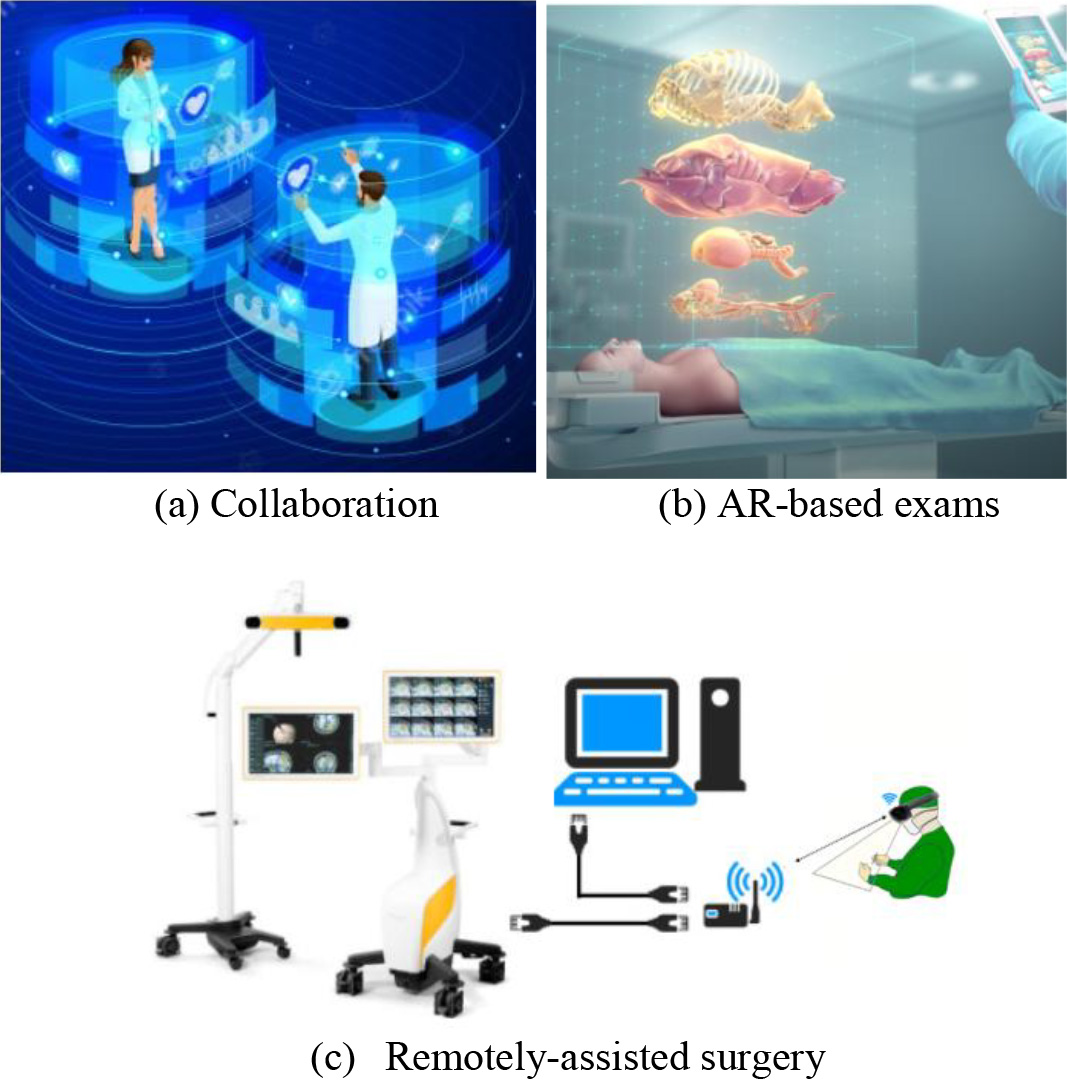
The brain controls configurations, while the sense organ converts natural and synthetic stimuli into neural impulses that go to the brain, as in Fig. 2. A VW Generator (VWG) yields another world users perceive through sense organs and energy-emitting displays mimicking the RW stimulus/sensation [51]. The VWG renderer converts/outputs VW data, e.g., in SP screens and video projectors. Artificial objects to enhance the VR gaming experience can improve healthcare via AR [52]. So, users easily employ VR technology for any VW creation and interaction. Figure 3 shows the collaboration of VR and AR and VR remote surgery.
