
Abstract
BACKGROUND:
A growing number of studies of informal carers of older people reveal positive results concerning support via Information and Communication Technologies (ICT). Systematic examination of factors that have a potential impact on carer outcomes are needed to inform future research.
OBJECTIVE:
To explore studies concerning ICT support of adult carers of older people and to identify study characteristics that have a potential impact on carer outcomes.
METHODS:
This integrative review includes 123 studies published since 2005. Fundamental questions for designing sensitive support interventions; ‘who, what, and how’ were applied to a synthesis of the results.
RESULTS:
Identified characteristics from the studies responding to the who question included variables of the carers, such as their relationship with the care recipient or their ethnicity. Characteristics related to the what question related to the types of interventions, and the how question concerned the different services or programs offered, the idiosyncratic needs of the carers, and the types of technologies used.
CONCLUSION:
Results are discussed according to micro, meso and macro levels of analysis. This extensive review can inform future studies and highlight the evidence in the area for decision makers, practitioners and/or NGOs working with innovative forms of support for carers of older people.
Background
There has been a growing global awareness and recognition of the role of informal carers of older people [1]. Informal carers (providing unpaid, regular support or care to a significant other aged 65 years of age or over and hereafter referred to as ‘carer’) may experience negative effects as a result of their caregiving role. This is perceived to be due mainly to lack of time for socialization and psychological stress [2]. Thus, there is a need for relevant, flexible and more individualized support for carers reflected earlier within Nolan and colleagues’ temporal model of family caring [3]. In meeting this challenge, positive results have been highlighted with the use of Information and Communication Technologies (ICT) to support informal carers [4].
Even though a number of review studies have dealt with ICT based support for carers, the present review study differs on a number of counts. Previous studies are mainly directed at carers of a relative/significant other with a specific diagnosis such as dementia [5], or stroke [10]. Alternatively they are directed at a specific aspect such as education [11] or they do not focus solely on older adults [4]. The present review is not diagnosis specific, enables inclusion of people with different diagnoses and focuses solely on adult carers of older adults. Furthermore, the findings from this study intend to focus on study characteristics that have a potential impact or influence outcomes for the carers. To the best of our knowledge, this perspective, has not been reported on in a previous review study. Due to the growing number of studies in the area of ICT based support for carers [4], a comprehensive overview may be difficult to achieve and warrants a systematic examination of the literature.
This study employs an integrative review methodology which is a systematic process of retrieving articles, aiming to reduce, order, categorize and summarize data from primary sources, resulting in a synthesis of the evidence, and presented in a descriptive, narrative format [12, 13]. The main rationale for using an integrative review is that it allows the inclusion of different types of studies (e.g. quantitative, qualitative, theoretical) allowing for a more comprehensive picture of the field to emerge. In the field of carer intervention research, Schulz [14] presented three dimensions for describing complex interventions based on 1.) the primary entity being targeted 2.) the primary function or variable being targeted and 3.) the mode of delivery for the intervention [14]. These dimensions of who, what, and how help to provide a common framework, enabling comparisons between study characteristics and interventions, which may lead to a more comprehensive understanding of complex interventions and thus provide valuable knowledge when developing new approaches for supporting carers via ICT [15]. The present study uses these dimensions as a lens to structure the findings.
Dimensions that have the potential to impact on carer outcomes have been analyzed according to individual or micro-levels, organizational levels (meso-levels) and a level of overall care and systems of social protection (macro-level) [16]. The phenomenon of interest within the present study initially concerns support via ICT products and services that make life easier for carers of older adults, in a broad sense, not only in their role as carers ‘per se’ but also for e.g. having time outside of their caregiving role, and for enhancing the well-being of the carer and the dyad. This clearly reflects an individual or micro-level of analysis. However, our interests also lie in how health and social care services for older people and their carers address carer outcomes (meso level) as well as generalizable results measuring the societal impact of carer focused ICT support interventions (macro level). All three levels of analysis will act as a structure for a discussion of the findings.
The aim of this integrative review is to explore the ‘state of the art’ regarding ICT based support targeted at adult carers of older people and to identify study characteristics that have a potential impact on carer outcomes.
Methods
The literature search was conducted in April 2015 and updated in April/May, and in September 2016. With the assistance of a university librarian, fifteen different databases were initially accessed to reflect the medical, social and technical facets of the research question: AgeLine, AMED, Cinahl, Cochrane, EMBASE, ERIC, Inspec, LISTA, MedLine, Psyc INFO, ScienceDirect, Scopus, Social Services Abstracts, Sociological Abstracts and Web of Science. The search terms were guided by PICOC (population, intervention, controls, outcomes, and context) [17]. We performed searches by subject headings and free-text and used different combinations of search terms such as: caregiver, carer, caregiver support, geriatric, old, elder, dyad, couple, family, informal, telecommunications, computer, communication networks, telecare, telehealth, telematics, information and communication technology, e-health, gerontechnology, online, assistive technology, assistive devices, interactive health communication, health informatics, medical informatics, social media and support. Ancestry searching from the reference lists resulted in the addition of relevant literature.
The inclusion criteria included published, peer-reviewed articles in English, published in 2005 or thereafter, dealing with informal (not professional) adult carers that provided care, help or support to an older adult with any impairment, disability or disease, living in their own home. The support intervention or services used in the study had to be ICT based. All study designs were included. Grey literature was excluded. Exclusion criteria concerned studies where results involved approximately one third or less of the reported outcomes for carers (e.g. due to results that involved mixed groups of people such as formal carers and care recipients). A total of 5061 titles were found in the initial search. After discarding duplicates, reviewing for relevancy and adding the additions of ancestry findings, 121 articles remained in the review.