VR System: The best VR example is playing games where the brain interacts via visual, auditory, and haptic signals. A VR System (VRS) comprises users, hardware (HW) components such as computers headsets and controllers, and RW [53] as below:
HW components can override users’ by tracking their motion. Head tracking, controller actions, eyes/other body parts’ motions are very important. Users have other senses that respond to RW stimuli. VR HW might also track objects other than the user if the interaction is part of the VR experience. Output Data: Output devices must produce an immersive feeling, fitting in visual, auditory, or haptic presentations with the least criticism, and just some of them are upgraded by sound or haptic data. Components: A VRS relies on HW and SW to control varied, immersive 3D user interfaces. Importance: VR offers great degrees of freedom to various groups to reproduce physical nearness. Advantages: (a) Little/no risk; (b) Safety and area control; (c) Realistic scenarios; (d) Retention and recall gains; (e) Simplifies complex problems/situations; and (f) Suits different usability styles. Future: Organizations may use immersion as a key element and make a stride further in their item and administration’s progression. Despite many VR burdens, the market is growing. Disadvantages: VR headsets can strain users’ eyes due to solitary refractive optic components. Data Storage: VR data storing also permits accessing and handling files monetarily for info safety, with front network-attached storage (NAS) frameworks and back storage [54, 55].
VR vs. AR differences
In VR, PCs simulate 3D via high-tech gear. Both are real and tangible. As a result, visual-auditory haptic feedback and somatosensory cortex notes are always enriched by SW-created cortical info [56, 57]. The fast AW growth shows, and technological disparities widen. Image detection use grows hastily, requiring empathy. VW immersion offers isolation, displays better synthetic images without ignoring real life, and boosts AR to connect it to the RW throughout holography. VR tools permit explorations with special fresh dialog tools for listening immersion/users, masks, gloves, laptops, iPhones, enhanced SPs, and corresponding apps. Next, further usage of AR vs. VR technology aspects follow.
Healthcare
AR adds key and alive knowledge to health staff. Surgeons can train before surgery while other specialists assist, diagnose, recover, and rehabilitate people tangibly, aiding what is happening to them [58, 59]. A surgeon’s success and special equipment increase user satisfaction and boost drug expertise. Dental professionals use a 3D IOS printer to reconstruct teeth and prepare for surgery. XR’s virtual needle insertions are key for preparation [53]. In multiple situations, haptic input devices can mimic internal tissues and work with fitness simulations in delicate medical care. AR/VR can compact handheld scanners’ access, which helps broadcast spatial details [60].
Classroom
Trainers utilize many VR platforms to instruct learners on precise facts, including history. VR is useful for gazing at items instead of hearing about them in lessons. Healthcare newbies may find it tough to learn and add knowledge into practice, but VR may assist in various health conditions [61]. Coaches may blend VR trips into classes. AR boosts STEM teaching via 3D versions of organisms, human entities, substances, natural processes, etc. These digital versions can be rotated, zoomed in, and seen from multiple viewpoints by learners, which is an excellent opportunity to learn more about the subject. Learners could build interactive environments with AR 3D objects. Combining concepts offers valuable, enriching experiences that evolve with tech creators to provide a stronger future healthcare role. VR can greatly benefit health degree partakers. Developers might decide if their designs fit the plain text or if any advances are needed. Learners may build VWs with instructional SW displaying simulations and allowing many users to invest time leveraging various elements to create unique VWs/AWs. After inventions wind up, they can explore other options. Classrooms become AR/VR creative training spaces to gain skills, improve teens’ participation in hard tasks, and inspire them to start/change their AWs. Still, not all mentors are device-ready to shift graciously, thus requiring more expertise rather than usual teaching materials. Schools will strive to include/equip new experts to benefit users fairly while keeping things open, cheap, and handy to all.
Comparison of VR and AR
Comparison of VR and AR
Total cost for AR/VR tools has shrunk, rushing health experts/suppliers and caregivers to adopt them. Original goods, imagination-based therapy, etc., aid better, effective illness recovery more simply [62].
Industrial transition
CAD modeling may treat 3D human bodies/shapes [63] and rate wound size, bettering cures. Unique AR/VR results can improve hearing aids. Infrared allows seeing/simulating real-time drug usage. VR can treat hand problems and strain. AR/VR designs also assist impaired patients in moving safely.
Drawbacks
R/VR has drawbacks and benefits depending on how/ why certain companies deploy products. As questionnaires do not identify/itemize drawbacks, the negative health effects of AR/VR follow:
Eye pressure: AR/VR headsets restrict vision to a narrow region. Since one can see and concentrate on details long, blinking is scarce in frequency, drying/ straining the eye’s front surface [64].
VR Sickness: Prolonged use of Glasses and LCD screens raises computer-concentration stress, pain, and blur.
Divinity: 3D VR headers’ effects need not affect amblyopia with impeding focus, false range beliefs, or irregular 3D vision, causing headaches and eye exhaustion.
Safety Reach: The AR game Poker Mongo acts as an intruder invading a garden to track any character and breach defenses. Table 3 compares VR and AR.
2D vs. 3D virtual reality
Google card launching placed VR on SPs to enjoy 3D angles. Gyroscopes are great sensors to pick directions and degrees to watch 360 photos/videos. Gyro sensors locate and move SPs right or left to ratify coordinates [65, 66].
3D technology
Scenes captured have depth, and 3D playback is (a) active, which needs a battery (e.g., the Ammeter sensor can connect TVs, receivers, and glasses to create a 3D image); and (b) passive that usually has rendering/interfacing issues, 3D normally happens without glasses, though health institutions can afford extra HW [67].
2D technology
It captures pictures with a normal camera without depth, but stereo offers some 3D feeling [68].
Stereo projections
Depth counts in 3D medicine and can use one (monocular) and two eyes (binocular). Solving distances may entail extra info. The eye’s focusing muscles’ tension for 3D depth weakens the eye-brain system.
VWs and VGs
VWs date from the 90s, on different sides, and have become personal. More persons’ interactions and presence allow mutable conditions, tools, fun, pursuits, and varying presence levels in VW/AW and game [69]. Many users prefer it mediated 3D VWs, if they look touchable, with nice 3D effects and increasing presence levels.
Arousal
It depicts emotive responses/levels, ranging amply amid high or low points. Different media formats can affect research settings. Many motivated users enjoy gaming, but little arousals distract and deter VRGs’ expert users.
VG attitude
Gameplay attitude estimates handle vital context feelings and views that positively or negatively influence users, depending on objects and how much time is spent.
QoE assessment for VRG
VRG QoEA covers subjective (SA) and objective assessment (OA). Psycho-physiological measures, i.e., ECG, EEG, heart rate, and skin conductance, help [70]. SA includes subjective experiments to collect users’ opinions on a questionnaire, while OAs use VRG logs. The ITU-T SG12 recently defined SA methods for games [71], focusing on three areas: QoE IFs for applications (G.QoE-gaming), SQoE methods definition during gaming activities (P.GAME), and opinion model for games (G.OMG). They open doors for experts and researchers on new assessments and their limits before final advice. Literature on VRG QoEA addressed aspects threefold: 1) identifying and addressing key IFs; 2) subjects’ genders; 3) VRG QoE aspects. IFs could be human-, system-, and content-level. Multiple HMDs targeted VRE, and HMDs device type greatly influences users’ VR experience (VRE). The SA from [72] addressed different HMD headsets’ impact on users. Other HMDs have different VREs, with females feeling more sickness than males. Generally, VRG better the overall GE, satisfaction, interest, creativity, fixation, familiarity, CG, and sound quality compared to desktop.