Even though the focus of this study was on the content and implications of the studies rather than on the studies’ individual qualities [13], we evaluated the included studies using the screening questions of the Critical Appraisal Skills Programme © (CASP) [18]. This was conducted according to the type of study (e.g. qualitative, cohort studies, etc.) and to give us an approximation of the quality of the study. The authors discussed studies that were in doubt to achieve agreement. Three studies were eliminated due to poor quality leaving 118 studies remaining. Alerts from PubMed were generated during the process of this review and used. An updated search was performed in Age Line, Cinhal, Inspec, and MedLine to include September, 2016 and resulted in an additional five articles that fit the inclusion criteria and are included in the final results. (Please see Fig. 1 above). Thus, the results of the review include a total of 123 articles.
Flow diagram of included studies.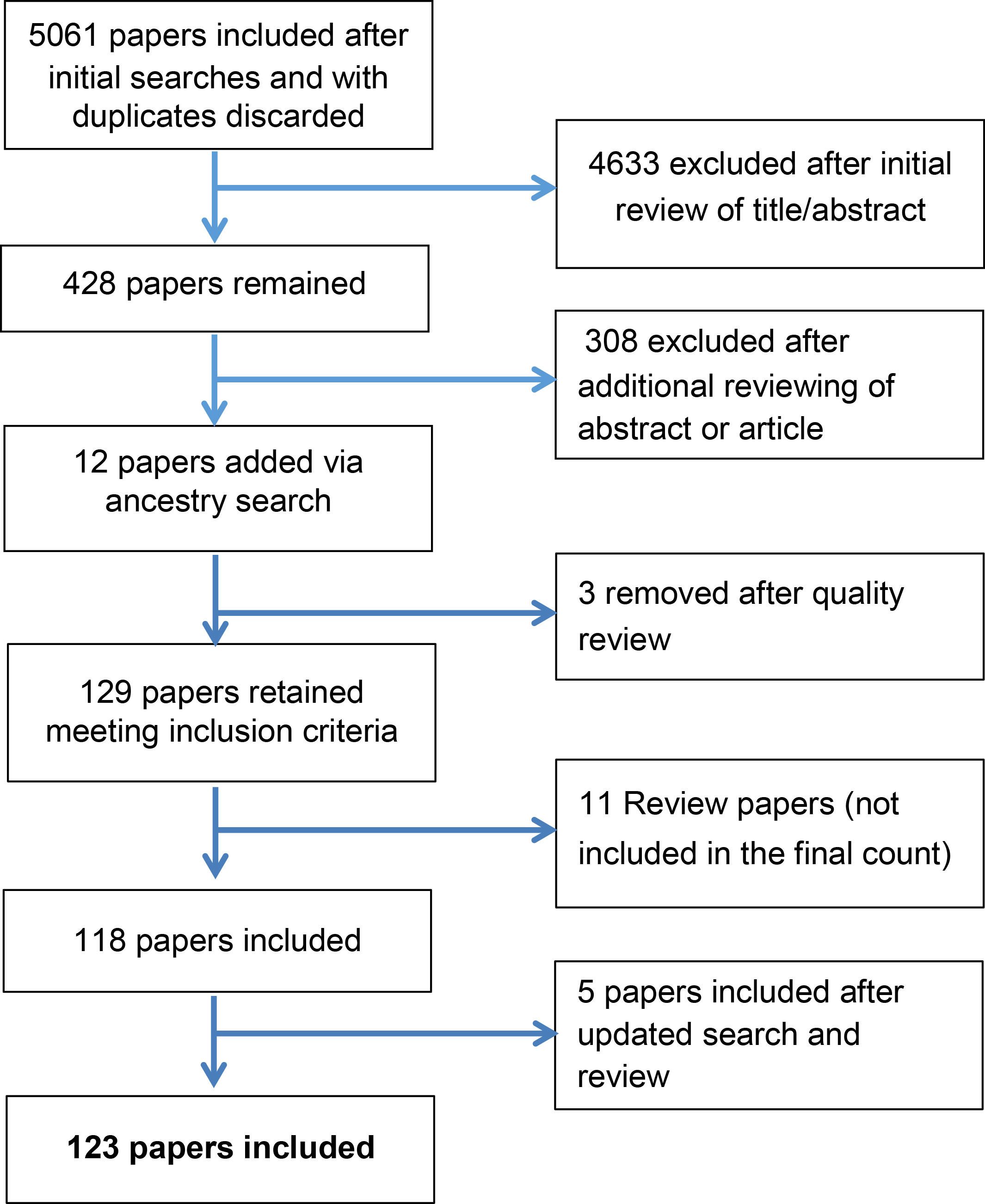
First, we present general study characteristics. We then report descriptive features followed by a presentation of the characteristics that emerged from the analysis and grouped according to Schulz’s [14] fundamental questions, namely ‘who, what, and how’. Given the large volume of included studies (
Overview of the highlighted studies that illustrate the core review findings
Overview of the highlighted studies that illustrate the core review findings
Distribution of the studies by year published.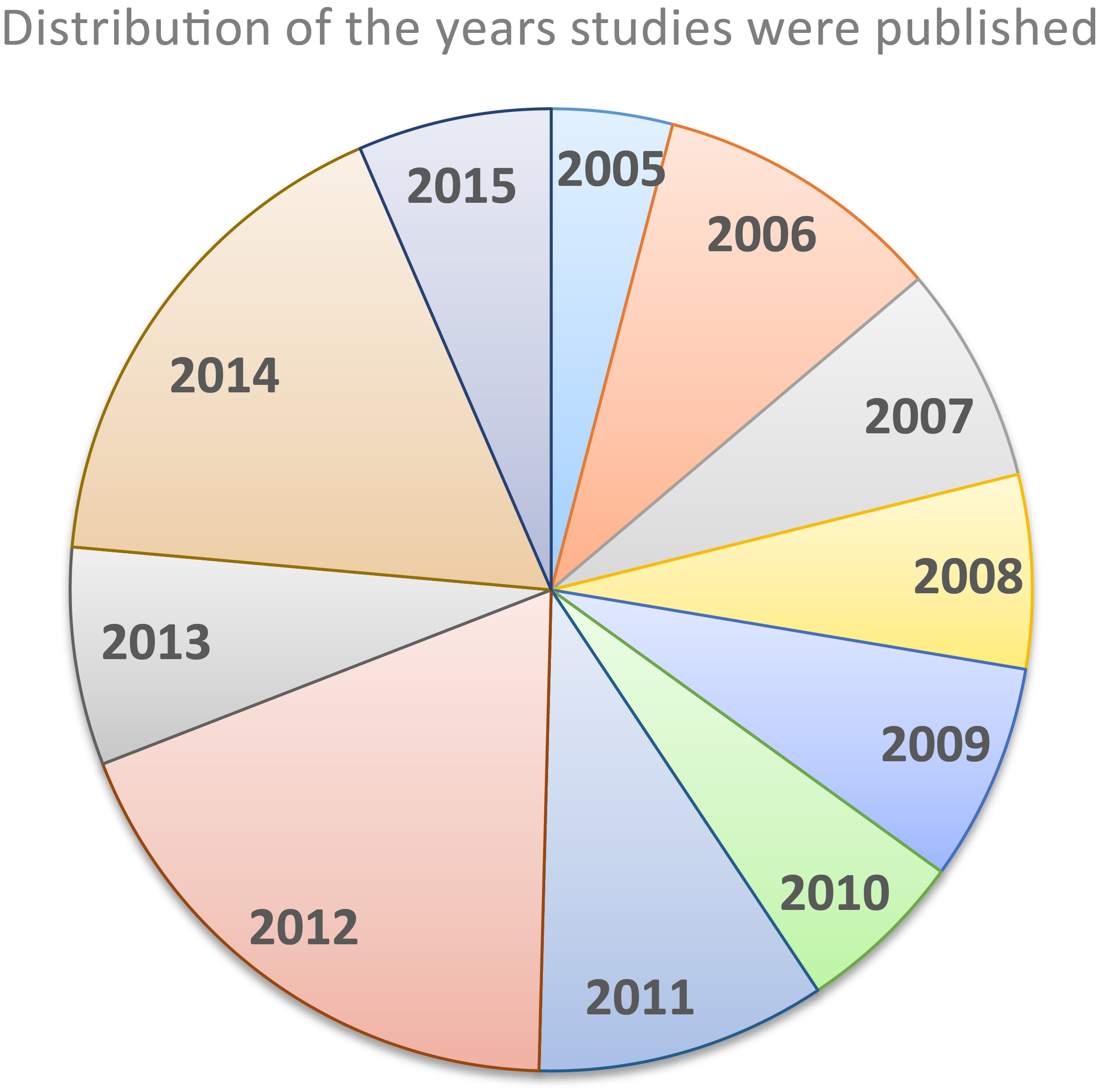
Qualitative analyses were employed in thirty-two studies (26%), thirty-one studies were based on cohorts (25%), thirty-three (27%) were randomized control trials, fifteen (13%) used mixed methods, ten (8%) were based on case control and two articles (2%) were considered as “others” comprising of debates or presentations of systems or ways of working.
The majority of the 123 articles were from the United States (
See Fig. 2 for an overview of the year in which the included articles were published.
Who is the primary entity being targeted?
Descriptions of the carers and care recipients
Female carers dominated the studies, with only two studies dealing with male carers [19, 20]. Approximately two-thirds of the studies reported on the carers’ relationship with the care recipient. Approximately 25% of the studies reported that the carers were spouses, partners or were co-habitating. Carers that were an adult child to the care recipient were represented in approximately eight studies. The carers’ living situation (rural carers) was highlighted in nine studies, and carers’ employment was mentioned in seven studies. The carers’ or dyads’ ethnicity (e.g. Black, Hispanic, Chinese) was apparent in nine studies. Most studies stated the care recipients’ diagnosis. The most common diagnosis was dementia or memory impairment reported singularly in 51 (41%) of the 123 included studies with dementia being represented as one of the other diagnoses in an additional six studies. This was followed by stroke, which was found singularly in 14 studies or in a combination with others in an additional 6 studies. Six studies involved frail older people or chronic conditions and different forms of cancer. Studies also involved carers of people with heart problems, hip fractures, visual impairments and other diseases such as multiple sclerosis (MS) and Parkinson.