Summary of VR QoEA aspects and questionnaires
Summary of VR QoEA aspects and questionnaires
HMD devices impact mental responses to cyber sickness and GE. Better technology does not affect cybersickness frequency or severity, and desktops are less prone to it than VR GE. Tryouts showed more GE while using VRG than desktops. Cybersickness restricts VR GE, so major IFs must be known and tackled [2, 70, 72]. Questionnaires help judge IFs. Table 4 recaps these different questionnaires used for VR QoEA, where subjects rate their fear and discomfort levels [73]. Usability means the ease of playing a game with clear goals without users’ cognitive hitch of controls and interfaces. The GE Scale (GES) from the Game User Experience Satisfaction Scale (GUESS) [73] aids in measuring GE. Captivation is a major QoE aspect that shows users feel like they visited VWs, nearly forgetting RWs. Cybersickness seriously affects users’ VRG QoE with nausea or vertigo and worsens over longer exposure or shifting contexts. Stakeholders must feel relaxed performing healthcare tasks.
Delivering high-quality care is vital for Healthcare Systems (HSs) to have effective and patient-centered care. HSs face huge challenges (e.g., complex needs/processes, bigger demands for chronic conditions) and an economic landscape requiring more for less. This work overviews monitoring and improving the telemedicine quality of imaging. Transparency is crucial to support the health needs to meet these demand- and supply-side dares while ensuring financial sustainability. Remodeling HSs and changing cultures is not an easy task, but it involves three areas:
Places
HSs need investments in whole, continuous, coordinated care for patients with complex needs [77]. Building a strong primary care foundation requires investment to create collaborative and high-quality community care services and develop a rich data-transparent infrastructure to monitor and improve quality.
People
Transparency means patients are at the center of care deliverance with maximum quality and efficiency for users in choices and promoting health literacy. Patients’ QoE is pivotal to delivering services that respond to needs [78]. While modernizing health professionals’ roles, patients’ listening and engagement will boost care.
Data/rewards
HSs must invest in proper data and incentives to promote accountability and transparency [79]. Collecting and publishing information around outcomes and quality (rather than inputs/activities), moving to performance feedback, and linking rewards to high-quality care are key in acute financial stress.
Accountability and incentives are chiefly key levers to support quality improvement. Systems should collect more quality indicators around prevention, chronic disease management, elder care, and mental health in primary care. Performance feedback and rigorous open comparisons also permit sharing experiences and ease of learning. Non-financial incentives can enhance the quality of public reporting. Financial rewards are effective when directed towards high-priority areas, e.g., greater chronic conditions management and quality of hospital/mental/long-term care to link payment to quality and outcomes. Empathic and better HSs need more research. Proper and repeated application of the plan-do-study-act cycle should reinforce this, aiming at patient outcomes. Such evaluation should systematically assess policies’ impacts and fill in existing gaps.
QoE impacts several fields and services as per user needs. Still, much research is required for positive QoE on different IFs not considered in VRG studies [80]. There are so many organizations, their VR box for gaming but the quality of the display and cost varies, so which VR boxes provide better QoE? Different platforms, e.g., desktops, mobiles, and the cloud, can offer simple VR gear requiring future QoE research. Cloud gaming gives more GE in the multiplayer scenario with VR boxes. Yet, the CG quality hinders services due to the middle network speed and connection [81, 82, 83, 84]. Researchers still need to address how dynamic network traffic affects CG quality. Future work will focus on network parameters’ impact on the QoE of CG quality of VRG, GE level of user, and the multiplayer scenario game’s speed. This research work can improve the overall QoE for VRG, and organizations will generate more revenue. IFs need consideration, especially since erring may harm humans and at home playing, game café, or traveling, impacting users’ QoE differently. Some users are comfy with multiplayer home playing. Others have more GE when in a café in the multiplayer scenario. The QoE influence on different environments will help manage services for particular users according to their needs. Still, QoE research and novel assessment models are required.
Conclusion
This paper reviews VR gaming QoE Assessment and Measurement for medical applications, analyzing human, systemic, and impact factors for optimal QoE parameters (e.g., throughput, loss, response, delay, frame/data rates, etc.), impacting serious healthcare game users. A systematic review/evaluation of previous gaming models, methods, and designs based on multimedia and network QoE employing key concepts, backgrounds, and subjective/objective QoE to foster further growth is presented. QoE design for data capturing, contextual heterogeneity, curbs, and challenges with future directions, leading the futuristic research to develop efficient schemes, were discussed.
Footnotes
Conflict of interest
The authors declare that they have no conflict of interest.