Carer variables influencing outcomes
Falling into the realm of who, we found that certain studies grouped different carers together whereas other studies acknowledged the relationships the carers had with the care recipient. This may be an important factor since different groups of carers may influence outcomes. For example, the outcomes of those that were spousal carers differed from those that were adult children to an older person. Spouses expressed a need for more social contacts and to meet other participants, whereas adult children, who were often employed and experienced time constraints, expressed the need for having contact with other carers in similar situations to their own to help normalize their care experience but not to interfere with their busy schedules [21]. The carers’ varying relationships to the care recipient highlights that a general intervention does not necessarily serve both spouses’ and adult childrens’ needs and preferences [21, 22].
Further, characteristics within the carer group regarding race or ethnicity may influence outcomes. A number of studies presented the effects of ethnicity or race on the outcomes [23, 24, 25, 26] or where ethnicity was a factor [27, 28] such as the effects of ethno-cultural-linguistic contexts on the usability of the system [29]. On the other hand, one study claimed that race was not associated with the outcomes, nor did it interact with the effects of the treatment [30].
What is the primary functional domain being targeted?
General characteristics regarding interventions
Falling into the realm of what, the review revealed different types of interventions, broadly grouped as support, information, or education or a combination of these. Some interventions had a theoretical basis which included known therapeutic methods such as Cognitive Behavior Therapy used to target different outcomes such as improving depression [31] or self-efficacy [32].
The most common type of intervention, focused on different types of emotional or psychosocial support, such as follow-up support to assist carers in identifying problems during the transition back home after a stroke [33] or support groups for reducing depression and caregiver burden [28]. Social support was also offered [34] as well as emotional support [30, 35]. Structured counseling tailored to individual concerns and needs, and delivered by a psychologist was also offered [36, 37]. Communication via videoconferencing [38] as well as social problem solving [37], or social networking [39] facilitated social connectedness. A novel program via social media (Facebook) enabled social contacts and was an acceptable method for younger family members [40].
Education and information were also common interventions as a means of carer support [29, 34, 35, 41]. There were many different variations [42, 43, 44] such as websites with education and support [45], information combined with didactic instruction, role playing, problem solving, and skills training [23], or with on-line material, interactive exercises and interactions with other participants and a trained facilitator [46]. Psycho-educational programs were also employed [33, 47, 48].
General characteristics regarding variables or targeted outcomes
A further factor falling into the realm of what had to do with a number of different variables or targeted outcomes directed towards the carers and used either alone or in different combinations in the intervention studies. In total there were approximately 40 different variables used. The most prevalent outcome variable was carers’ level of depression, depressive symptoms or negative mood [31, 49, 50, 51] followed by levels of caregiver burden or perceived burden [21, 52, 53] and subsequently levels of social support and quality of life or life satisfaction [23, 54, 55]. Outcome variables reflected positive aspects such as the carers’ self-efficacy [39, 56] or more neutral outcome variables such as knowledge and use of community services [21].
Individual needs of the carers
Continuing in the realm of what, carers’ individual needs and preferences were characteristics that emerged. Carers expressed their desires for ICT programs and solutions that were more individualized to their specific situation [57]. Carers’ needs varied and included reducing stress, and increasing personal motivation and self-confidence [58]. As well, carers’ requested information that was not diagnosis specific but rather directed towards syndromes with multifactorial origins [59]. As well, the need for encouragement, support and feelings of increased security [60] together with a preference for social contacts [58, 61] or for regaining social inclusion [60] and a need to achieve balance in everyday activities [62]. Likewise, recognition of the role of new technologies to help facilitate living an active life [63]. Interventions specifically targeting the identified needs of the carer were hypothesized to give caregivers enhanced support [64]. Conversely, a lack of knowledge regarding the carers’ unique situation proved to be problematic when providing support [65].
Health care utilization and costs
Studies falling into the realm of what dealt with reduced health care costs or health care utilization. Studies showed that an intervention group used fewer health resources [33] and that decreasing the number of hours per day carers spent in caregiving duties was considered to be cost beneficial [66]. Further, cost savings were achieved, hypothetically preventing nursing home placement [67]. A web-based intervention group showed fewer hospital re-admissions, emergency department visits and fewer nursing home placements, resulting in reduced associated costs [42], and group support education showed a significant decrease in the average overall costs of care per patient, however, this effect was not sustained [68].
How is the method of delivery?
Types of technology
The different technologies used in the studies fall into the realm of how. ICT used to support carers has been classified as those for a.) independent living including e.g. home alarm systems, monitoring systems, telecare, tracker devices, and home sensors, b.) giving remote access to information, such as the internet and telephone-based information, c.) services for support and to help carers’ integration and to maintain contacts, such as online communities offering informal peer-support and d.) the coordination of care through online systems [16]. A number of studies included in this review dealt with technologies for independent living and focused on carers’ perspectives such as use of home sensors [69], tracking devices [38], or for the coordination of care [72]. The vast majority of the included studies dealt with remote access to information and support services directed at carers (b and c above).
Approximately one third of the studies (
Individualized programs
Programs based on assessments of carer needs and preferences and resulting in tailored interventions presented an element of individuality [23, 82]. Even when standardized interventions were offered, individual emphasis regarding relevant intervention domains, enabled individualization [27]. Other studies offered individualized online counseling support for carers [32] or programs that asked carers to create their own individual ‘action plans’ [48]. Even a mixture of modalities (e.g. individual telephone sessions, group sessions) combined with individual goal-setting or risk assessment enhanced an individual approach [53, 54]. Programs offered to rural carers were seen to successfully offer individualized interventions [36, 37, 83]. These interventions were in line with carers’ suggestions for combining programs and services such as therapy and respite [57]. An example of an effective intervention was built on carers’ specific needs and problem severity determined after their level of risk was assessed and thereafter tailored to the carers’ specific needs. The program provided the carers with skills training and support and was seen to significantly reduce caregiver burden after six months [84].
Delivery of the intervention; peers or professionals
The person or persons offering the intervention is a further how characteristic. For the most part, health professionals with various backgrounds offered the interventions. However, in several studies, the support was peer driven. For example, experienced carers were trained and worked as peers, providing weekly telephone support [85]. Health care staff were trained to deliver telephone support to carers [86] and trained professionals together with peer facilitators were used in an on-line support group [87].
Discussion
Identified characteristics deemed to have a potential impact on or influenced carers outcomes and responded to the who question included carers’ relationship with the care recipient or their ethnicity; characteristics that responded to the what question involved different targeted outcomes, the individual needs of the carers and the focus on health care utilization and costs; and characteristics that responded to the how question concerned the different services or programs offered, and the types of technologies used. Due to the complex nature of the phenomenon of ICT based carer support [88], a deeper understanding of the characteristics that emerged from the studies in this review is achieved by discussing them according to micro, meso and macro levels. This perspective is further motivated since there is currently a lack of evidence regarding ICT based services for carers at the meso and macro levels [16]. Potential gaps in the literature, challenges, and success factors that may impact on future research and development will also be discussed.
An important finding of the present study at the micro level showed that certain characteristics of the carer such as their relationship (e.g. spouse/partner, adult child, other family member) and extent of employment), or race/ethnicity appears to makes a difference in the outcomes and this should be considered in planning and analyzing the effects in future studies.
A further consideration at the micro level, concerns the relatively few studies focusing on the caregiver dyad found in this review. Only four studies adopted a dyadic perspective, despite positive results of directing the intervention at both the carer and care recipient [33, 43, 86, 89]. The needs of the dyad being the unit of analysis in carer intervention studies was addressed almost 15 years ago emphasizing outcomes that represent the greatest good for both members of the dyad [14]. This appears to be a plausible request since reciprocal influences of the two persons in the caregiving dyad has been shown in relation to life satisfaction [90]. Even studies addressing challenges for successful outcomes on the level of the triadic constellation (carer, care recipient, and professionals) should also be considered [91].
Regarding the meso level, a number of studies offered multi-faceted or multi-component programs, offering a ‘smorgasbord’ of options to fit personal requirements and preferences. Due to the differing needs and preferences of carers, this may prove to be a success factor and have a positive impact for carers. Studies also presented individualized goal setting or risk assessments. It appears that highly individualized assessment processes and interventions are more likely to achieve desired outcomes compared with those interventions that are more rigid [14]. Offering multi-faceted programs is in line with the results considering the different needs of sub-groups of carers such as those in different relationships with the care recipient or belonging to a different ethnic group and having different needs.
Carers’ individual needs and preferences can be considered at a micro level but should also be seen in a broader perspective. Carers’ unique needs must be congruent with targeted outcome variables, and subsequently with carer interventions (at the meso level). The present review study revealed a multitude of outcome variables. Results of research studies, with planned interventions, controlled variables and determined outcomes, tend to give only small, defined snapshots of limited real-life situations, presenting issues to be considered. First, studies need congruent links between interventions and outcome variables that are based on relevant theories [14]. In some studies, connection to a theory was not presented, making it hard to determine the link between intervention and intended outcome variables. In two studies, the congruency of the intervention and intended outcome variable was diffuse when the provided intervention was directed to a problem that was not frequent in the study population [27, 31]. This can occur when performing research with cross-sectional cohorts and where wide spectrums of participants are included but may prove to be problematic.
Considering the time and resources of both researchers and the potential study participants, it is ethically sound to target interventions to those that need them, and need them the most. Therefore, future studies should help identify especially vulnerable groups of carers and dyads and their needs that they themselves prioritize. In addition, individualized programs, recognized in the results of this study, should be offered. Working together with carers to acknowledge their specific challenges has been shown to be successful by adopting a user participation and user centred design process. Namely actively involving the people that will be using the services to produce acceptability and high levels of usability [92].
Studies focusing on health care utilization or reduced health care costs often relate to meso and macro levels of analysis as they focus on overall care and/or organizational factors. This review found few studies with this emphasis. Carretero et al. [16] argued that further studies operating at a macro level are necessary to ascertain the availability, efficiency and sustainability of ICT based carer support programs. Furthermore, a broader perspective incorporating contextual factors beyond the technological system and models of care need to be explored if the full impact as well as limitations of supporting carers via technology is to be fully understood [93].
Past and future perspectives
The complex interplay of a range of factors in providing support to carers with the help of technology has also been recognized in other review studies [94, 95]. The 2004 review published in ‘Technology and Disability’ discussed success factors for ICT support services, one of the topics being older peoples’ attitudes towards technology [95]. This characteristic was not prominent in the present review and may reflect a growing digitally proficient older population [96]. Nevertheless, measures need to be taken to ensure that those whom are not digitally enabled or empowered are not discriminated against [97]. However, novel technologies or new ways of using technologies as found in some studies in this review will continue to appear and may give rise to new issues of use to be addressed.
To resolve potential accessibility issues it is important for future planners of technology based interventions to identify how technologies are incorporated into the everyday lives of carers and care recipients [93] and to recognize the fit of the technology with the individual or the dyad [98].
Methodological considerations
This study had a broad focus and included a relatively large number of articles. However, we limited the studies to empirical studies published in English from 2005 onwards. By searching in a number of databases, we have endeavored to cover the broad spectrum this subject area encompasses and have included data bases focused on technology, health and social aspects. However, we may have missed relevant work in our sorting process. Nevertheless, our work was conducted systematically and according to the recommendations for an integrative analysis in order to ensure trustworthiness.
Conclusion
Identified characteristics making up the current review results should be considered in future studies since they appear to have an impact on carer outcomes. Future studies should take into consideration carer variables such as ethnicity and the carer’s relationship to the care recipient. Vulnerable groups of carers or dyads should be prioritised and their specific needs and preferences identified. The needs of the carer or dyad should be congruent with the studies’ outcome variables and programs meeting the carer’s or dyad’s needs should be offered. Rapid developments in health and technology combined with an increasing ageing population and need for informal caregiving present challenges that need to be confronted and studied. The present study’s extensive review of recent literature as well as unique focus concerning study characteristics that have an impact on carer outcomes has the possibility to inform future studies. As well, this review highlights the current evidence in the area which we hope will be useful for decision makers, practitioners and or NGOs working with innovative forms of support for carers of older people to make their lives easier.
%section*Acknowledgements
Footnotes
Acknowledgments
This work was carried out as part of a post-doctoral fellowship at the Department of Health and Caring Sciences, Linnaeus University, Kalmar, Sweden.
Conflict of interest
The authors have no conflict of interest to report.